Clinical Periodontology
UNIVERSITY OF MOSULCOLLEGE OF DENTISTRY
By: Dr. Huda A. Salim
B.D.S, M.Sc. In Oral and Maxillofacial Surgery
Mosul University/College of Dentistry/Oral and Maxillofacial Department.
2020-2021
Department of:
Oral and Maxillofacial Surgery.
Department of:
HEREUNIVERSITY OF MOSUL
COLLEGE OF DENTISTRYDepartment of:
HERE
Clinical Periodontology
Initial phase of treatment including examination and diagnosis determined by history, sign and symptoms, tests.UNIVERSITY OF MOSUL
COLLEGE OF DENTISTRY
Department of:
HERE
Proper diagnosis is essential to intelligent treatment. Periodontal diagnosis should first determine whether disease is present.
It should then identify the disease, and its severity and extent.
The periodontal diagnosis is determined after careful analysis of the case history and evaluation of the clinical signs and symptoms as well as the results of various diagnostic procedures (e.g., probing, mobility assessment, radiographs, blood tests, and biopsies).
UNIVERSITY OF MOSUL
COLLEGE OF DENTISTRY Diagnosis must therefore include a general evaluation of the patient and a consideration of the oral cavity
Overall Appraisal of the Patient
Health History:
Medical
Dental ( chief complain )
* Past dental history
* Ask about tooth brushing
* Others like mouth wash & I.D. Aids
* Areas of food impaction
* Teeth feel loose? Difficulty in chewing ?
* Habits (smoking, nail biting….etc)
* spreading of the teeth with the appearance of spaces where none existed before,
* foul taste in the mouth, or an itchy feeling in the gums.
* pain
UNIVERSITY OF MOSUL
COLLEGE OF DENTISTRY020-2021
Paragraph
Paragraph
UNIVERSITY OF MOSUL
COLLEGE OF DENTISTRY
020-2021
Clinical Examination:
Examination of Extraoral Structures:Temporomandibular joints, lymph node changes, glands.
Examination of the Oral Cavity:
* the extent of accumulated food debris, biofilm, calculus, and tooth surface stains.
* Oral malodor, which is also termed fetor ex ore, fetor oris, or halitosis
* The lips, the floor of the mouth, the tongue, the palate, the vestibule, and the oropharyngeal region.
Examination of the Periodontium:
*1st dryness of the gingiva.
*Inspect the color of gingiva,(red spongy texture smooth, glossy)or pale & firm or bluish gray
*Bleeding on probing (only 30% of sites with bleed will go on to lose attachment )
*Pressure by index finger
*Localized or generalized , marginal or diffused , edematous or fibrotic.
UNIVERSITY OF MOSUL
COLLEGE OF DENTISTRY020-2021
Paragraph
Paragraph


UNIVERSITY OF MOSUL
COLLEGE OF DENTISTRYDepartment of:
HERE
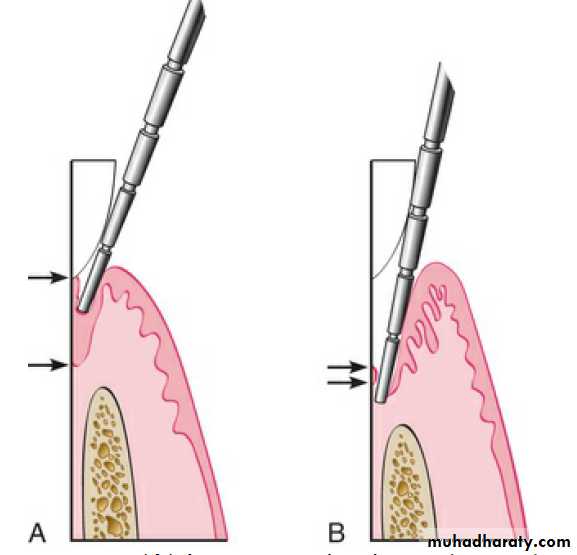
Probing Pocket Depth:
Distance from gingival margin to bottom of gingival sulcus/pocket).Dependent on the position of the G.M.
Differ from actual biological depth (is the distance between the gingival margin and the base of the gingival crevice (i.e., the coronal end of the junctional epithelium).
as it depend on: size or type, angulation, pressure (force), degree of inflammation, convexity of crown.
Others signs of pocket as rolled margin that separate from tooth surface, vertical discolored zone extend to mucogingival junction, pus discharge, extrusion of tooth with diastema.
UNIVERSITY OF MOSUL
COLLEGE OF DENTISTRYDepartment of:
HERE
Over & under estimation; as in healthy g.2/3 penetration of epith.in gingivitis its stopped o.1mm short of its apical end, in p.d.it past most apical cells of J.E. about 0.3mm
0.75 N force, accurate
Inter examiner error---2.1 mm ( average 1.5 mm )
UNIVERSITY OF MOSUL
COLLEGE OF DENTISTRYDepartment of:
HERE
Paragraph

UNIVERSITY OF MOSUL
COLLEGE OF DENTISTRY
Department of:
HERE
Bleeding on Probing:
The insertion of a probe to the bottom of the pocket elicits bleeding
if the gingiva is inflamed and if the pocket epithelium is atrophic or
ulcerated. Noninflamed sites rarely bleed.
To test for bleeding after probing, the probe is carefully
introduced to the bottom of the pocket and gently moved laterally
along the pocket wall. Sometimes bleeding appears immediately
after the removal of the probe; other times it may be delayed for a
few seconds. Therefore the clinician should recheck for bleeding 30
to 60 seconds after probing.
UNIVERSITY OF MOSUL
COLLEGE OF DENTISTRYDepartment of:
HERE
Probing Attachment Level:
Clinical attachment level measures the distancebetween the attachment level and a reference point on a tooth, such
as the cementoenamel junction.
Measured from a fixed reference point ; the CEJ or margin of restoration to the base of the gingival/ periodontal
pocket.
Detected in exposed & unexposed
CEJUNIVERSITY OF MOSUL
COLLEGE OF DENTISTRY020-2021
Furcation Involvement:
the pathologic resorption of interradicular bone within a furcation of a multirooted tooth due to periodontal disease. Classification:Ι, ΙΙ, ΙΙΙ, ΙV
• Special probe:
Nebers 2 , Za 3
Radiograph can detect 2 & 3
FI. Assessed all the entrances of possible periodontal lesion of multirooted teeth:
Buccal and /or lingual of mandibular molars.
Maxillary molar and premolars/ buccal /distopalatal/ mesiopalatal.
Due to furcation between MB and P:explored from palatal aspect.
UNIVERSITY OF MOSUL
COLLEGE OF DENTISTRYDepartment of:
HERE
UNIVERSITY OF MOSUL
COLLEGE OF DENTISTRY
Department of:
HERE
Tooth mobility:
Classification:Degree 0, 1, 2 and 3.
All teeth have a slight
degree of physiologic
mobility???
Causes of mobility:
1- Loss of tooth support (bone loss).2- Trauma from occlusion.
3- extension of inflammation.
4- Immediately after periodontal surgery.
5- Pathologic process of the jaw.
6- Tooth mobility is increased during
pregnancy.
UNIVERSITY OF MOSUL
COLLEGE OF DENTISTRYDepartment of:
HERE
:
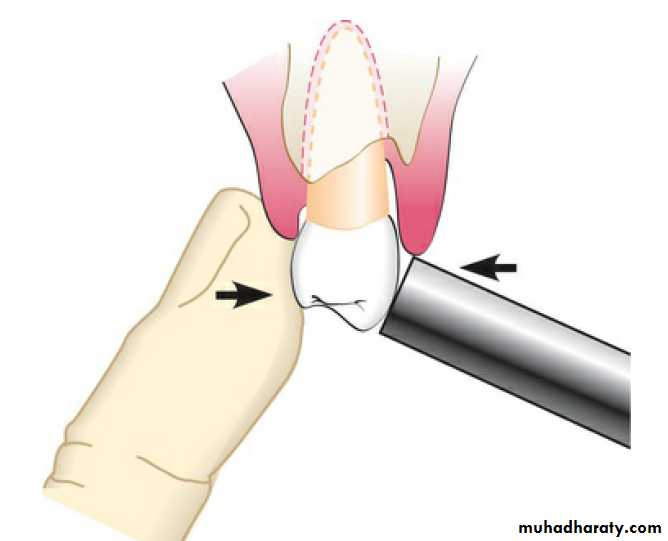
Techniques of tooth Mobility Detection:
UNIVERSITY OF MOSUL
COLLEGE OF DENTISTRY020-2021
Halitosis (fetor ex ore, fetor oris, malodor)
Foul or offensive odor that emanates from oral cavity, result from bact. putrefaction of protein containing sulfer A.A. that involve in transition from healthy g.to p.d. Intra oral causes ; retention of food ,NUG ,dehydration ,caries, denture, smoking, healing surgical or exo. wound, coated tongue ,pocket (accumulated debris), putrefaction of saliva
Extra oral causes;
lung disease, metabolites excreted through lung from onion, alcoholic ,acetone.
UNIVERSITY OF MOSUL
COLLEGE OF DENTISTRYDepartment of:
HERE
WASTING disease of teeth:
Gradual loss of tooth substance characterized by formation of smooth, polished surface
Erosion; wedge shaped depression in cervical area of facial tooth sur. E. caused by acidic food, acidic Salivary secretion, frectional action b/w soft & hard t.
Abrasion; caused by mechanical wear other than that of mastication started in Cementum due to clasp, tooth brushing
Attrition; occlusal wear due to functional contact with opposing teeth
Abfraction: occlusal loading surfaces causing tooth flexure and mechanical micro fracture the cervical area.
UNIVERSITY OF MOSUL
COLLEGE OF DENTISTRYDepartment of:
HERE


UNIVERSITY OF MOSUL
COLLEGE OF DENTISTRYDepartment of:
HERE
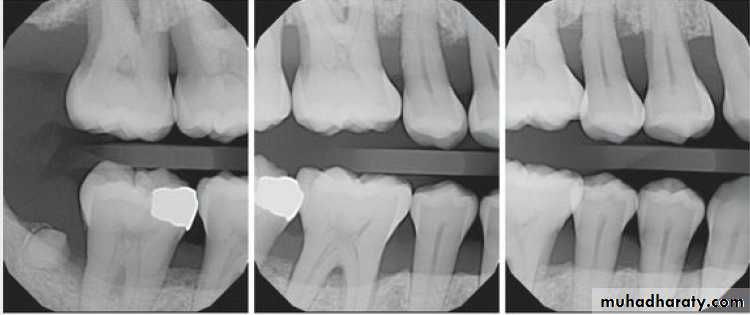
Radiographic Examination:
Radiographs are valuable for the diagnosis of periodontal disease,
estimation of severity, determination of prognosis, and evaluation
of treatment outcome.
The radiographic survey should consist of a minimum of 14
intraoral films and 4 posterior bitewing films.
Panoramic radiographs are a simple and convenient method of
obtaining a survey view of the dental arch and the surrounding
Structures.

UNIVERSITY OF MOSUL
COLLEGE OF DENTISTRYDepartment of:
HERE
The interdental bone normally is outlined by a thin, radiopaque line
adjacent to the periodontal ligament (PDL) and at the alveolar crest,referred to as the lamina dura.
Prichard established the following four criteria to determine
adequate angulation of periapical radiographs:
1. The radiograph should show the tips of molar cusps with
little or none of the occlusal surface showing.
2. Enamel caps and pulp chambers should be distinct.
3. Interproximal spaces should be open.
4. Proximal contacts should not overlap unless teeth
are out of line anatomically.
In conventional radiographs, periapical and bitewing projections
offer the most diagnostic information and are most commonly used
in the evaluation of periodontal disease.

UNIVERSITY OF MOSUL
COLLEGE OF DENTISTRYDepartment of:
HERE
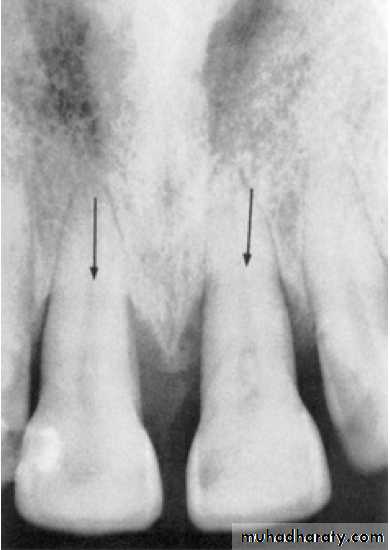
Pattern of bone loss:
Several investigators have analyzed the distance from the CEJ tothe alveolar crest.
The height of interdental bone may be reduced, with the crest perpendicular to the long axis of the adjacent teeth (horizontal bone loss), or
angular or arcuate defects (angular, or vertical, bone loss)
could form.


UNIVERSITY OF MOSUL
COLLEGE OF DENTISTRYDepartment of:
HERE
Parodontitis:
Parodontitis superficialis (mild –to- moderate periodontitis.
Parodontitis profunda (advanced periodontitis)
Parodontitis inter-radicularis (periodontitis in the furcation area).
UNIVERSITY OF MOSUL
COLLEGE OF DENTISTRY