1
Polyhydramnios
Definition :
Polyhyramnios is an abnormally excessive
amniotic fluid volume ( usually 2000 ml ) .
Incidence :
1 % of pregnancies .
Types :
I. Chronic hydramnios
: It usually occurs over
many weeks . This is the more common type .
II. Acute hydramnios : The accumulation is quite
rapid in progression especially in association with
uniovular multiple pregnancy .
Causes :
I- Fetal factors :
1- Congenital fetal malformations : The greater the severity of polyhydramnios the
more likely is it that the fetus will be abnormal . The most commonly seen
malformations causing polyhydramnios are :
a. Central nervous system abnormalities :
i- Anencephaly ( most of cases ) : Due to inability of the fetus to swallow
( principle cause ) , transudation from the exposed meanings , proteins
which result in increased osmolality , and fetal polyuria from lack of
antidiuretic hormone .
ii- Hydrocephalus ( mostly due to the associated abnormalities ) .
b. Alimentary obstruction ( mechanical or functional inability to swallow and
absorb fluids ) .
2- Multiple pregnancy : Polyhydramnios may occur in one or more sacs .
Polyhydramnios in uni-ovular twin pregnancies is specifically associated with
interconnecting vascular systems through the placenta . An imbalance of
pressures between circulations seems to result in one fetus becoming dominant
and fluid accumulates in the single sac .
3- Hydrops fetalis : Polyhydramnios associated with hydrops fetalis is a reflection of
the generalized edema which affects the placenta as well as the fetus ( cardiac
failure and lowered plasma protein concentrations ) .
4- Chorioangioma of the placenta is an uncommon but well documented cause of
polyhydramnios .
II- Maternal factors :
1- The only common maternal condition is uncontrolled DM . The cause of the
polyhydramnios is uncertain and probably due to interplay of several metabolic
factors , including increased growth hormone . There is no direct relationship
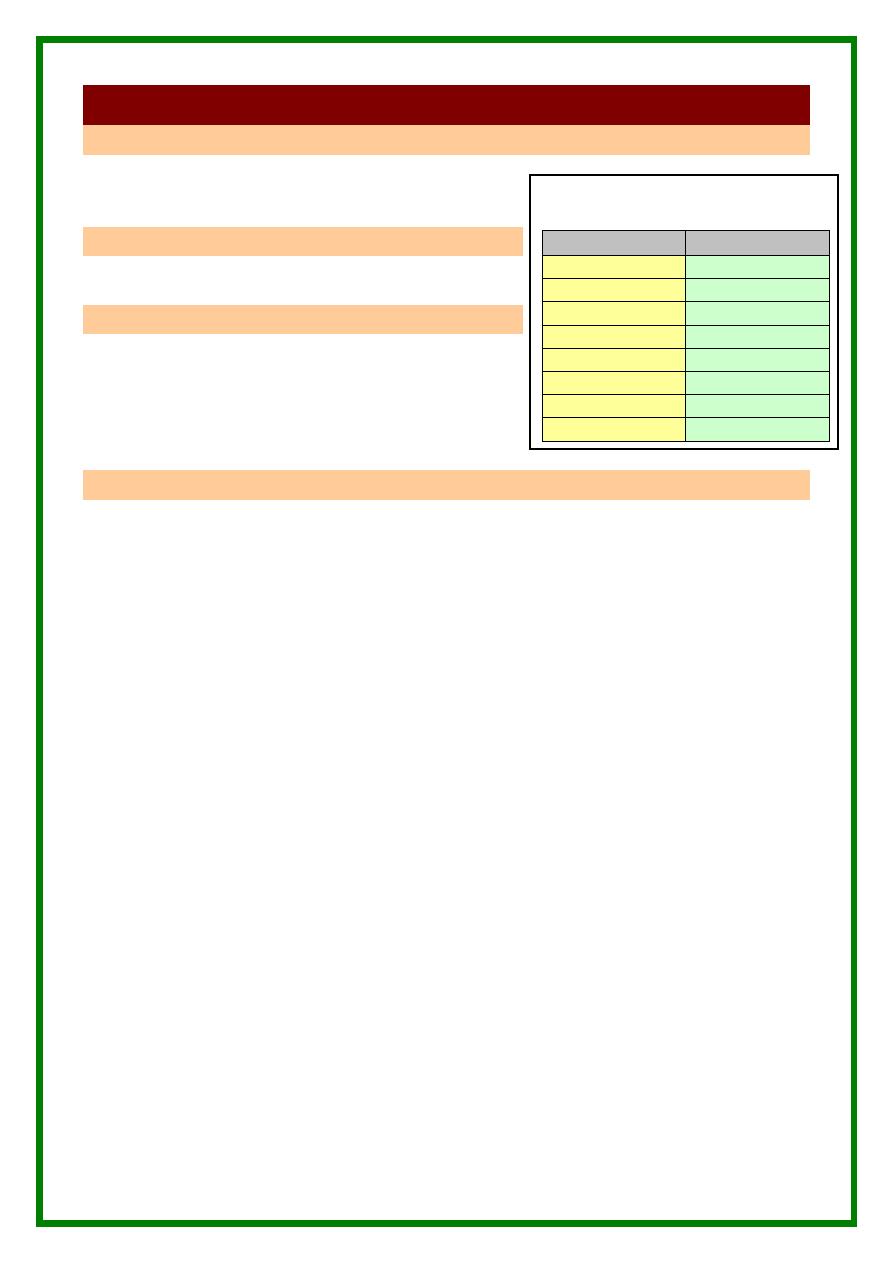
Normal amount of AF
in relation to the age
Age ( Ws )
Amount ( cc )
5
10
10
30
20
300
30
600
36
1000 – 1500
40
850 – 1000
42
250
> 42
< 250
2
to the duration of the disease or maternal insulin requirements , but fetal size
appears to be related .
2- Maternal infection causing fetal infections .
3- Generalized maternal edema .
III- Idiopathic :
Complications :
1- Preterm delivery .
2- PROM with increased risk of accidental hemorrhage , cord prolapse and IAI .
3- Preeclampsia ( why and when ? ) .
4- Malpresentations .
5- Uterine inertia .
6- Obstructed labor .
7- Increased risk of operative delivery .
8- Postpartum hemorrhage .
9- Postpartum infection .
10- The overall perinatal mortality is approximately 50% mostly from congenital
anomalies .
Diagnosis :
Suspicion of polyhydramnios usually arises
from observation that the abdomen is larger
than is appropriate to the gestational dates .
The uterus is often tense and a fluid thrill
may be elicited . The fetal parts may be
difficult to identify and malpresentations
are common . In gross cases , the fetal heart
is not readily audible .
In severe cases , excessive distension of the abdomen will lead to abdominal
discomfort , indigestion , respiratory embarrassment , aggravated varicose
veins and hemorrhoids and dependent edema of the legs and lower abdomen .
Increased AF index by U/S examination .
On radiological examination there is a hazy appearance and the fetal limbs are
usually extended .
AF prolactin level is expected to be elevated for the gestational sage ( under
trial ) .
Differential Diagnosis :
1- Causes of oversized abdomen .
2- Causes of oversized uterus .
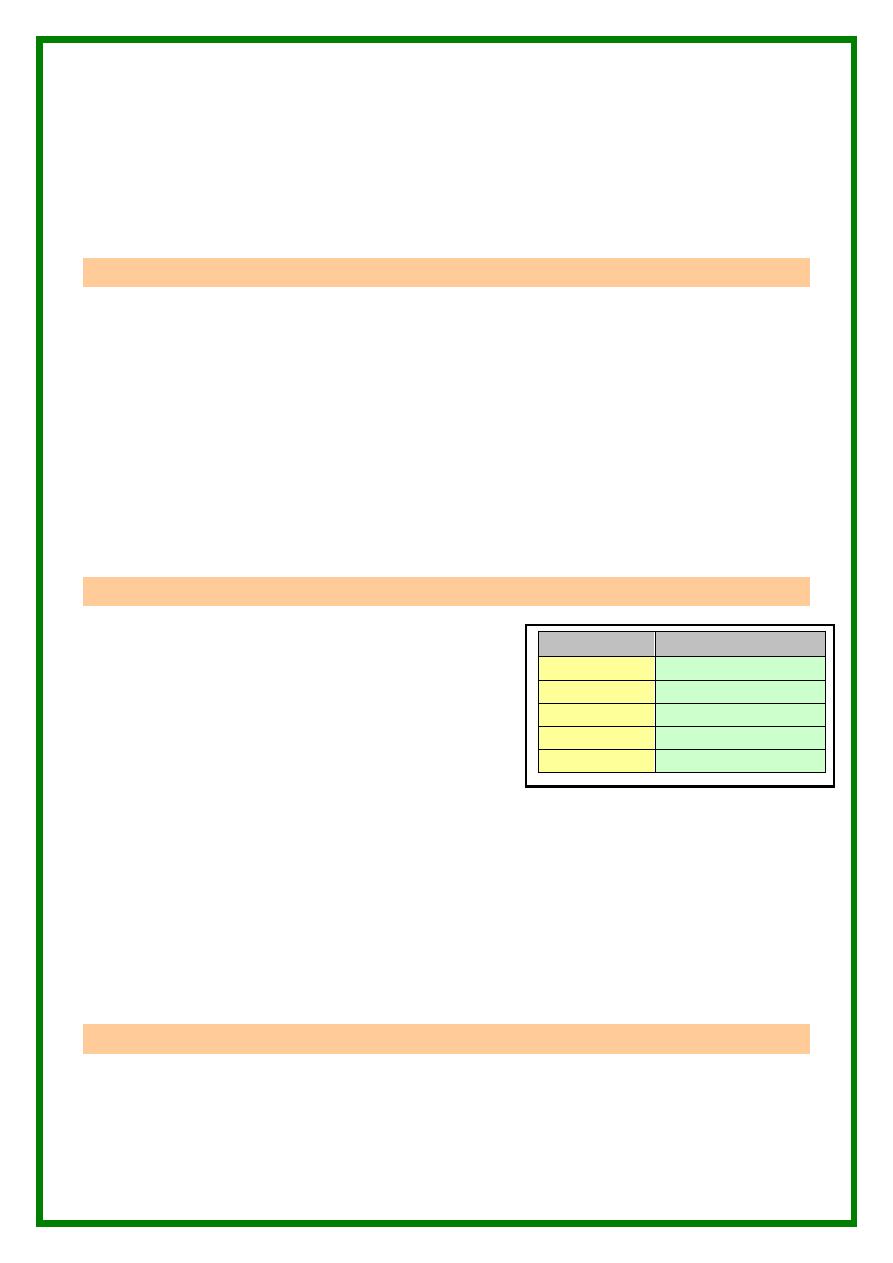
Index
Diagnosis
> 5 cm
Oligohydramnios
5 – 10 cm
Decreased index
10 – 15
Average .
15 – 20
Increased index
> 20
Polyhydramnios
3
Treatment :
I- If there is lethal fetal congenital anomalies TOP despite the type of hydramnios
or fetal age . Try always to perform hindwater rupture of membranes to allow slow
drainage of liquor ( to improve the quality of uterine action ) and to avoid sudden
rupture of the forewater ( to avoid premature placental separation ) . Give
prophylactic antibiotics after ROM .
II- If no lethal anomalies ( hopeful baby ) :
1- If the fetus is > 37 Ws or L/S ration is > 2 TOP . Try always to perform
hindwater rupture of membranes to allow slow drainage of liquor ( to improve
the quality of uterine action ) and to avoid sudden rupture of the forewater ( to
avoid premature placental separation and cord prolapse ) . Give prophylactic
antibiotics after ROM . CS is indicated on the general obstetric indications .
Abdominal binder is recommended by some to prevent splanchnic shock after
delivery .
2- If the fetus is preterm , try to prolong pregnancy till fetal maturity . Cases with
tolerable maternal discomfort needs no intervention and pregnancy usually
passes normally till labor . In cases with severe maternal discomfort , the
following measures can be done to effect relief :
a. Amniocentesis : Aspirate 1-2 liters slowly ( 500 ml/hr ) to be repeated
till fetal maturity . This procedure gives temporary relief and is
potentially risky ( complications of amniocentestis )
b. Indomethacin :
* Reduce the AF by :
i- Decreases fetal urine output .
ii- Decreases pulmonary fluid production .
iii- Increases absorption by the fetal lung .
iv- Increase fluid movement across fetal membranes
* The initial studies report effectiveness without adverse fetal effects
( specially premature closure of the ductus arteriosus ) .
3- Management of the newborn : A pediatrician should always be present at the
delivery unless there is evidence that the fetus has a lethal abnormality . Many
infants are premature and infants of diabetic mothers , although large , require
treatment similar to premature infants . Every effort is done to diagnose
congenital abnormalities , anemia , hyperbilirubinema , sensitized RBCs in
Rh-ve mothers , neonatal infections .
Prognosis :
In the case of fetal abnormalities , the parents should know the risk of recurrence
of the abnormality and the possibility of early antenatal diagnosis in subsequent
pregnancies .
4
Oligohydramnios
Definition :
Oligohydramnios is a reduction in the volume of amniotic fluid sufficient to cause
fetal abnormalities or affect the progress of pregnancy ( usually < 500 cc at term ) .
Incidence :
Different according to the etiology .
Causes :
I- IUGR .
II- IUFD .
III- Congenital abnormalities with either failure of urine or obstruction causing
inability to void urine .
IV- PROM .
V- Idiopathic .
Complications :
1- Malpresentations .
2- Fetal deformities due to abnormal external pressure or AF circulation
( torticollis , pulmonary hypoplasia , hip dislocation , talipus , short limbs ) .
3- Amniotic bands .
4- Complications of PROM .
5- Increased risk of cord compression .
6- Prolonged labor .
7- Increased risk of operative delivery .
Diagnosis :
In many cases the diagnosis is difficult , but the following may help :
1- Small sized uterus ( Decreased fluid volume and / or IUGR ) .
2- The fetus is in an attitude of hyperflexion and , fetal parts are often difficult to
define . Breach presentation is a common feature .
3- U/S examination reveals decreased amniotic fluid index . Amnioinfusion may be
needed to enhance the picture for diagnosis of congenital malformations .
4- Radiological examination confirms the hyperflexed attitude and to the unwary this ,
together with the small size of the baby , may be interpreted as evidence of
intrauterine fetal death , but the other radiological features intrauterine death are not
evident .
5- Little or on fluid is obtained at the time of amniotomy or aminocentesis .
6- Detection of amnion nodosum ( elevations due to vernix depositions ) in the placenta
and membranes .
Treatment :
I-
In cases with congenital fetal malformations TOP .
II-
Management of PROM .
III-
Management of IUGR .
IV-
Management of IUFD .
V-
Saline amnioinfusion is under trial .