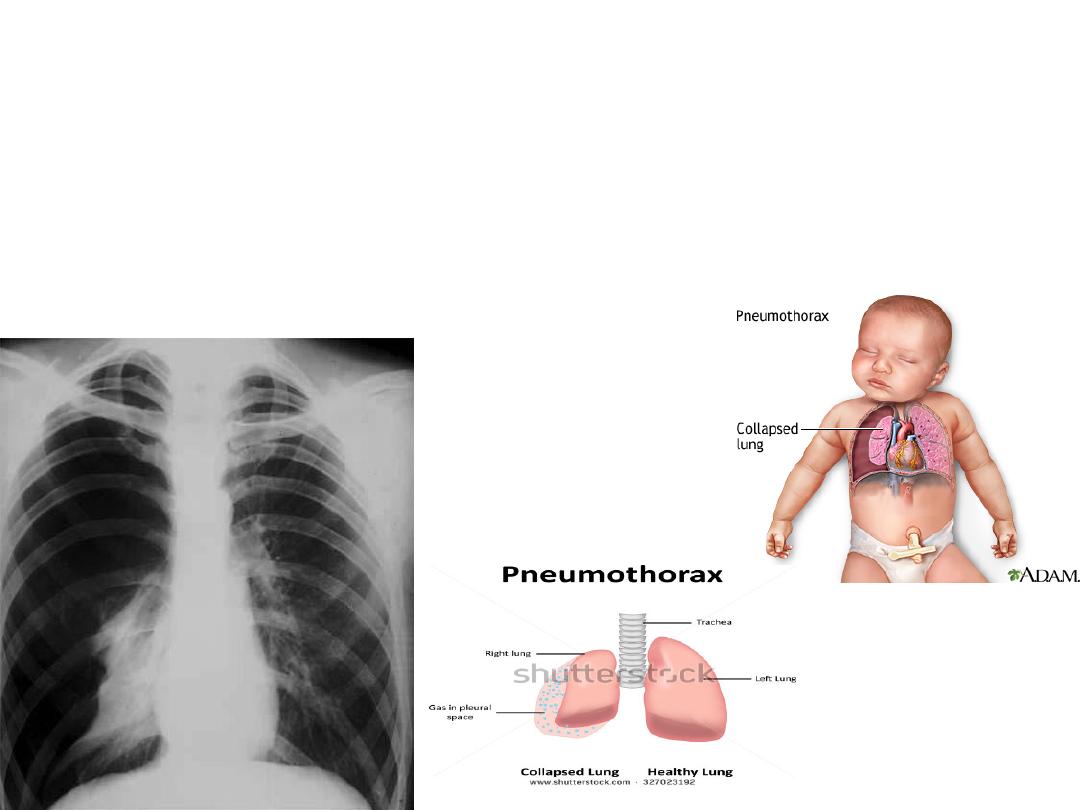
Pneumothorax
dr. Ahmed Shemran Alwataify :
lecture 3
Is accumulation of air gas in a pleural space or accumulation of
extra pulmonary air within the chest which can impair oxygenation
and or ventilation
.(
air can enter the intra pleural space through a communication
from the chest wall as in trauma or lung parenchyma across visceral pleural ) ,
Is uncommon during childhood , may result from external trauma ,
iatrogenic ,pulmonary diseases or mat be spontaneous.
---1---

Causes
:--
1-
chest trauma
2-
iatrogenic *
3–
pulmonary dis as:--
in ----:
asthma ( occurs in 5% of asthmatic patients )
due to rupture of
emphysematus bleb .
pneumonia
:- in connection with empyema ( pyo-
pneumothorax) as in staph pneumonia .
cystic fibrosis
:- occurs in 10-25% which commonly above
10 years of age .
kerosene pneumonitis
4-
collagen disease :-- like marfan syndrome , Ehlar danols
syndrome, histiocytosis
Pneumothorax
may associated with
pleural effusion
( hydro-pneumo
thorax ) or
purulent effusion
( pyo-pneumothorax )
It is common unilateral , while bilateral is rare beyond neonatal period
* iatrogenic ;-
as in complication of tracheostomy , Endotracheal intubation ,
thoracocentesis .
.

ClF :--
severity of symptom depend on
:-- a-
extent of
disease ( extent of lung collapse)
b
-amount of pre-existing lung dis.
The presentation of patients varies depending on types of pneumo thorax and ranged from asymptomatic
to life threatening respiratory distress .
In infancy :-
the S&S is difficult to recognize ( as irritable , dyspnea , cyanosis )
In spontaneous
pneumo-thorax :- may occurs while patients at rest( no clinical sign and
symptoms in primary spontaneous until bleb ruptures causing pneumothorax )
moderate pneumothorax
caused little displaced of intra-thorax
organ caused few or no symptoms .
Extensive pneumothorax
leading to sever chest pain & dyspnea,
&may be diaphoresis & cyanosis especially in children .
Severity of chest pain usually does not directly reflect of extent of
collapse
.
OlE :--
1-
sign of respiratory distress
2-
decreased breath sound on affected side
3-
tympanic by percussion unless associated with Empyema
•
or pleural effusion leading to dullness
4-
shifting of mediastinum to opposite side 5- decreased tactile fremitus
Plus cardiovascular finding
may include the following :----
tachycardia
,
pulsus
paradoxus
and (
hypotension
,
jugular venous distension
which occurred in
tension type ).
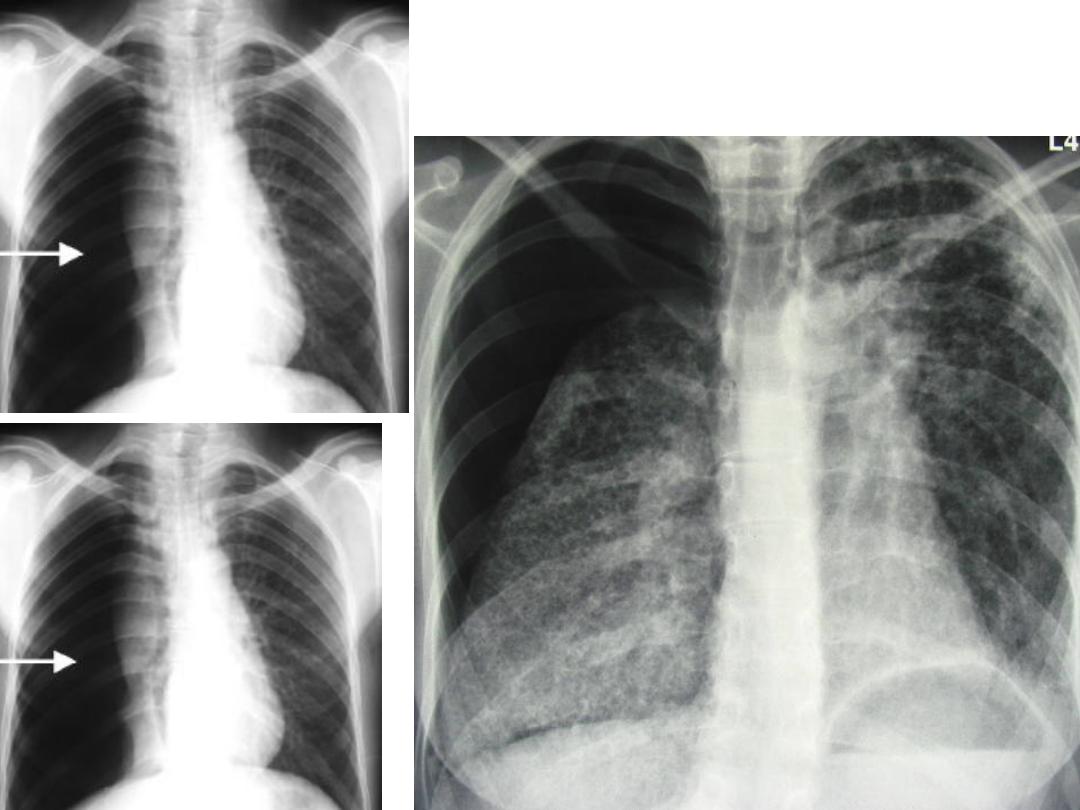
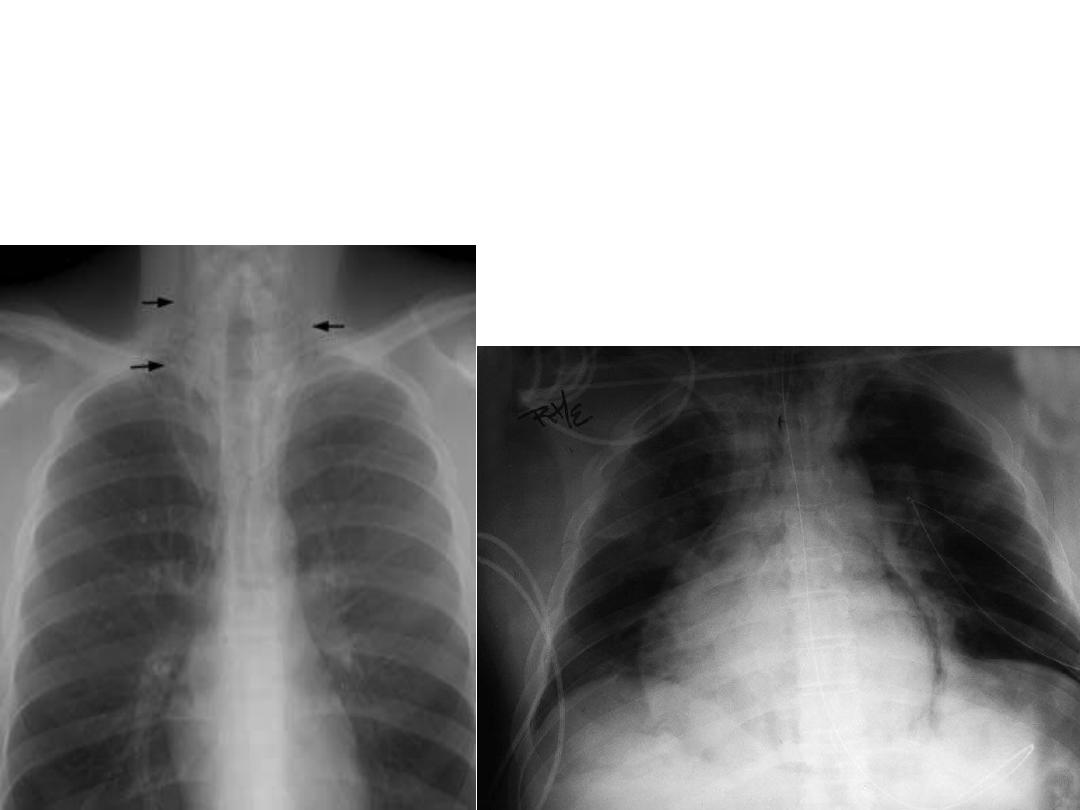
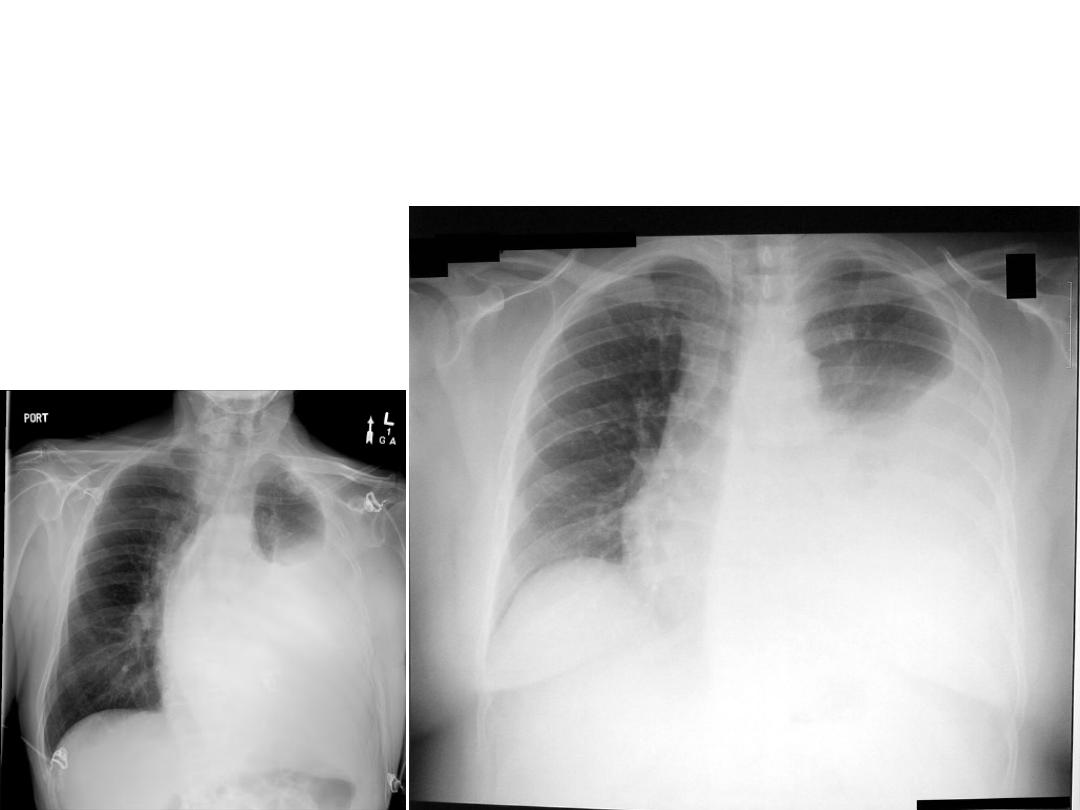
X-rays of pneumothorax
Diagnosis :--
ClF
( history and physical examination remain the keys for the diagnosis )
+ radiological finding
by (
CXR , or sometime used chest CT scan and chest ultra sound )
in infant
translumination of
chest wall helps in rapid diagnosis .
It is important to determine whether this pneumothorax undertension
( tension pneumothorax ) why
:--
Because of causing limitation of contra lung expansion leading to
•
compromise venous return .
Feature of tension pneumo-thorax
:---
1-
respiratory distress , chest pain , distension of jugular vein& or abdominal
distension
.
2-
presence of circulatory collapse
3-
evidence of an audible of Hiss of rapid exist of air under tension with
insertion of chest tube .
4-
mediastinum shifting to opposite site ( sometime no shifting ,if
there is bilateral pneumo thorax or stiff lung of both side )
DD:--
1-
localized or generalized emphysema
2-
cystic fibrosis
3-
diaghramatic hernia
---4---

Treatment :---
depend on extent of pneumo thorax , nature & severity
of underlying disease
:--
1-
if collapse of less 5% ( mild to moderate ) often resolve
spontaneously within one week & increase or hasten resolution
by given high concentration of O2 100% that increased nitrogen
pressure gradient between pleural air & blood .
2-
if collapse is extensive of more than 5% (extensive ) or recurrent
or under tension needs chest tube with air drainage .
Pleurodesis ( is obliteration of pleural space )
is indicated
if
1- pneumo-thorax is
recurrent
, or 2- if the cause is is
cytic fibrosis or
malignancy
.
Pleurodesis is introduction of chemical substance by chest tube into
pleural cavity like tetracyclin or silver nitrate .
3-
treatment of underlying lung dis.
----5---

Pneumo-mediastinum
:
--
is presence of air or gas in the mediastinum , resulting from dissection of air from a leak in a
pulmonary parenchyma into mediastianum (
excessive intra alveolar pressures lead to ruptures of alveoli bordering
the mediastinum where air escapes into the surrounding connective tissues and dissect into further into the mediastinum
.
Causes :---
1-
asthma ( commonest cause
2-
trauma ( penetrate chest trauma , or esophageal
•
perforation )
3-
may associated with dental extraction ,D.K.A, acute
puncture , acute G.E .
4-
idiopathic ( occasionally )
5-
sever coughing
6-
mechanical ventilation
It is rarely a major problem in a children because of air leak going into neck or abdomen
without affection of mediastinum
.
ClF:--
chest pain
( transient stabbing that may radiate to the neck is
principle feature of pneumo-mediastinum )
OlE :--
may be absent or just crunching noise over sternum by auscultation .
DKA(
diabetic ketoacidosis) ,
G.E(
gastroenteritis )
Subcutaneous emphysema if present is diagnostic
.
Diagnosis
is confirmed by chest x-ray which showing mediastinum air
with more distinct cardiac border than normal .
Treatment :-treatment of underlying disease
.
-----------------------------------------------------------------------------

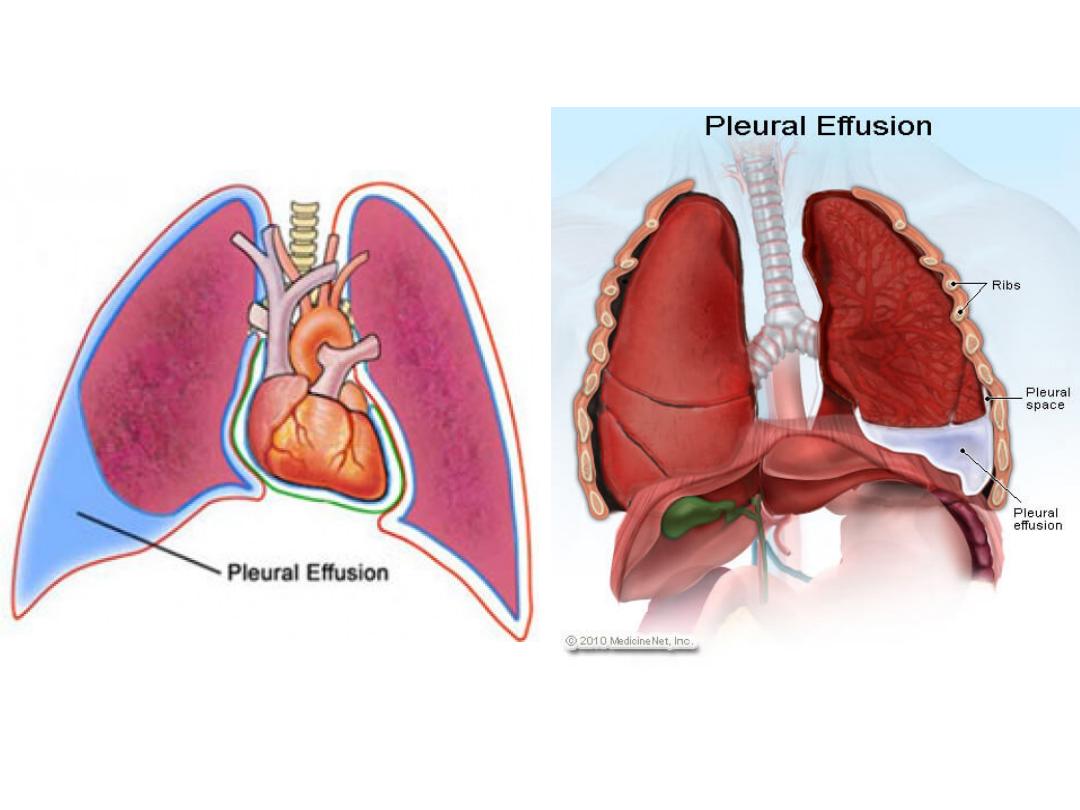
Pleurisy and pleural effusion :--
is fluid collection in a pleural cavity which either serous or
purulent , can be differentiate between them through fluid
aspiration & send for protein , sugar , cell specific gravity,
lactate dehydrogenase (L.D) pleural fluid is of less than 1 cc
between pariatal and visceral layers )
serous
exudate
1-specific gravity
less than 1015 more than 1015
2-protein
less than 2.5gmldl more than 3gmldl
3-sugar
normal less than 60mgldl
4-cell
low cell count high cell count
mainly PMN
5-LD
less than 200 IU/L more than 200 IU/L
6-PH
7.4-7.55
7.3-7.45
Note :--normal PH of pleural fluid 7.6
X-rays
X-rays of pleural effusion
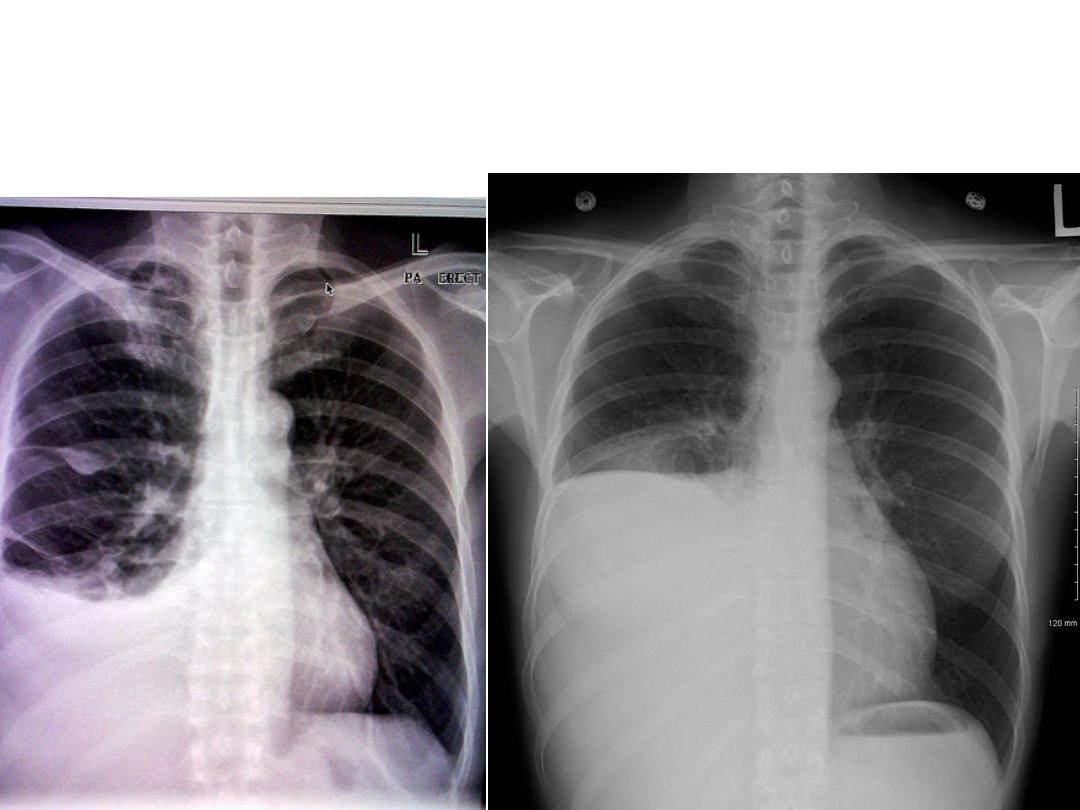
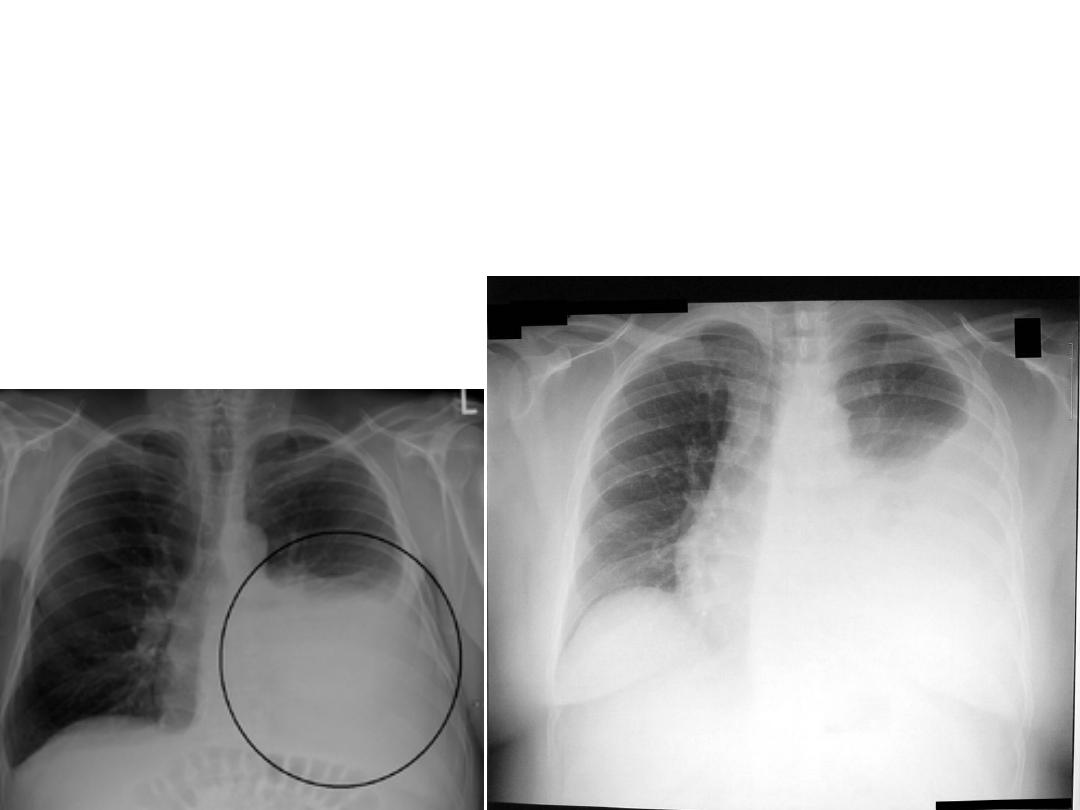
X-rays of pleural effusion
X-rays

The commonest cause of effusion
is bacterial pneumonia & next CHF,
hypoproteinemia , rheumatological causes, metastatic intra-thoracic
malignancy & others like T.B , SLE ,aspiration pneumonitis
infection :---
( parapneumonic effusion & empyema are serious complications of bacterial pneumonia .
Streptococcus pneumonia is most common pathogen ( now it is decreased its incidence by availability of vaccine .) .
Staph aureus is probably the most common caused empyema in children .
Anaerobes have been found particularly in empyema associated with aspiration pneumonia in neurological impaired children .
Pleural effusion occurs in 2-38% of all cases of T.B in children which common in adolescent and is uncommon in the preschool
children
. . .
Pleurisy :--
is inflammation of pleural membrane , classify into 3 type :--
1-
dry or plastic type
2-
sero-fibrinous
3-
purulent type
Dry pleurisy :---
its process limited to visceral pleura with small amount of serous fluid
Causes :--
1- acute bacterial pneumonia & T.b
2- may associated with connective tissue dis. Like Rheumatic fever
3-may develop during course of URTI ( upper resp. tract infection )
ClF :--
cardinal feature is chest pain which increased by coughing , straining , breathing & some time describe as dullache
which less likely vary with breathing , the pain is referred to back , shoulder , responsible for grunting , guarding of
respiration .
x-ray
diffuse hazziness at a pleural space or dense , sharply demarcated shadow
--8--

DD:--
1-
pleurodynia
2-
trauma to rib cage
3-
tumour of spinal cord
4-
herpes zoester .
Note :- any patient with pleurisy + pneumonia should always screened
For T.B .
Treatment :-
treatment of underlying dis. + analgesia NSAID
Sero-fibrinous pleurisy :--
is defined by a fibrinous exudate on the pleural surface & an exudate effusion of
serous fluid into the pleural cavity .
Causes :--
1-
most commonly associated with infection of lung or
inflammatory condition of abdomen or mediastinum .
2-
less commonly associated with SLE, Rheumatic fever ,
lung malignancy .
ClF :---
1-
often proceed by dry pleurisy .
2-
when fluid collection , the pain is disappeared & the patients are asymptomatic .

Note :-
if effusion remain small
:- have only sign and symptoms of
underlying dis., but ,
if effusion become large
leading to resp.
Distress .
OlE :--
depend on amount of fluid
:--
large effusion
: dullness by percussion
in infant
: there is bronchial breathing
Diagnosis :--
1-
ClF
2-
X-ray finding *
3-
WBC
4-
thoraco-centesis
Course :-
effusion is usually disappeared rapidly ( unless fluid collection with exudate) by appropriate
antibiotic .
if persist ( longer ) suspected possibility :--
T.B , neoplasm , connective tissue dis., Empyema
Treatment :--
1-
treatment of underlying dis .
2-
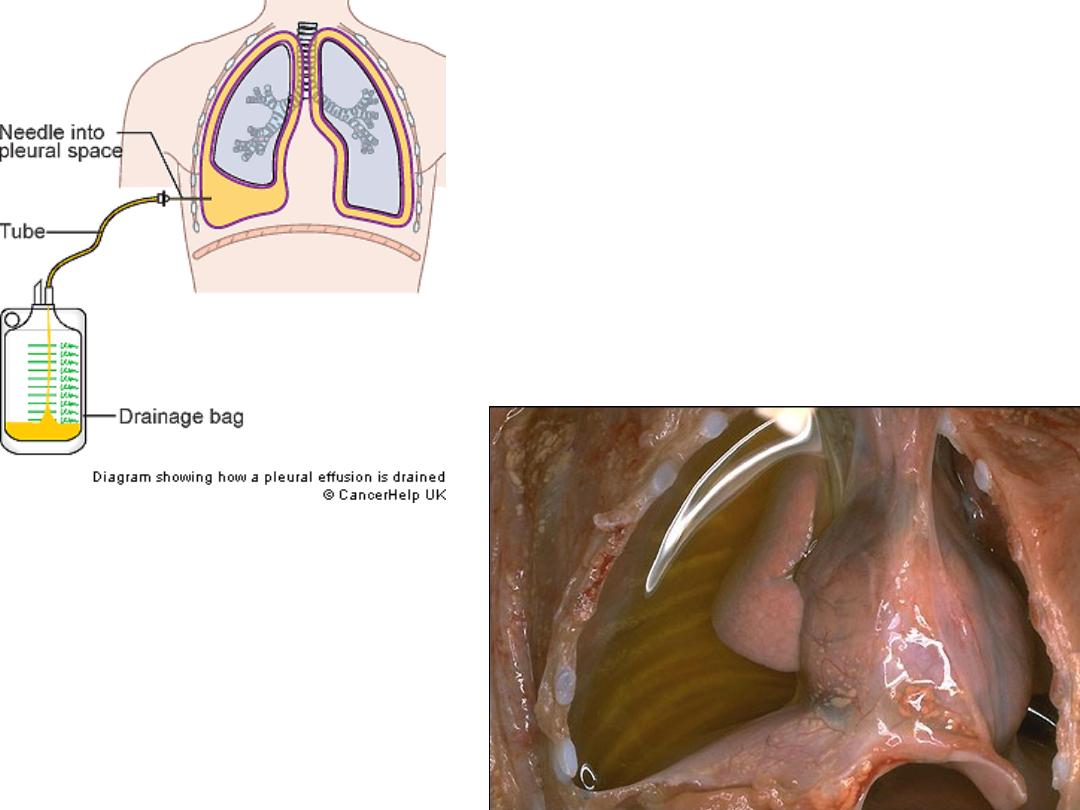
if large effusion , :-needs drainage make the patient more comfortable & removal of not more
than one litter ( if drainage of more than one litter leading re-expansion of pulmonary disease.
if
become purulent
: needs chest tube drainage
*In adult about 50 cc of fluid causes blunting of posterior costophrenic angle recess on a lateral
chest x
ray
, in contrast 200 cc is necessary to blunt the lateral recess on an upright CXR , while lateral
decubitus film is most sensitive view and can detect as little as 5-10 cc of free fluid .
Ultra sound
is superior to standard upright CXR for detection pleural effusion
Chest CT
can easily identified effusion and easily detected presence of empyema but lack the
accuracy required for differentiation of exudates from transudates and chylothorax .

Purulent Effusion :--
is a accumulation of pus in a pleural space , most often associated
with bacterial ( staph infection ) & less frequently with pneumococcal & H.
influenza .
Empyema
is most often encountered in infant & pre-school children
and
is account about 0.6 -2% of children with bacteria pneumonia .
If pus not drained : may dissect through pleura into lung parenchyma
producing broncho- pleural fistula & pyo-pneumothorax
clinical feature :
--present with clinical feature of bacterial pneumonia with acute bacterial
response , pleuritic chest pain, cough , dyspnea and possibly cyanosis , may associated with
abdominal pain and vomiting due to inflammation of pleural space ..
OlE :--
most frequently in infant & pre-school children
And up to 86%of children with necrotizing pneumonia
1-
interval of few days between onset of bact. Pneumonia & empyema if not treated well .
2-
fever in most of pts
3-
respiratory distress
4-
if fluid is not shifted with change position ,
indicated loculated empyema which reverse to serous effusion that shifted with change position .
Thoraco-centesis
should drained as much as possible & send for protein , sugar , cells , lactate
dehydrogenase , specific gravity
gram stain
&
culture
The effusion is empyema if bacteria are present on gram stain ,ph of less than 7.2 , PMN of more than
100000/µL
-11-

CX:--
1-
broncho-pleural fistula & pyo-pneumo-thorax
( commonest cx)
2-
others like purulent pericarditis , pul abscess , peritonitis
& osteomylitis of ribs
3-
septic cx like meningitis , arthritis , osteomylitis
4-
septecemia ( occurs infrquently with staph , is often occurs by H-
influenza & pneumo-coccal .
Treatments :---
1-
pus drainage ( continue for about one week even small amount of
pus , when no longer drained , removed chest tube )
Like methicicline for staph , pencilin or ceftriaxone for pneumococal
2
(
-A
.B
(
and if
resistance , given vancomycin) & ceftriaxone or cefotaxime or ampiciline plus chloromphenicol
for H.influenza
duration of antibiotic : staph for 3-4 wks
3-
if pneumatocelle ; no treatment unless sufficient size which embrass
respiration or secondary infected ( treated by surgery )
4-
instillation of fibrinolytic agent into pleural cavity ( promote
drainage, decreased fever, less for surgical interference , shorten
hospitalization
like streptokinase 1500unit / Kg in 50 ML normal saline for 3-5 days or
urokinase 40000 unit in 40 ML of normal saline twice for 3 days
.
Thank you
note :-- A.B (
antibiotic) Cx ( complication )
--12-