Radiology L:1
Radiology of bone disease :
To study the modalities and the state of musculoskeletal system
In the top of the list is the X-rays examination because it simple , sensitive , formative
imaging modality
Then the MRI for further investigation
CT scan
Radioisotopes for osteomyelitis and metastasis
US
These are the modalities foe evaluation of the bone disease .
1. Plain X-rays
In each system in the body we should know what it the idea of the x-ray exam and which is the
standard view that we need to evaluate this area
Like:
the limbs we need: AP & lateral view
While spines: we need AP & lateral and the oblique
The signs that we found in x-ray exam :
a. Decrease in bone density : which is localized ( which mean solitary or focal lesion or
generalized decrease like in osteopenia )
The generalized osteopenia like in osteoporosis or osteomalasia
b. Increase in bone density : which is localized ( second sign ) or focal sclerosis or generalizes
Radiology L:1
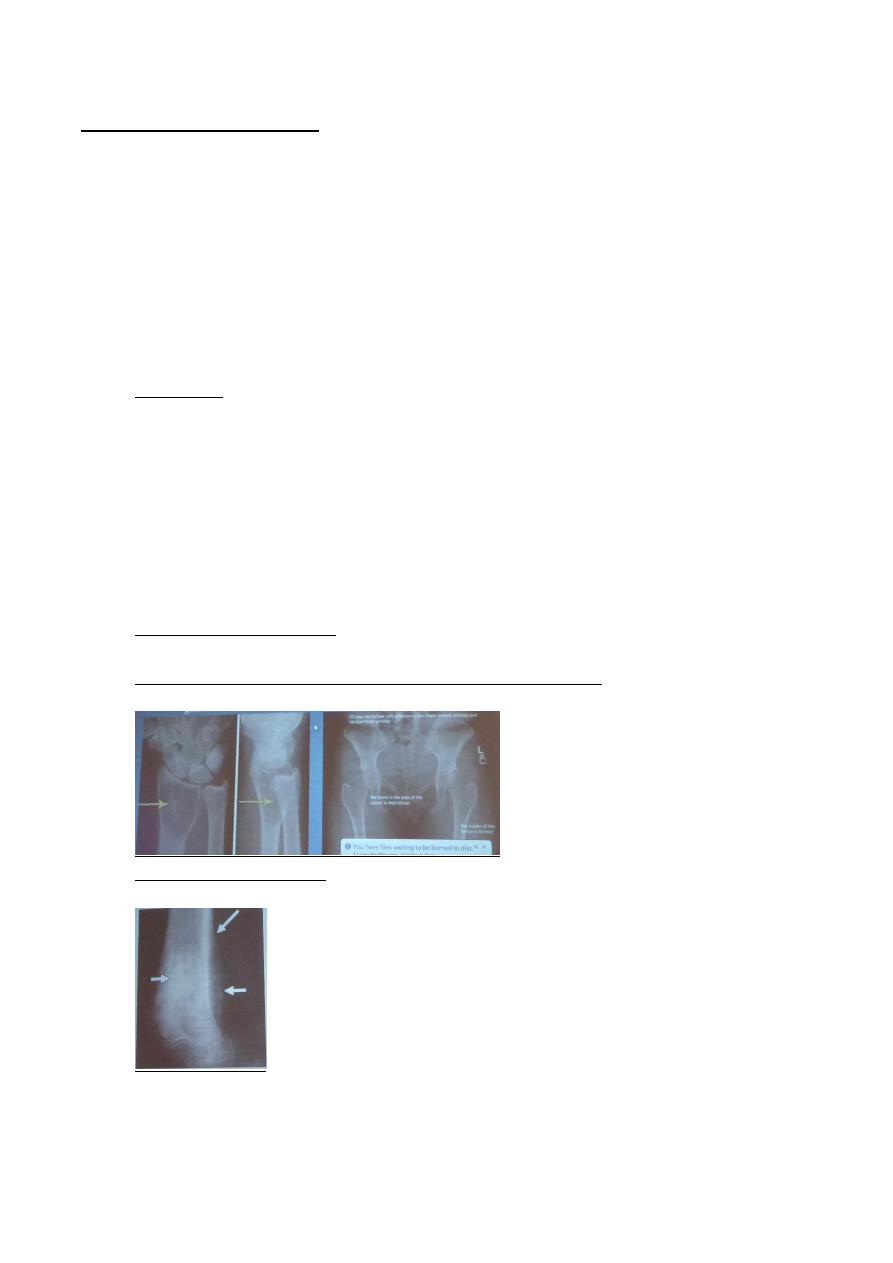
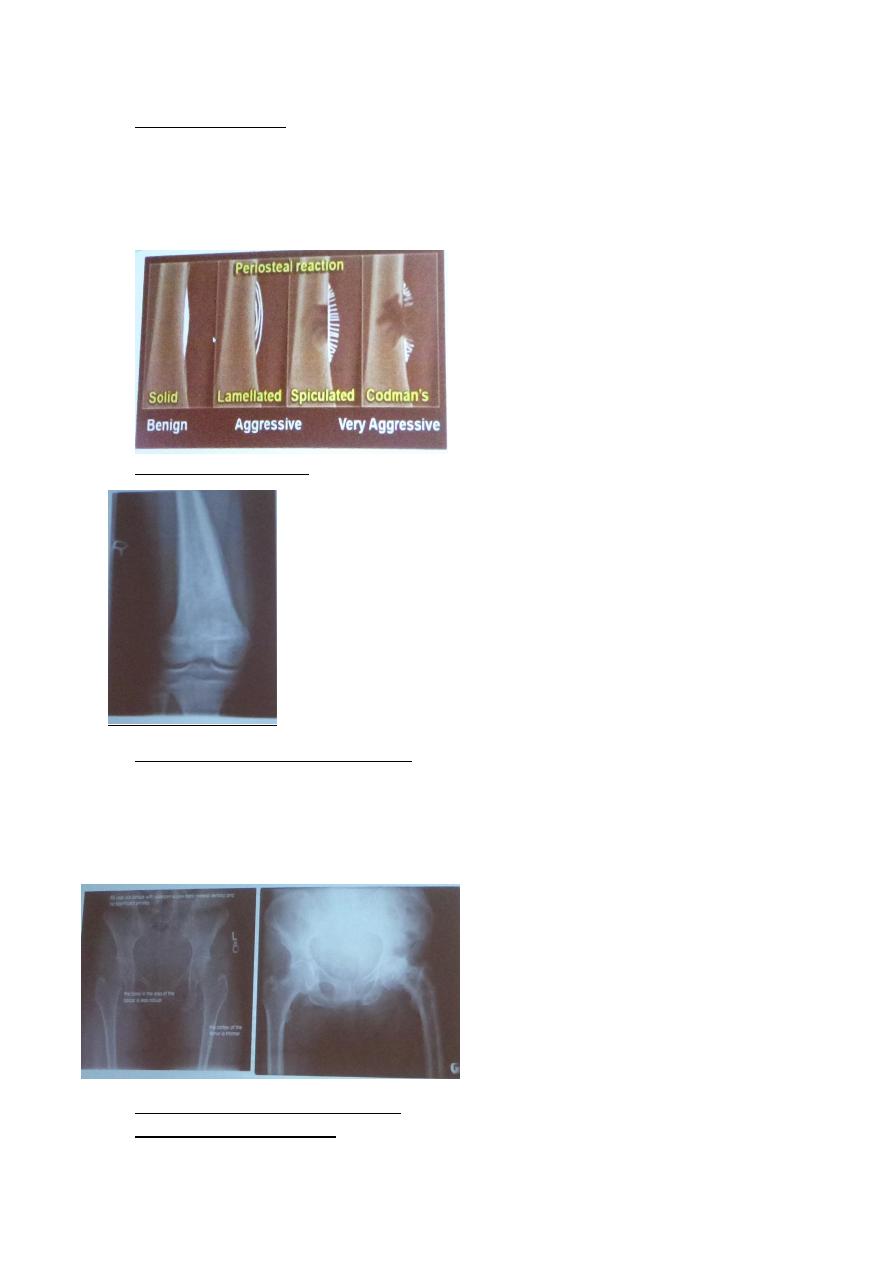
c. Periosteal reaction : according to the underlying cause
-the solid type : which is benign
-the lamellate
- the stellated
-the codman s
The last 3 types are aggressive which mean malignant
d. The cortical thickening :
e. Alternation in the trabecular pattern :
The bone matrix have trabculae ( primary & secondary ) , the alternation on it occur by certain
pathology just affect the trabculae by two pattern either : thinning of it and cause generalize
reduction in the bone density or forcing of it and cause generalize increase in density like in paget
disease
f. Alternation in the shape of the bone : like in acromegaly or metabolic disorders
g. Alternation in the bone age
Radiology L:1
2. US : used for solid tissue scanning and abscesses
3. Radioisotope bone scan : the radioisotope material used in bone scanning is technetium 99
labeled phosphate amount
Used for :
- Osteomyelitis
- Diagnosis of suspicious lesion in suspicious site or focal lesion like osteoid ostoma
- Multiplicity of lesion like the metastasis other bones from other tu.
4. CT scan
Used in :
- Demonstrating the abnormalities in pelvis and spine
- Demonstrating the extent & characterization of bone tumor in selected cases to
complement MRI like tumors in cortex and osteoid osteoma
- As Gide of bone biopsy
-
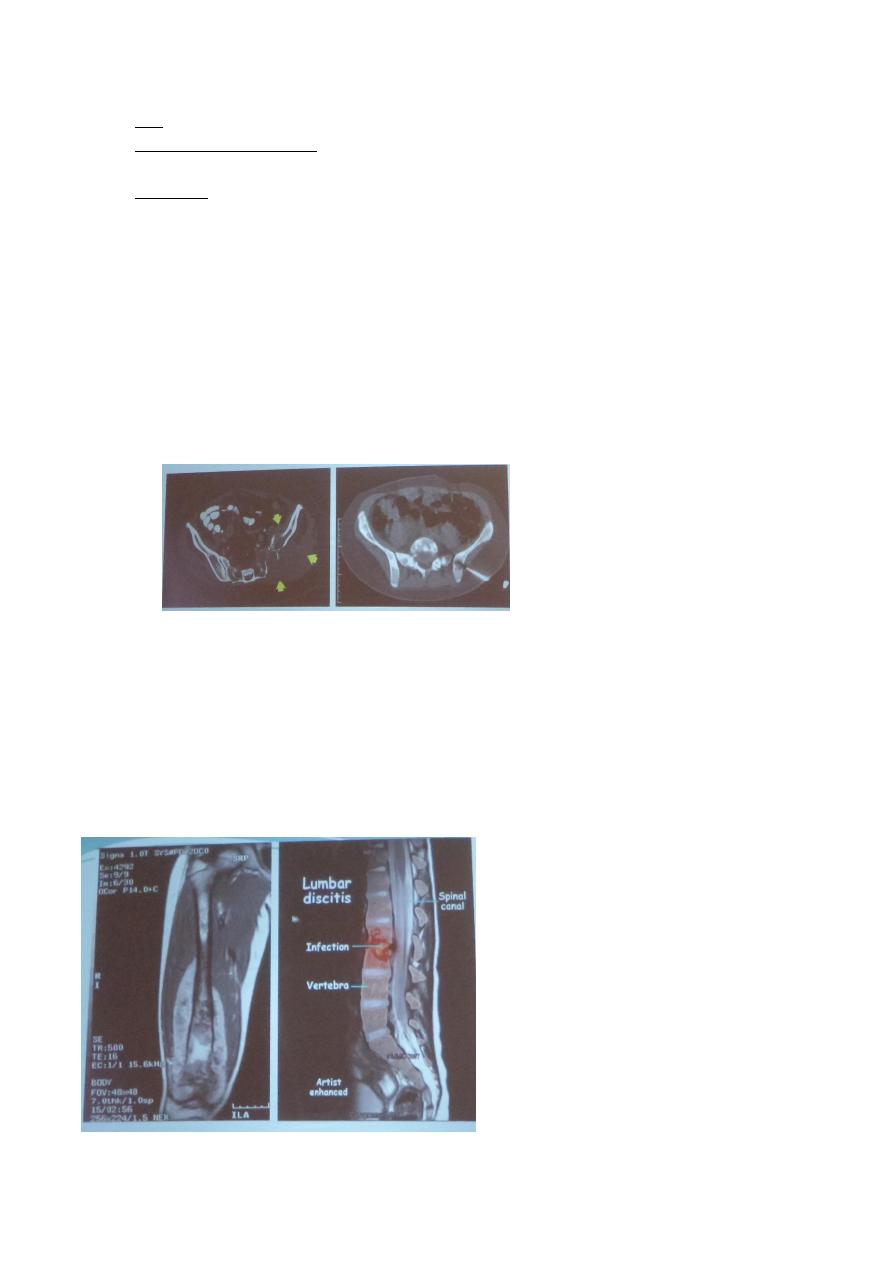
5. MRI
- demonstrate disc herniation and spinal cord or nerve root compression
- to diagnose bone metastasis
- show extent of primary bone tumor & demonstrate myloma & lymphoma
- image soft tissue mass foe local staging ( very specific )
- to diagnose osteomylitls in early stages & show any soft tissue abnormality
- to diagnose avascular necrosis & other joint pathology.
- Staging
Radiology L:1
Bone diseases
Solitary bone lesion are usually one of the following:
- .bone tumor: malignant ( primary or secondary ) , benign .
- osteomyelitis
- . bone cyst, fibrous dysplasia or other non -neoplastic defects of bone
- condition of uncertain nature such as langerhans histiocystosis
the initial radiological decision is usually to try &decide whether the solitary lesion is benign or its
aggressive by looking for the following features on plain radiographs & CT :
1. Zone of transition : which is the area that separate the normal from diseased areas >>so
that the margin is well or bad demarcated
So .. according to that we divided the bone disease into :
a. Solitary bone lesion , well define zone of transition with sclerotic rim ( it is a reactionary
sclerosis on the edge )
So when we see the rim + narrow transition zone it mean that the lesion is benign and not
aggressive
b. But when see ill define transition margin , wide zone of transition . it mean that it an
aggressive disease non- benign
c. In the mid between them there is well – define narrow zone of transition but without
sclerotic rim its diagnosis may be benign or malignant but the benign is more like in myloma
2. the adjacent cortex : if it preserved ( intact ) which mean benign , or it destroyed which
mean aggressive
3. Expansion : if the lesion caused expansion or not ? if no it benign , if yes it aggressive
Radiology L:1
4. Periosteal reaction :
When asked us what is the cause of periosteal reaction it mean all aggressive pathologies but
the most DDx for localized periosteal reaction are :
- Osteomyelitis
- Malignant bony tu. Especially Ewing sarcoma & osteosarcoma
- Occasional type of metastasis especially from neuroblastoma
- Langerhans histeocytosis
- Trauma because the pt. already come and his cortex is destroyed
5. Calcified densities
This calcified matrix cam from the cartilage to decide it benign ( without ) or aggressive ( with ) [
6. Soft tissue swelling
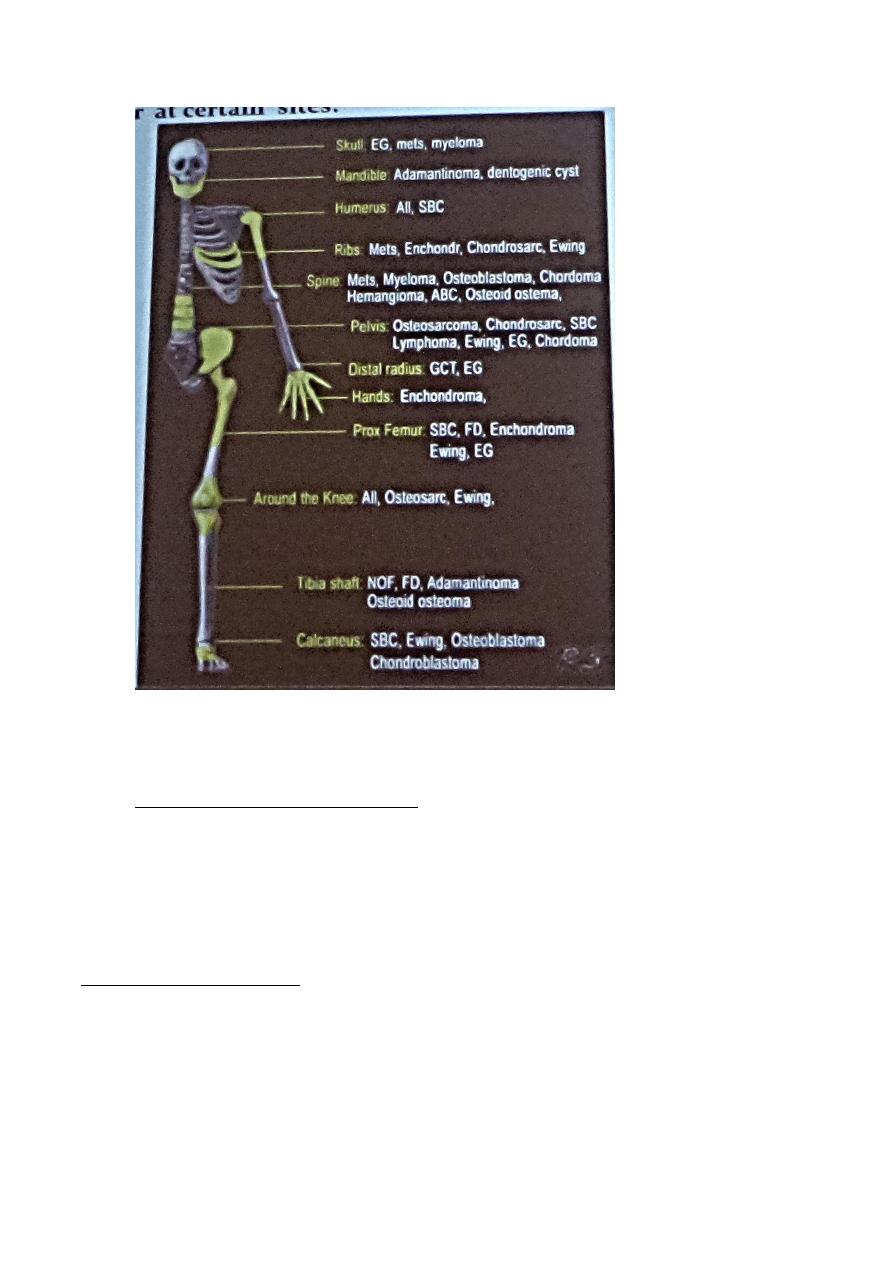
7. Site of lesion
- Which bone involve ?!
- And which the anatomical part of the involved bone had involved ? metaphysis or
epiphysis or diaphysis
Radiology L:1
Bone Tumors
Primary malignant tumours
1. Osteosarcoma ( osteogenic sarcoma ) the famous one , the commonest primary malignant
bony tu.
-Peak age is 5 – 20 yrs
-Aggressive
-Arise in metaphysis , commonly around knee
-Occur in elderly in one condition only when the pt. have preexisting bony lesion called
pagets disease
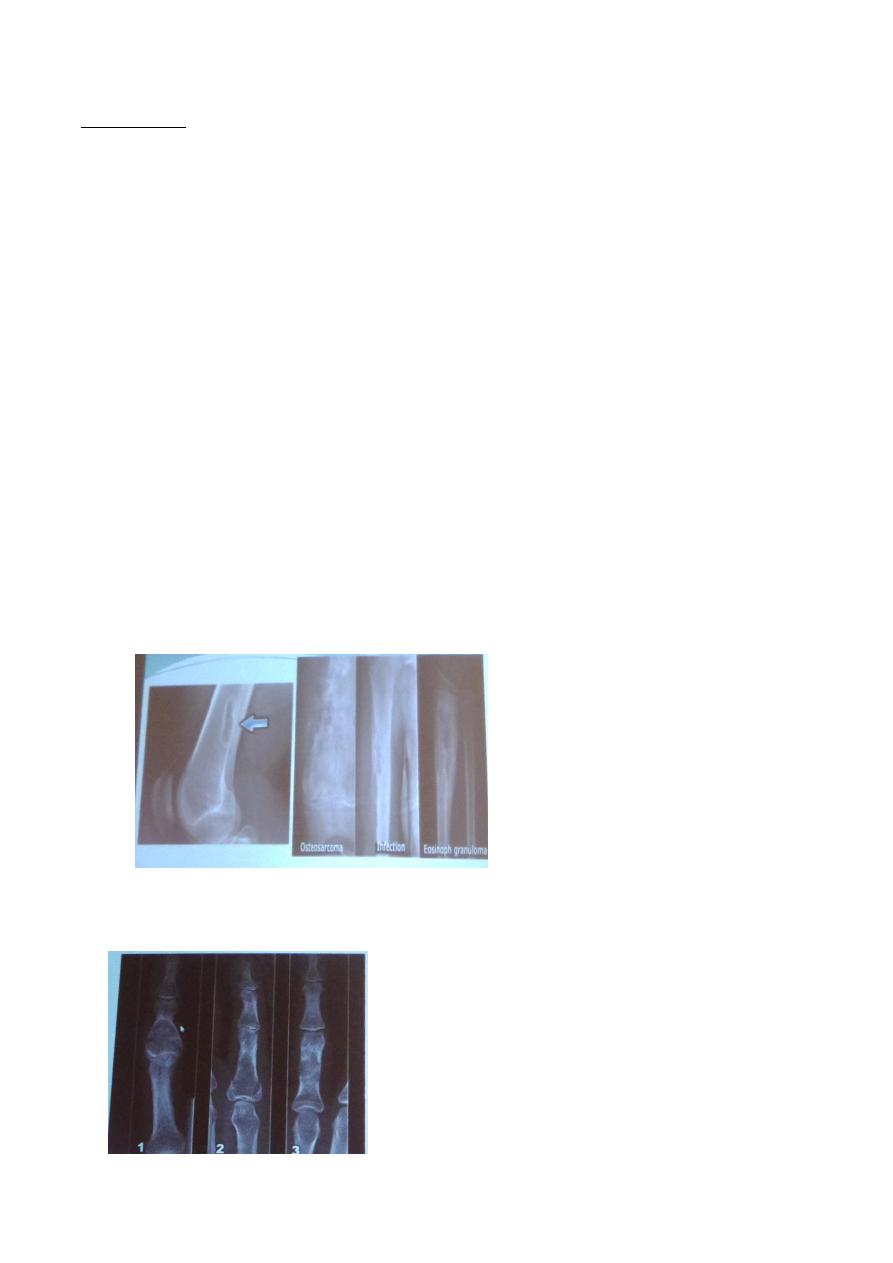
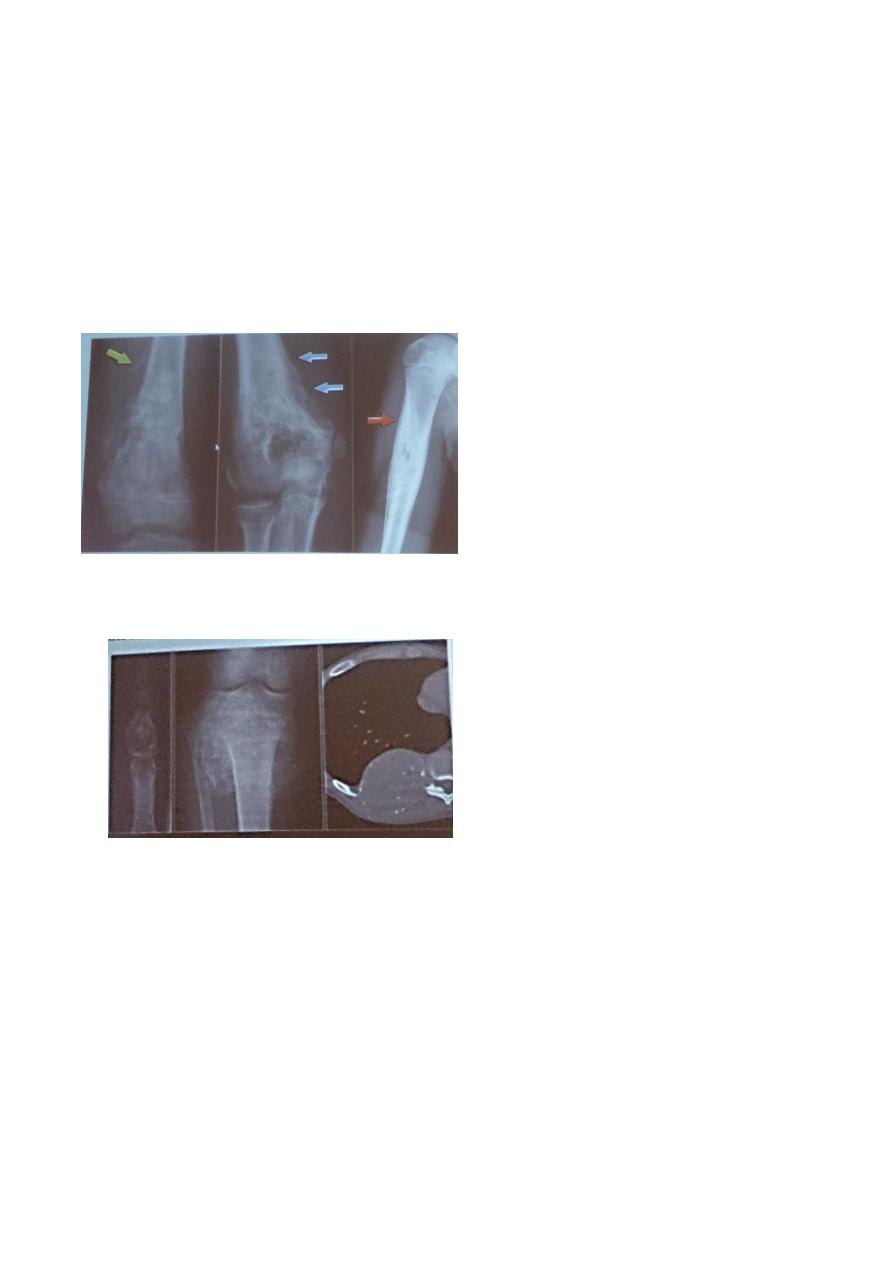
The Radiological appearance :
- Aggressive bony lesion
- Wide zone of transition
- Cortex destruction
- Different type of pereosteal reaction , but the commonest type is the codmans and
speculated one
- With soft tissue involvement
Radiology L:1
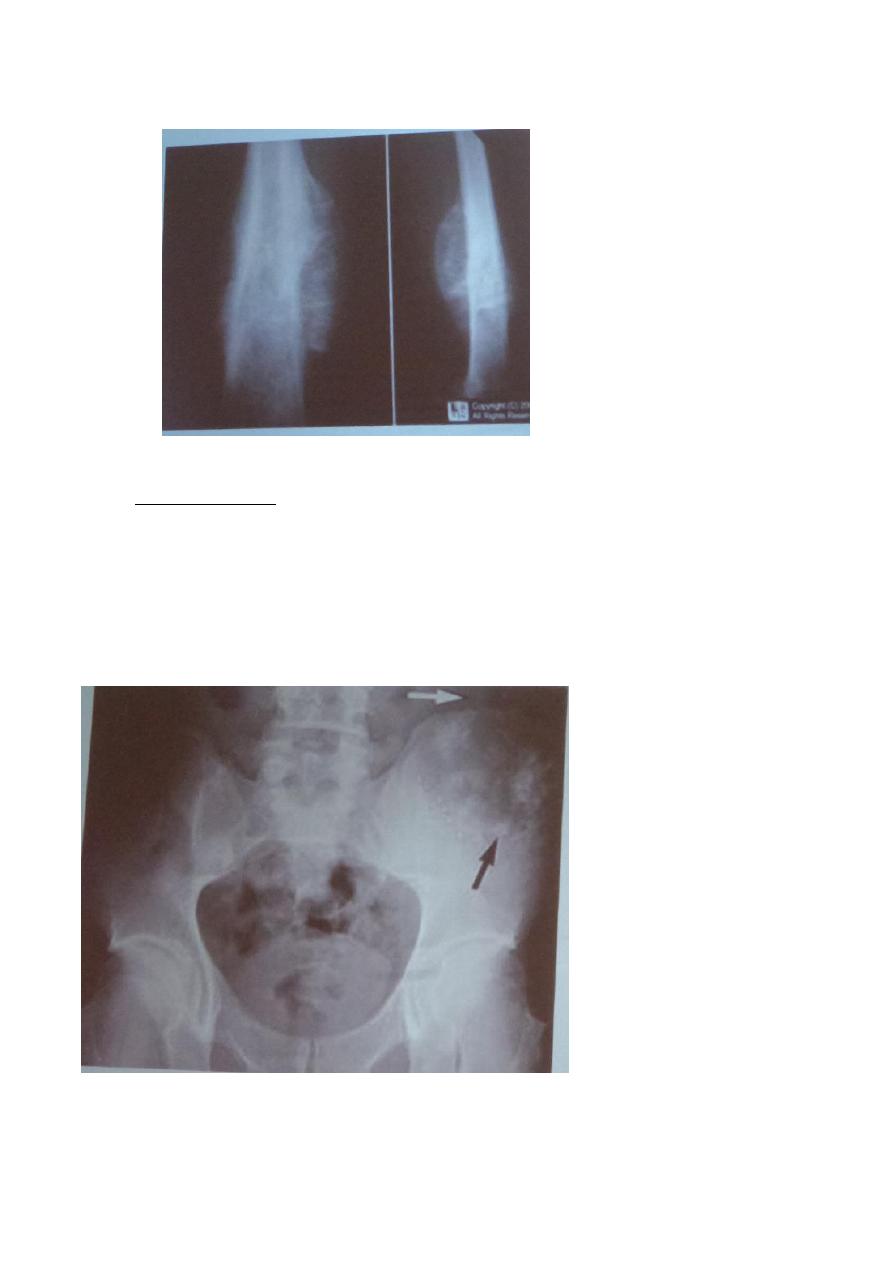
2. Chondrosarcoma : the 2
nd
most common one
- Arises from cartilage
- Occurred in 30 – 50 yrs people
- Occur in pelvis , ribs , scapulae , and humeri and femora
- It appearance as large soft tissue mass + speckled calcification
- When there is calcific lesion + benign appearance it mean chondroma
- The chondrosarcoma produce lytic expanding contains flakes of calcium which improve
the originality from cartilage

Radiology L:1
3. Fibrosarcoma + malignant fibrous histiocytoma كالت لتقروها )
- Rare
- Present as fibrocystic mass
- Damage the cortex
- Cant distinguish it in v-ray but in biopsy can
- In young and middle age people
- Aggressive boney lesion
4. Ewing s sarcoma
- Highly malignant
- Affect the children
- Rapidly progressive
- The commonest sites : diaphysis & shaft of long bones
Criteria :
- Lamellate type of periosteal reaction ( anion ) which is characteristic
- Aggressive bony lesion
- Wide zone of transition
5. Gaint cell tumor
- Have both malignant and benign and have local invasion but rarely metastasize
- Appearance : solitary
- Narrow zone of transition
- Age after 25-30 after closure of epiphyseal palate
- Occur in the sub-articular area , It have an expanding lesion + damaged cortex
- Not in diaphysis and mtaphysis
- In plain x-ray it not aggressive
- The commonest site is around wrist and knee

Radiology L:1
Benign Tumors
1. enchondroma :
- site : small metacarbal , ribs , long bone but commonly in the bone of head
- solitary or multiple
- lytic expansion with few flakes of calcium
- radiological appearance : solitary , expensile , no expansion , narrow zone of transition ,
no cortical damage

Radiology L:1
2. fibrous cortical defect ( non-ossifying fibromas )
- tubal lie lesion
- fibrous
- eccentric , near medulla in the cortex of long bone
- solitary
- little sclerotic rim
- benign
- asymptomatic
- common
- age 10-13 yrs ( child and young adult )
3. fibrous dysplasia
- affect one or several bones and may affect the same bone in several sites
- commonly in axial skeleton and humeri and femora and spine and long bones and ribs
- appearance : ground glass appearance
- criteria : geometry of bones change the shape of bone
- well define edge and may expand and may have sclerotic rim

Radiology L:1
4. simple bone cyst :
- wall of fibrous filled with fluid
- inside bone
- age below 20 yrs ( child and young adult )
- simple , benign
- site : humeri and femora
- narrow zone of transition
- asymptomatic , thin cortex , first clinical feature is pathological fracture
- form a leucency across the width of shaft of the bone
5. aneurysmal bone cyst
- have multiple blood pools
- site : spine + long bones + pelvis
- radiological appearance : benign with massive expansion of the cortex
- eccentric
- age : child and young
- still benign appearance , no periosteal damage
- definitive diagnosis by MRI & CT

Radiology L:1
6. osteoid osteoma
- benign
- painful
- commonest one
- site : in femur and tibia in young
- originate in cortex
- highly vascular
- presented as small tissue nidus with reactionary peaking around sclerotic rim
- in early presentation is just cortical and rarely see the nidus
- definitive diagnosis by MRI & CT scan
7. eosinophilic granuloma
- mildest and the most frequent form of Langerhans histeocytosis
- affect children & young
- single and multiple
- site : skull , pelvis , femur , rib
- extensive lesion may be – seen giving rise to the so- called geographic skull
- long bone lesions show bone destruction which may be aggressive with ill define margin
or benign with well definew margin + sclerotic rim
- sometimes see the periosteal reaction
Noor Rahman