By
Dr.Ashraf Hussain
PhD. Community Medicine
Occupational Respiratory Diseases
Occupational Respiratory diseases
are broad group of pulmonary disorders that develop
from inhalation of specific particles.
Historically, they have been a major cause of
morbidity and mortality before workplace safety
guidelines were rigorously established and enforced.
Although each disease has a slightly unique
presentation, they all lead to progressive
deterioration in lung function that can cause severe
respiratory compromise if appropriate measures are
not undertaken.
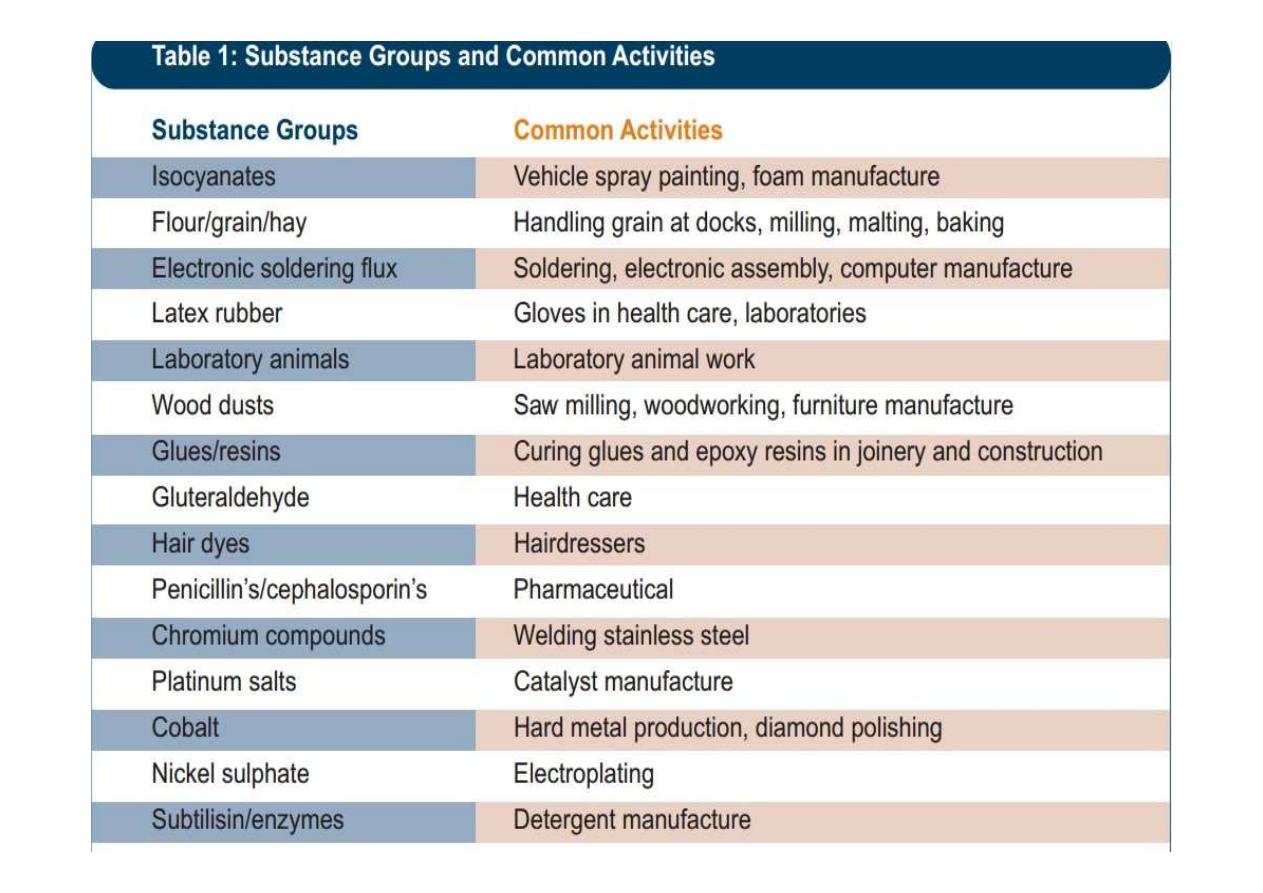
Occupational asthma
airflow limitation and airway hyper-
responsiveness caused by specific agents inhaled
in the workplace.
Caused as a direct result of workplace exposure.
It does not include activation of pre-existing
asthma.
Two types of occupational asthma are recognised:
Allergic Occupational Asthma or (Immunological
asthma) appears after a latent period of occupational
exposure;
Non-immunological occupational asthma develops
without a period of latency and is associated with
exposure to high concentrations of irritants also
called (Irritant Induced Occupational Asthma or
Reactive Airways Disease).
Irritant Induced Occupational Asthma
Also called reactive airway dysfunction syndrom or
reactive airway disease.
Usually develops after a single, very high exposure to
an irritant chemical.
The high levels of exposure required are
usually the result of accidents or some major failure of
controls, often in enclosed spaces
Frequently, individuals complain of a burning sensation
in their nose and throat within minutes of exposure up
to 24hrs (no latent period)
It is a direct “burn” effect on the airways and is not
related to the immune system.
Examples of causal agents include ammonia,
chlorine, acids and smoke.
Symptoms will tend to improve over time and may
go away entirely but if symptoms persist beyond 6
months, persistent problems are possible
.
Diagnostic criteria for reactive airways
disease syndrome
Individual previously free from respiratory
symptoms
History of inhalation of gas, fume, or vapour with
irritant properties.
Rapid onset of asthma like symptoms after
exposure
Bronchial hyper-responsiveness on methcholine
challenge test
Allergic Occupational Asthma
Allergic Occupational Asthma is caused by
sensitisation to a specific chemical agent in the
workplace over a period of time.
This is the mechanism for the vast majority
(>90%) of cases of occupational asthma.
The sensitisation process does not occur after one
exposure but develops over time (i.e., latency
period).
The latency periods are variable and can be as
short as several weeks or as long as 30 years.
If exposure is consistent, the period of greatest
risk is the first two years of exposure but the risk
does not go away after that but may reduce
somewhat.
If exposure to the causative agent ceases
completely, the condition will nearly always
improve.
If this happens within the first two years of the
development of the condition then complete
recovery is usual.
The longer exposure however, not only cause the
tendency for the condition to get worse, but the less
likely it is that there will be a complete recovery
although a cessation of exposure is nearly always of
benefit
.
For these reasons identifying a case of occupational
asthma as early as possible is of paramount
importance, and hence the reason for health
surveillance.
Health surveillance is used to detect the early onset
or symptoms of asthma.
It is deemed to be secondary prevention, (by
detecting adverse effects early rather than total
prevention)
Health surveillance can take the form of a pre
employment medical assessment, an annual
respiratory questionnaire or lung function tests or
both depending on the situation.
This should be carried out by a competent health
professional 3 months and 12 months after job
commencement and annually thereafter.
The respiratory questionnaire should be
completed again and results compared to pre
employment ones.
If health surveillance indicates that an employee
has become sensitized, the employer should
remove the worker from working with the
sensitizer and advise him/her to consult a doctor.
This would also indicate that the existing control
measures are inadequate and the Risk Assessment
should be reviewed and any necessary changes
should be made.
Byssinosis
Also called Monday fever or cotton workers' lung.
Hypersensitive airways and acute reduction in FEV1 in susceptible
individuals when they are exposed to dusts of cotton or flax.
Acute dyspnoea with cough and chest tightness on the first day of
the working week, then symptoms improve on subsequent
working days, despite continued exposure to the sensitizing agent.
As the disease progresses the symptoms recur on subsequent days
of the week, and eventually even occur at weekends and during
holidays.
If the workers who develop byssinosis are not removed from
further exposure, they go on to develop long term respiratory
impairment and subsequently have an excess risk of mortality
from respiratory disease.

2. Interstitial lung diseases (ILDs)
are a heterogeneous group of more than 100 diseases that result
in inflammation and/or scarring of the lung parenchyma.
Both occupational and non-occupational ILDs have similar
pathophysiology(ies), progressive fibrotic changes, structural
abnormalities, and common physiologic sequelae.
Occupational ILDs have varied latency periods, usually
measured in years, and present predominantly or exclusively
with pulmonary manifestations.
Extra pulmonary symptoms and signs rarely occur (eg, cases of
beryllium disease, silica-associated autoimmune disease, or
renal disease).
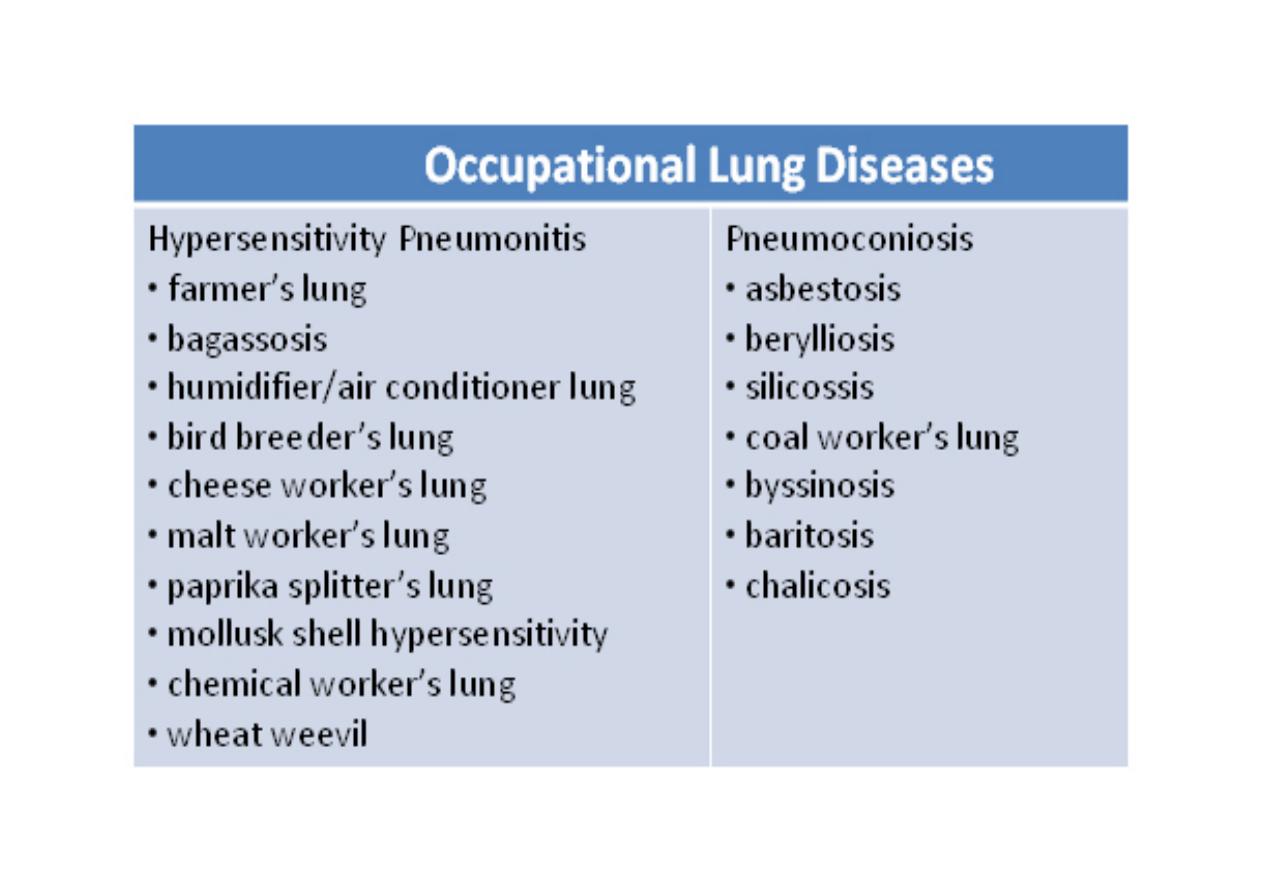
Pneumoconiosis
Pneumoconiosis is the generic term for the inhalation
of mineral dust and then the resultant diffuse, usually
fibrotic, reaction in the acinar part of the lung.
The term excludes asthma, neoplasia, and emphysema.
Hundreds of types of pneumoconioses have been
identified, but only three are common : asbestosis,
silicosis, and coal workers’ pneumoconiosis.
In these conditions, the radiologic findings were
resulting from the accumulation of inflammatory and
fibrotic responses triggered by dust deposition.
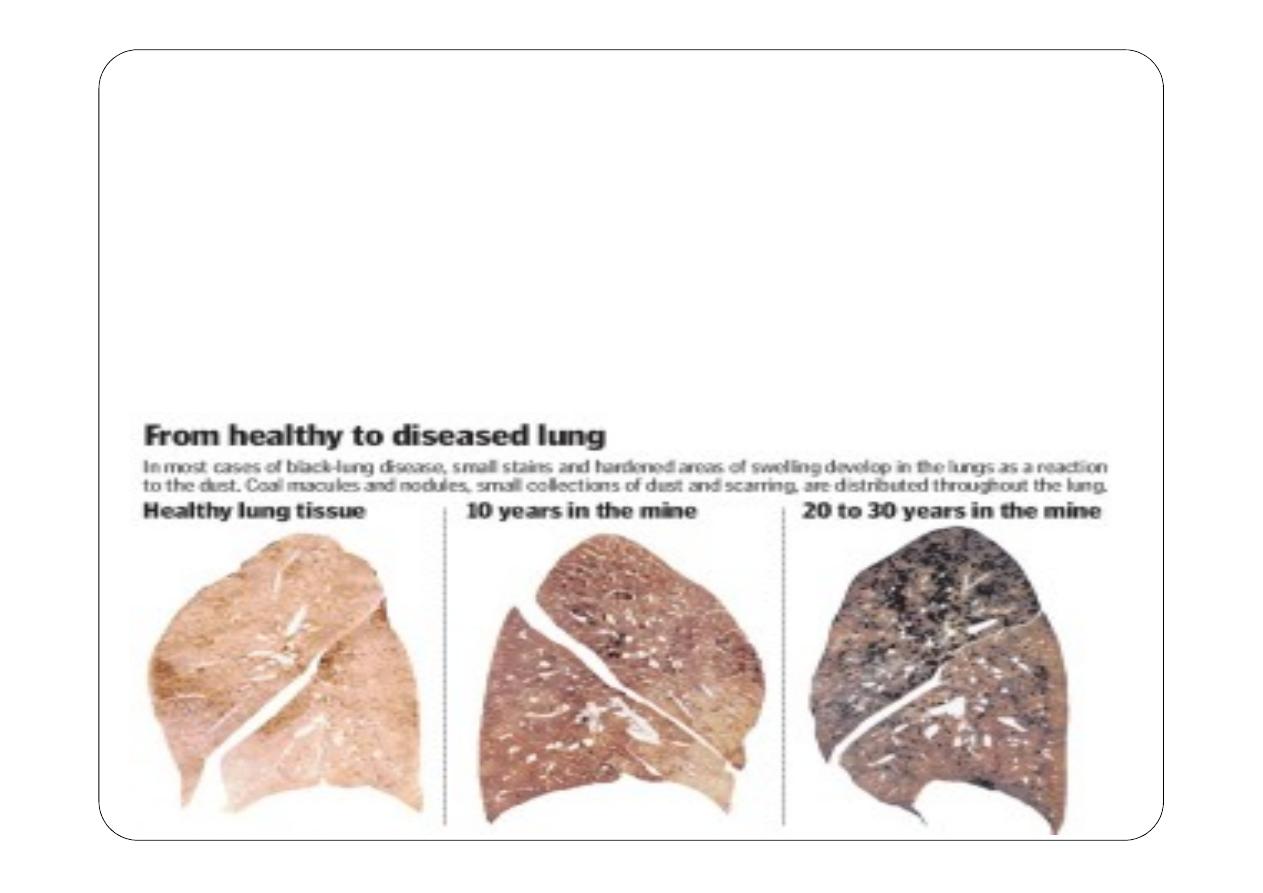
Coal Worker’s Pneumoconiosis (CWP
Also known as black lung disease
Interstitial lung disease result from long term exposure
(usually more than 20 years) to high levels of Coal
dust.
Simple CWP is largely only an abnormality on the
chest radiograph; there are small spots in the upper
lung zones that reflect inhalation of coal dust, but
nothing more.
Symptoms include shortness of breath, cough may be
chronic and problematic in patients even after they
leave the workplace and lowered pulmonary function.
However, it can develop into complicated CWP, which is
also called progressive massive fibrosis in which the
smaller shadows coalesce into large nodules, 1 to 2
centimeters in diameter.
These lesions can distort and destroy normal lung
architecture and result in severe shortness of breath,
disability and can lead to death.
CWP is diagnosed based on chest X-ray or CT findings,
and a history of work in coal mines.
There is no cure for coal worker’s pneumoconiosis.
Caplan Syndrome
Exposure to coal dust has been found to result in airflow
obstruction and chronic bronchitis and is also associated with
the development of rheumatoid arthritis, which when
combined with CWP is known as Caplan syndrome
Asbestosis
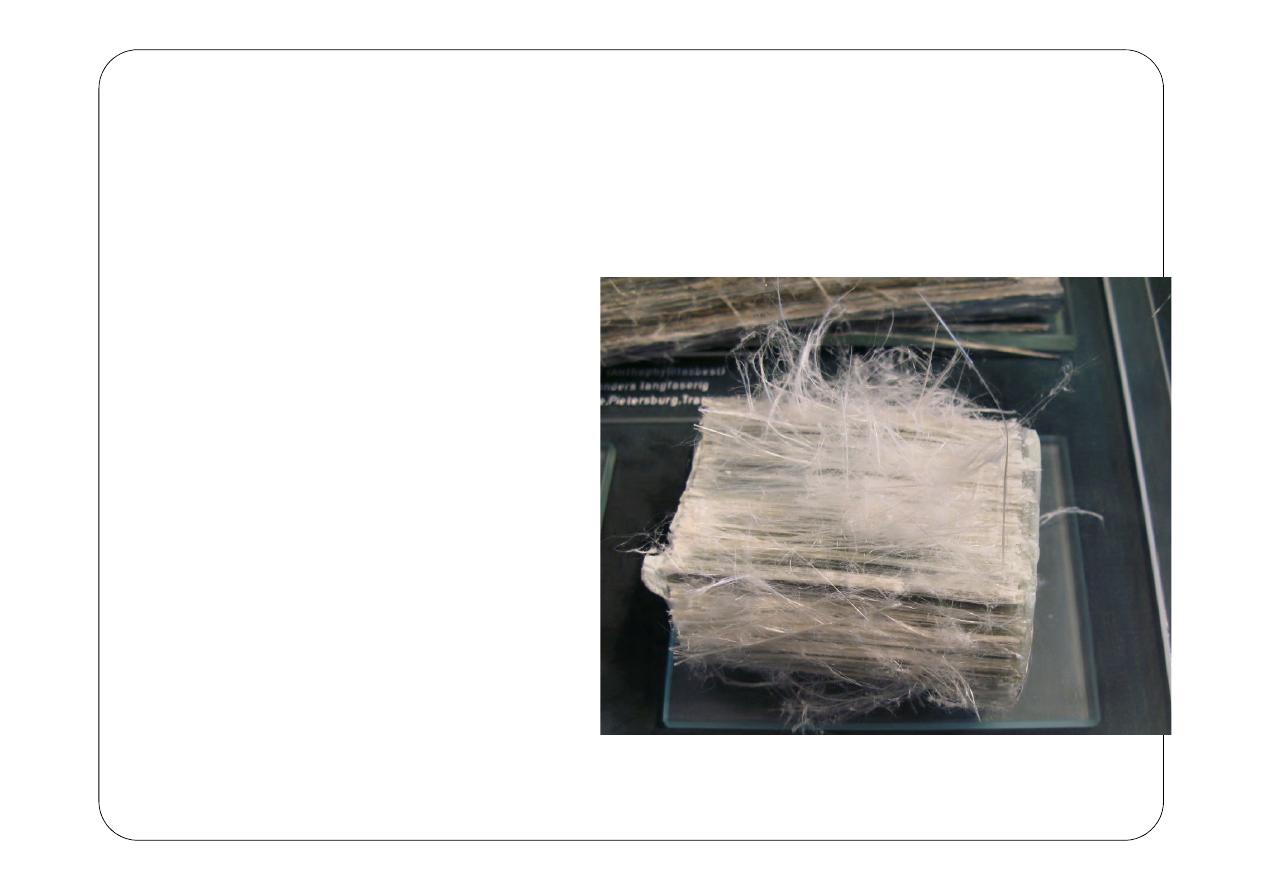
What is asbestos ?
Asbestos is a set of six
naturally occurring silicate
minerals , which is called by
that name due to
asbestiform habbit :
long thin fibrous crystals,
and each visible fiber
composed of millions of
microscopic "fibrils" that can
be released by abrasion and
other processes
Characteristics of
asbestos ?
Asbestos fibers are:
•
Very strong
•
Highly flexible
•
Non-biodegradable
•
Environmentally persistent
•
Resistant to breakdown by acid, alkali,
water, heat, and flame
Uses of Asbestos
Automotive Parts: Brake pads, clutches, gaskets and
valves.
Tiles: Flooring, ceiling and roofing tiles were
commonly made with asbestos. The adhesive used to
lay down flooring tiles has also been a source of
exposure.
Cement: Asbestos-containing cement was used in
building materials because the fibers provided
strength without adding much weight.
Its insulating and fire-resistant properties also made
the mineral an ideal substance to add to cement.
Textiles: Asbestos was used in the production of
cloths and garments for its resistance to heat and
corrosive elements. Some of the most common
textiles included blankets, fireman suits and rope.

Asbestos exposure is a concern for the following
workplaces and processes:
Mining of asbestos occurring from natural mineral
deposits
Processing of asbestos minerals (millers)
Manufacture of asbestos-containing products
Construction industry - disturbing asbestos-containing
materials during building renovations or demolitions
Mechanics - vehicle brake and clutch repairs
Marinas - renovating or demolishing ships constructed
with asbestos-containing materials
Insulation workers and heating trades
Sheet metal workers, plumbers and pipe fitters
Workers responsible for disposing of asbestos waste,
and waste workers
Cement workers
Custodial workers - contact with deteriorating
asbestos-containing materials in buildings
Pathophysiology and health effects
Factors
•
Asbestos fibrils are small so can travel
deeper into the lungs
•
Sharp pentrate through tissues
•
Hydophobic cant be coughed out
•
Contain Iron so can be oxidised
damaging neuclus
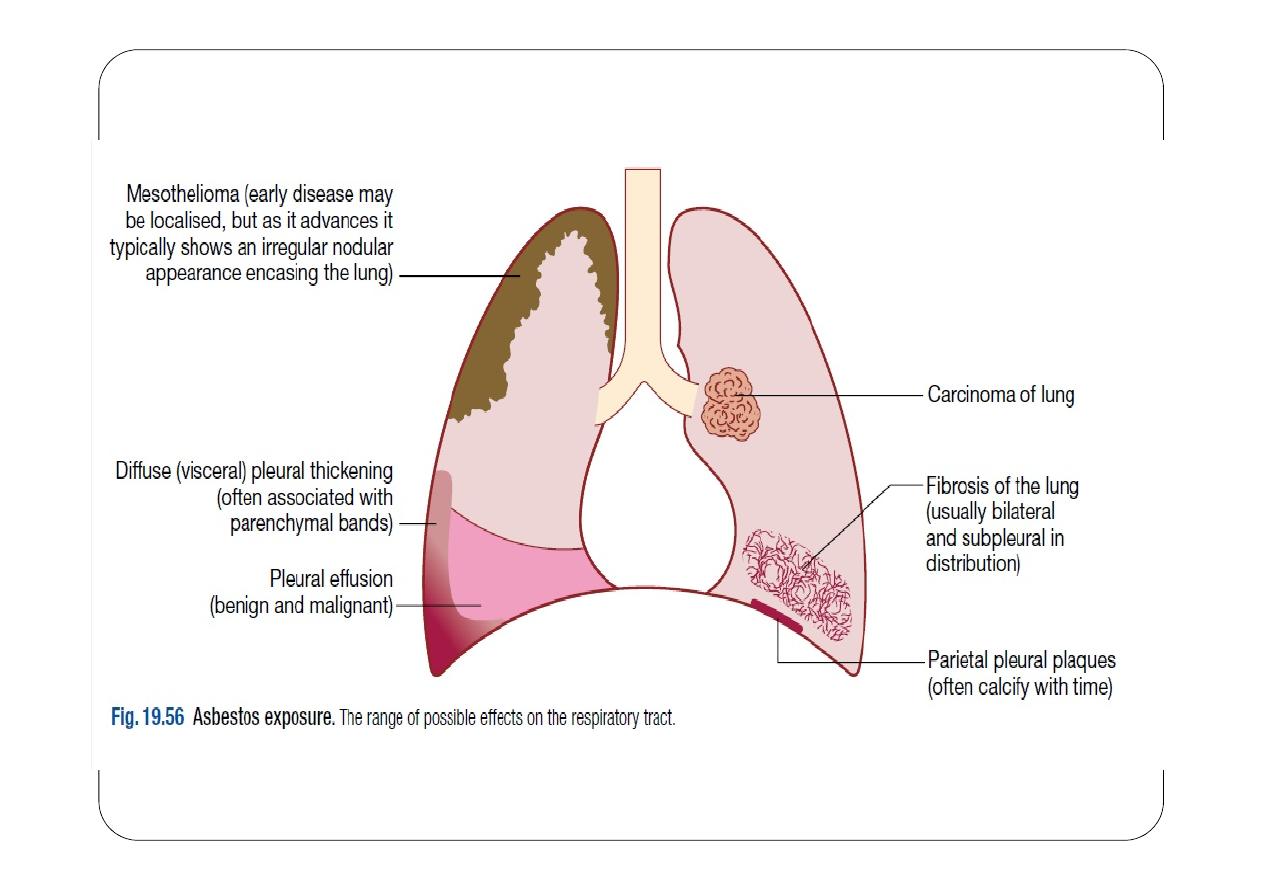
Diseases ?
Respiratory :
Parenchymal asbestosis : Diffuse interstitial
fibrosis
Asbestos-related pleural abnormalities
Pleura plaques
Benign asbestos pleural effusions
Diffuse pleural thickening
Pleural mesothelioma
Lung carcinoma
Severity depends on:
o
Nature and extent of exposure
o
Concentration of asbestos fibers
o
Duration and Frequency of exposure
o
Cigarette smoking
Histopathology
On gross examination, visceral pleura is markedly
thickened, especially on the lateral and diaphragmatic
surface of the lung with localized fibrous plaques and
pleural effusions.
Diffuse fibrosis of the lower lobe of the lung is visible on
the cut section.
Fibrosis causes distortion of the lung parenchyma
architecture, which causes the formation of enlarged air
space surrounded by a thick fibrous wall and hyperplastic
type II pneumocytes called honeycomb appearance.
History and Physical
Usually, there is a history of 10 to 20 years of exposure to
asbestos and progressively worsening dyspnea.
Cough with sputum and wheezing are unusual while
nonproductive cough is quite common.
History of loss of appetite and weight, hemoptysis indicates
the suspicion of lung tumors.
Physical examination reveals clubbing in 32% to 42%,
Reduced chest expansion due to restrictive lung disease
(38%).
Right-sided heart failure from pulmonary vascular
remodeling.
Mesothelioma
Plural plaques
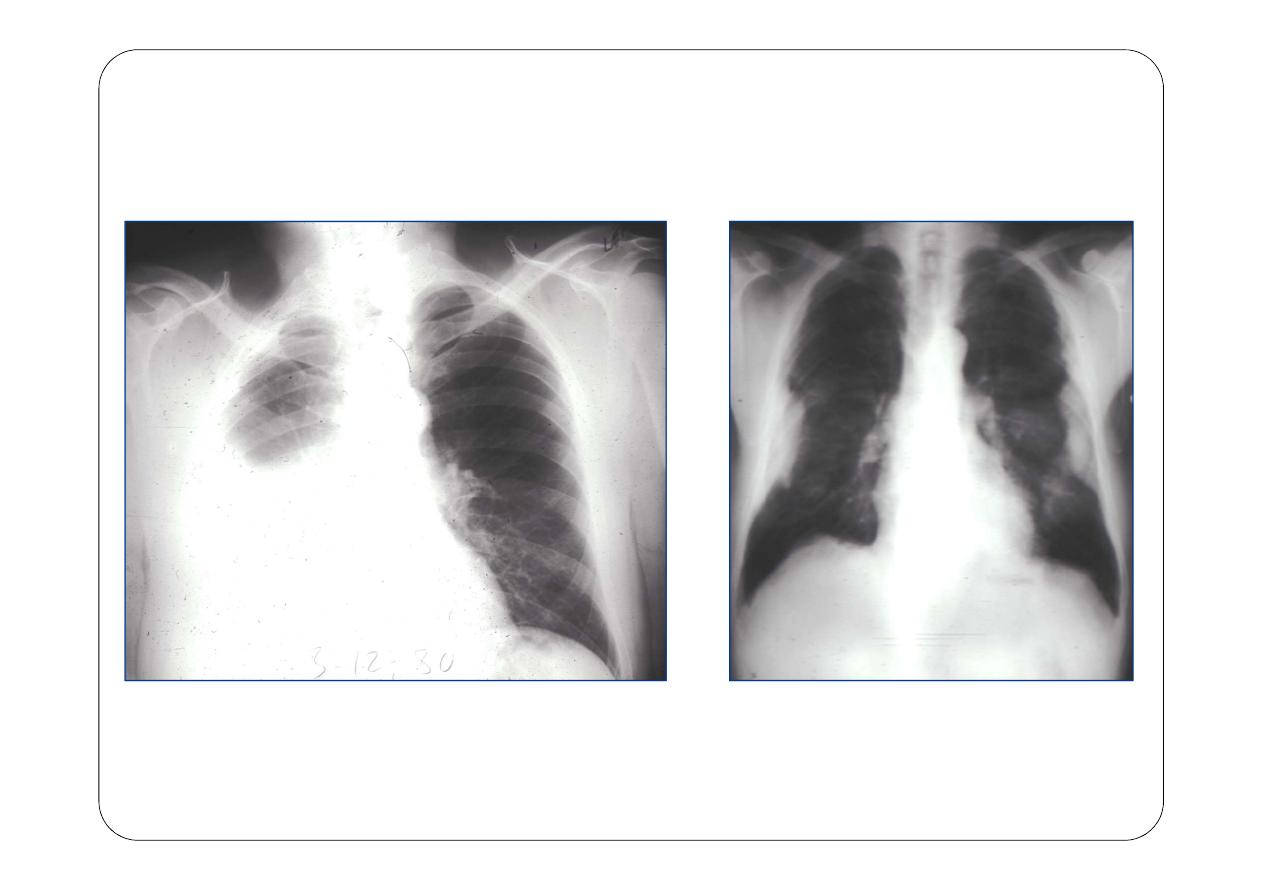
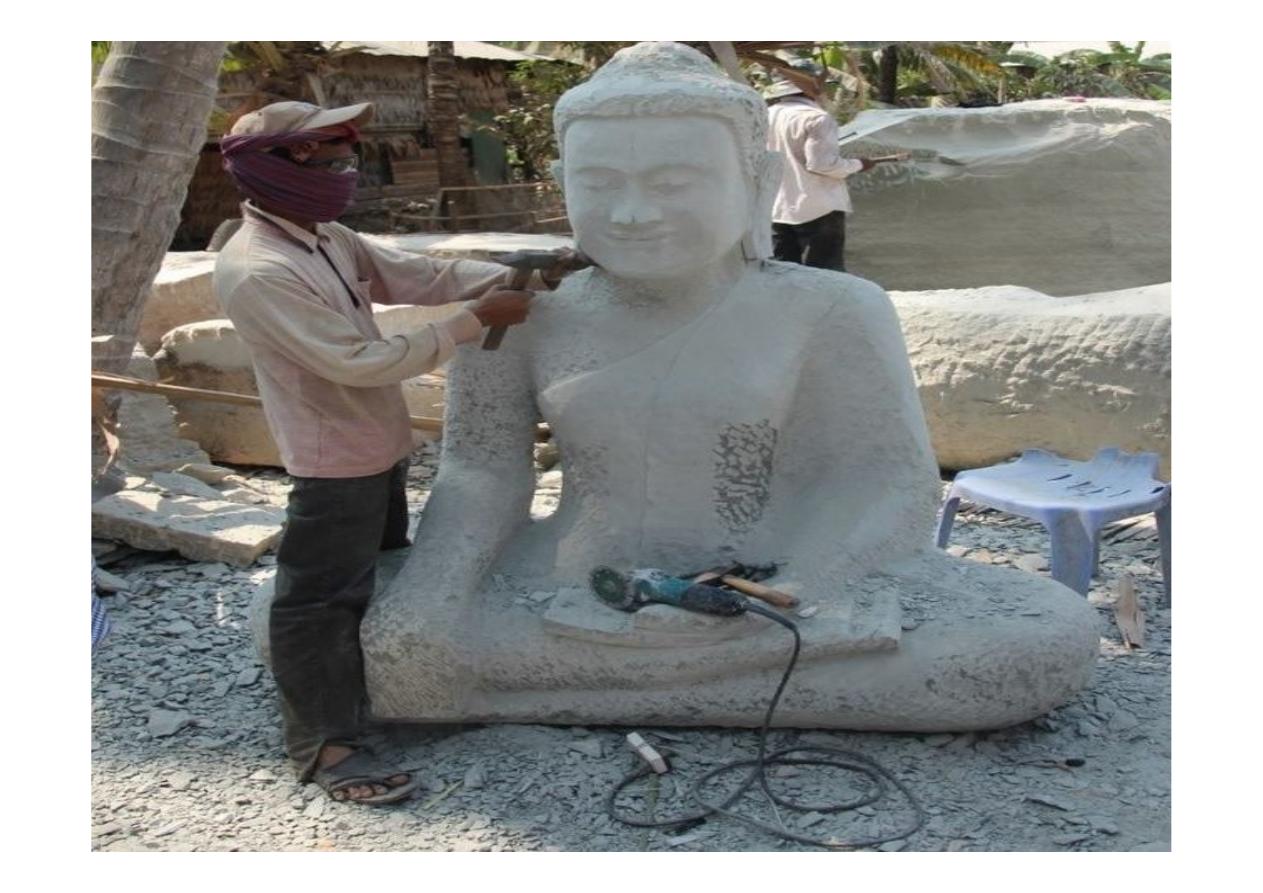
Silicosis
Silicosis
•
Occupational lung disease caused by inhalation of crystalline
silica dust
•
Marked by inflammation and scarring in the form of nodular
lesions in the upper lobes of the lungs.
Silicosis is caused by inhalation of unbound (free) crystalline
silica dust
Characterized by nodular pulmonary fibrosis.
Chronic silicosis initially causes no symptoms or only mild
dyspnea.
But over years can advance to involve most of the lung and
cause dyspnea, hypoxemia, pulmonary hypertension, and
respiratory impairment.
Diagnosis is based on history and chest x-ray findings.
No effective treatment exists except supportive care and, for
severe cases, lung transplantation.
Workers at greatest risk are those who move or blast rock
and sand (miners, quarry workers, stonecutters) or who use
silica-containing rock or sand abrasives (sand blasters; glass
makers; foundry, gemstone, and ceramic workers; potters).
Coal miners are at risk of mixed silicosis and coal workers’
pneumoconiosis
Factors that influence the likelihood of development of silicosis
include
Duration and intensity of exposure
Form of silica
Surface characteristics (exposure to the uncoated form poses
greater risk than the coated form)
Rapidity of inhalation after the dust is fractured and becomes
airborne (exposure immediately after fracturing poses
greater risk than delayed exposure)
It is found in many
rocks
, such as granite, sandstone, gneiss and
slate, and in some
metallic ores
.
Silica can be a main component of sand. It can also be in soil,
mortar, plaster, and shingles.
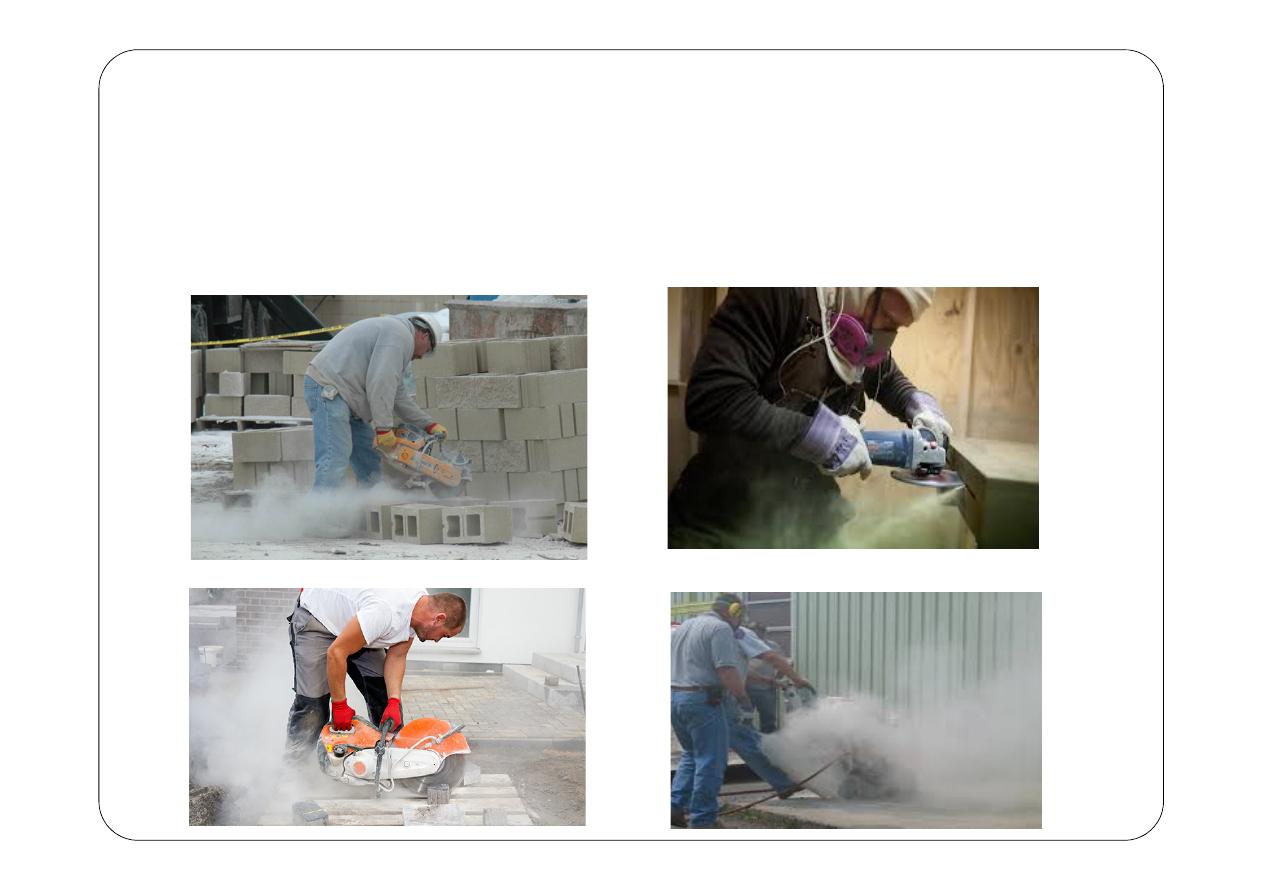
The cutting, breaking, crushing, drilling, grinding, or abrasive
blasting of these materials may produce fine to ultra fine airborne
silica dust.

Pathophysiology
When silica dust particles are
inhaled
→
embed
deeply
into the tiny
alveolar sacs
and
ducts
in the lungs.
There, the lungs
cannot
clear out the dust by mucous or
coughing.
crystalline silica dust
deposited
in the lungs
→
macrophages
ingest
the dust particles
→
inflammation response
→
produce
collagen
around the silica particle
→
fibrosis
and the formation of the
nodular lesions.
There is only abnormal chest X-ray in the beginning and then slowly
develop a cough and breathing difficulty.
More than a third of people with silicosis have phlegm production and
cough
Chronic bronchitis-like
symptoms may occur, and the lungs have
additional sounds called wheezes and crackles.
Compensatory emphysema may develop also.
Classification of silicosis
1.
Chronic simple silicosis :
long-term exposure (10 years
or more) + low concentrations of silica dust → appearing 10–
30 years after first exposure.
Often asymptomatic, but many patients eventually develop dyspnea
during exertion that progresses to dyspnea at rest.
Productive cough, when present, may be due to silicosis, coexisting
chronic occupational (industrial) bronchitis, or smoking.
Breath sounds diminish as the disorder progresses, and pulmonary
consolidation, pulmonary hypertension, and respiratory failure
with or without right ventricular failure may develop in
advanced disease.
2.
Accelerated silicosis
: Patients often experience the same
symptoms as those with chronic silicosis, but symptoms
develop over a shorter period.
develops 5–10 years after first exposure to higher
concentrations of silica dust
2.
Acute silicosis :
-develops a few weeks to 5 years after exposure to high
concentrations of silica dust
- Patients experience rapid progression of dyspnea, weight
loss, and fatigue with diffuse bilateral crackles.
-Respiratory failure often develops within 2 yr.
4. Complicated silicosis :
complicated by
1.
progressive Massive fibrosis
Also patients with silicosis are at risk of other disorders:
1.
Progressive systemic sclerosis
2.
Tuberculosis
3.
Nocardiosis
4.
Lung cancer
5.
Chronic kidney disease
6.
Possibly rheumatoid arthritis
Prevention
The most effective preventive interventions for silicosis occur
at an industrial rather than clinical level and include
dust suppression, process isolation, ventilation, and use of
non–silica-containing abrasives.
Respiratory masks provide imperfect protection and,
although helpful, are not an adequate solution.
Surveillance of exposed workers with respiratory
questionnaires, spirometry, and chest x-rays is
recommended.
Other preventive measures include smoking cessation and
pneumococcal and influenza vaccination.
2. Hypersensitivity pneumonitis (HP),
also known as extrinsic allergic alveolitis,
Granulomatous
inflammatory reaction caused by an
immunological response to certain inhaled
organic dusts
and
some low molecular weight chemicals.
Diagnosis based on history, physical examination, and
radiographic findings.
Hypersensitivity Pneumonitis (Cont.),
Patients may report fever, chills, malaise, cough, dyspnea,
and headaches 4-6 hours after heavy exposure to an inciting
agent in
acute HP.
Chronic
extrinsic allergic alveolitis is caused either by
chronic exposure to low doses of the causative antigen, or as
a consequence of repeated attacks of acute alveolitis over
many years.
Characterized by cough, progressive dyspnea, fatigue,
anorexia, and weight loss.
On examination, patients may present with fever, tachypnea,
and diffuse fine basilar crackles; with muscle wasting,
clubbing, and respiratory distress in severe cases.
Chest radiographs may show micronodular or reticular
opacities in acute or subacute HP and progressive fibrosis
with lung volume loss in chronic HP.
Bagassosis: This is a form of Hypersensitivity Pneumonitis
which is caused as a result of exposure to sugarcane fiber
waste.
Bird Fancier's Lung caused as a result of dust present in the
feathers of birds.
Farmers Lung: induced by the inhalation of biologic dusts
coming from hay dust or mold spores or any
other agricultural products


Lung Cancer
A number of occupations or occupational exposures are
established or suspected risk factors for lung cancer.
The International Agency for Research on Cancer has
identified some occupational exposure factors as being
carcinogenic to the human lung (aluminum production,
arsenic, asbestos, beryllium, cadmium, hexavalent chromium
and coal gasification fumes, crystalline silica, nickel, radon,
and soot)
Depending on the agent, additive or multiplicative modes of
interaction have been shown to operate with cigarette
smoking.
The majority of these cancers are caused by asbestos,
followed by radon, silica, chromium.
Cigarette smoke and asbestos interact strongly in causing
bronchogenic carcinomas, and the risk of carcinoma is
greater in persons with the interstitial fibrosis of asbestosis.
Lung infections:
contact with other people who are ill
infected from a source at work, such as a contaminated
humidifier.
Influenza and other infections such as tuberculosis or
legionella can be occupational infections.
