OBESITY
Ameer kadhim Hussein
M.B.Ch.B. FICMS
Introduction
Obesity is a type of nutritional disorder, due to
imbalance between energy intake and energy
expenditure resulting in positive energy balance,
characterized by the abnormal growth of the adipose
tissue, resulting in an increase in the body weight to the
extent of 20 percent or more of the standard weight for
the person’s age, sex and height.
Body Mass Index
Body mass index (BMI) is based on weight and height
of the individual.
This is also called as ‘Quetelet’s index’, named after
Lambert Adolphe Jacques Quetelet, a Belgium Scientist.
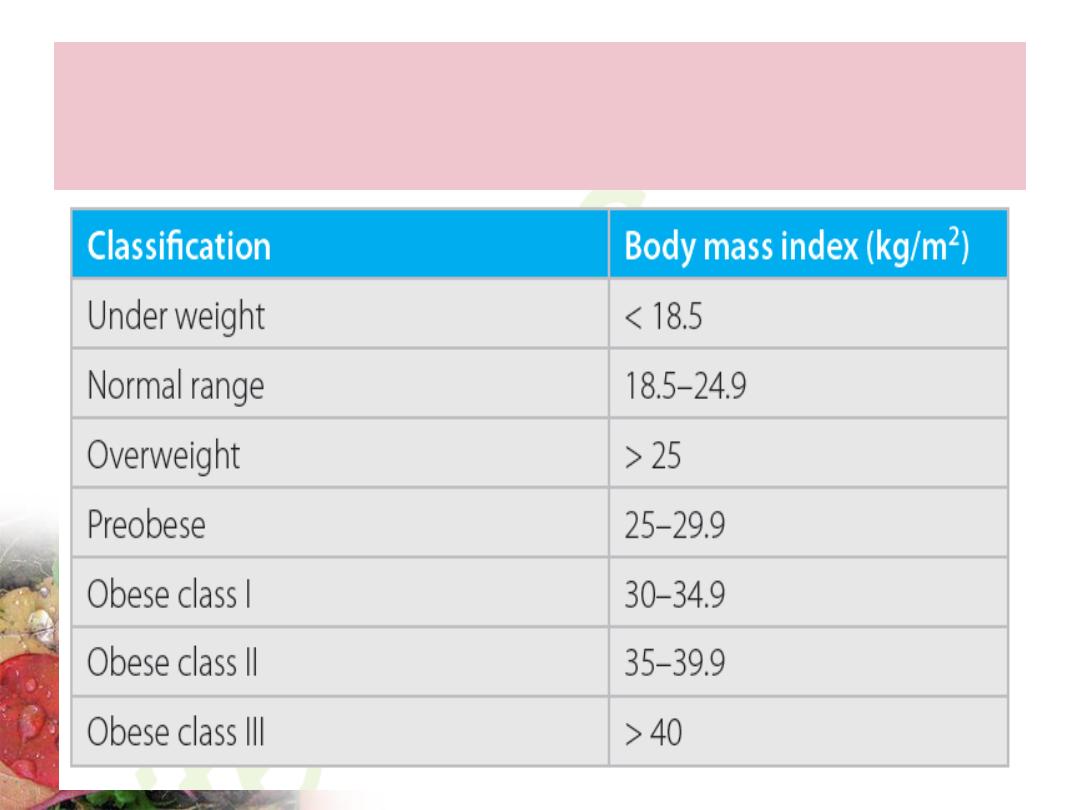
Classification of obesity according to
body mass index

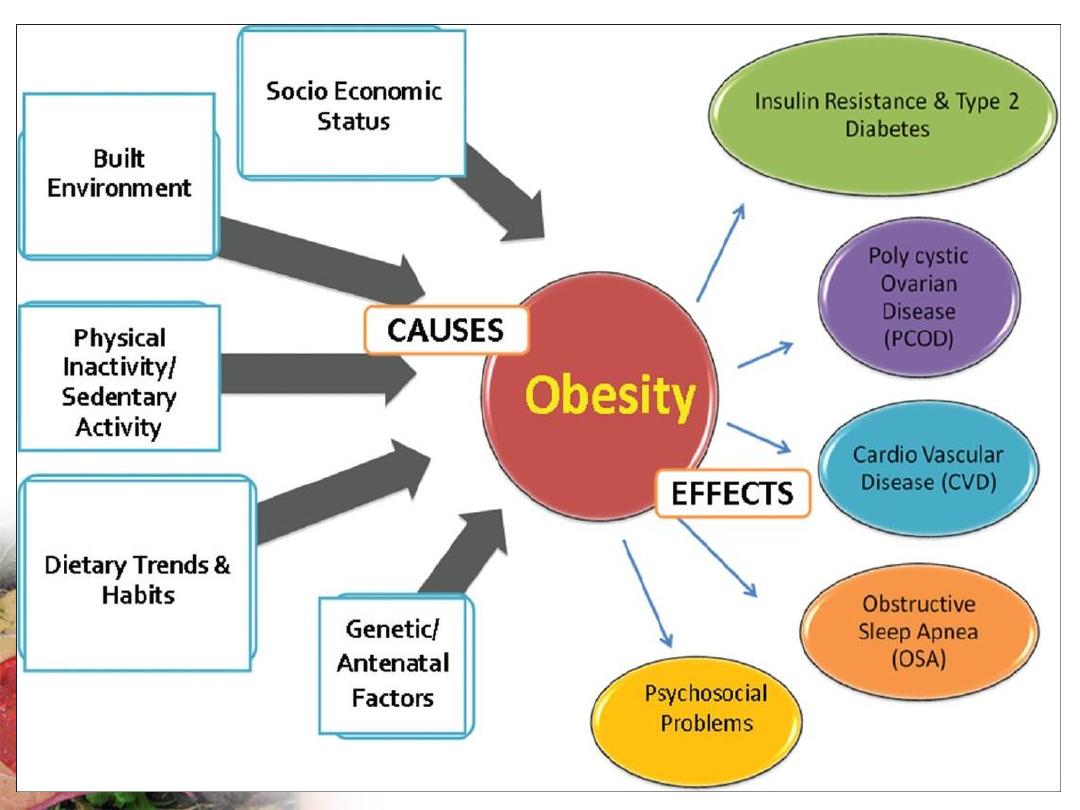
Risk Factors

Non modifiable Risk Factors
1.
Age: Obesity can occur in any age group. Generally it
increases with age. Obese children usually will have a
tendency to remain obese in future adult life.
2.
Sex: The prevalence of overweight is more among men but
obesity is more among women, specially during the
postmenopausal age, between 45 to 49 years.
3.
Genetic factors: Obesity tends to run in families, obese
children frequently having obese parents.
Modifiable Risk Factors
1. Physical activity: Regular physical activity burns
the fat and is protective against obesity, where as
sedentary lifestyle constitutes a risk factor.
2. Socioeconomic status: High socioeconomic status
correlates positively with obesity in the developing
countries. This association is reversed in the developed
countries, specially among women.
3. Literacy level: The relation has been observed to be
reverse, i.e. higher the literacy level, lesser is the
prevalence of obesity.
4. Body image: Traditionally it is considered that an
increase in body-weight is a sign of prosperity. But this
concept is now changed. Thin and slim body
symbolizes competence, success, control and sexual
attractiveness, while obesity represents laziness and
lack of willpower.
5. Smoking: Smoking increases the metabolic rate and
decreases food consumption. Thus smoking and obesity
are inversely related. Smokers often gain body weight
after giving up the habit.
Modifiable Risk Factors
6. Eating habits: Over nutrition is responsible for 95
percent cases of obesity. This is known as ‘Regulatory
obesity:’ Non nutritional causes like genetic, endocrinal,
metabolic, etc. account for the remaining 5 percent.
These are known as ‘Metabolic obesity’, e.g. Cushings
syndrome.
The capacity for storage of fat in human beings is highly
efficient and unlimited compared to protein and
carbohydrate. Therefore weight gain occurs primarily
due to high fat intake leading to anomalous fat balance.
Modifiable Risk Factors
7. Alcoholism: Alcohol intake is associated with increased risk of
abdominal fat. A recent report is that the relationship between
alcohol consumption and development of obesity is positive among
men and negative among women.
8. Psychological factors: People who are under constant emotional
strain find satisfaction in eating the food. Another motive for
overeating is the yearning for companionship. This forces the
individual to spend much time in the company of friends and foods.
9. Drugs: Use of certain drugs like corticosteroids, oral
contraceptive pills, insulin, β-adrenergic blockers, etc. can promote
weight gain.
Modifiable Risk Factors
10. Environmental factors: Fast process of
industrialization and urbanization has resulted in the
modernization of standard of living affecting the physical
activity pattern contributing to the development of
obesity such as Television viewing, using vehicles for
traveling short distances rather than going by walk or
cycling.
Modifiable Risk Factors


Prevention and Control
It is difficult or not possible to control obesity, caused
by non modifiable factors like age, sex or genetic factors
so we concentrate on modifiable risk factors. The
preventive measures should start early in childhood,
because once obesity is developed, it is difficult to treat
and the health consequences associated with obesity
may not be fully reversible by weight loss.
Aims
1. To maintain BMI between 18 and 25
throughout the adulthood.
2. To prevent the development of overweight.
3. To prevent the progression of overweight to
obesity.
4. To prevent regain of weight among those
obese patients, who have already lost some
weight.
Strategies
1. Dietary Changes
Refrain from over consumption of fats and carbohydrates.
Diet should contain suitable proportion of cereals, legumes and
vegetables, fibers content should be increased.
Food energy intake should not be greater than what is necessary
for energy expenditure.
Strategies
2. Physical Activity
Regular physical activity helps in increasing the energy
expenditure. So sedentary lifestyle should be discouraged.
Activity like gardening, dancing, cycling and swimming should
be encouraged.
Walking should be preferred to other means. Exercises should be
encouraged. Yoga exercises should also be encouraged.
Strategies
3. Health Education
People are educated about hazards of obesity and its
prevention by healthy diet and lifestyle, to be promoted
from early age.
4. Barrier Surgery
Among those whose BMI is >40 and is not possible to
control obesity with the routine measures of exercise
and change in life-style practices, ‘Barrier surgery’ is of
great help, where food consumption is minimized, there
by facilitating the subcutaneous fat to dissolve for
energy purposes.
ACCIDENTS
Accident has been defined as unexpected and un
planned occurrence which involve injury.
WHO group defined accident as
“Unpremeditated event resulting in recognizable
damage”.
Agent
Accidents and injuries are commonly classified
based on “intentionality”.
Most road traffic injuries, poisoning, falls, fire
and burn injuries, and drowning
are
unintentional.
Intentional injuries include interpersonal
violence (
homicide, sexual assault, neglect and
other maltreatment
),
suicide, and collective
violence (war).
Host
Poisoning, drowning, burns, and maltreatment by caregivers
affect primarily small children.
Road traffic accidents, interpersonal violence and sports injuries
tend to affect older children and adolescents.
In addition, injuries tend to be more prevalent in boys.
ACCIDENTS
Environment
In the rural areas injuries mainly including farming
activities, pesticide poisoning, and drowning.
In the urban areas, most injuries are traffic related, or
linked to electrical appliances, falls or poisonings
resulting from household chemicals and drugs ingested
by small children.
The environmental factors leading to injury may also be
associated with social factors, such as family stress and
critical life events (e.g. hospitalization or chronic
disease of a parent, or change of residence).
Road traffic accidents
About 1.25 million people die each year as a result of road traffic
crashes.
Road traffic injuries are the leading cause of death among young
people, aged 15–29 years. 90% of the world's fatalities on the
roads occur in low- and middle-income countries.
Half of those dying on the world’s roads are “vulnerable road
users”: pedestrians, cyclists and motorcyclists.
Without action, road traffic crashes are predicted to rise to
become the 7th leading cause of death by 2030.
The newly adopted 2030 Agenda have a target of halving the
global number of deaths and injuries from road traffic crashes by
2020.

Preventing accidents
Primary prevention
1. Data collection of all accidents, and possible
reconstruction of how the accident happened.
2. Safety education that must begin with children, and
end with drivers; the education must be delivered
through schools and include traffic rules, common
hazardous substances in the households, safe use of
electrical devices, etc.
3. Use of personal protective equipment eg. Seat belts,
helmet, leather clothing and boots, steering balloons.
4. Improve environment, i.e. Roads, lighting, marking
of danger points, provision of fire guards, to store toxic
substances safely and out of reach of children, etc.
5. Laws to ensure that only good quality drivers (who
are medically fit) and vehicles get on the street, speed
limits are not crossed and alcohol limit in blood/ breath
stays below threshold.
Primary prevention
Emergency care after accidents, with rehabilitation
services must be integrated into primary health
care.
Secondary prevention