1
Breast Pathology
Fourth Stage /Lec.no.2
Dr. Rawaa Ghalib
Benign Epithelial Lesions
The benign epithelial lesions of the breast have been divided into three
groups, according to the risk of developing breast cancer :
(1) Nonproliferative breast changes.
(2) Proliferative breast disease.
(3) Atypical hyperplasia.
Nonproliferative Breast Changes (Fibrocystic Changes)
These lesions might come to clinical attention when they mimic carcinoma by
producing palpable lumps, mammographic densities or calcifications, or
nipple discharge.
Fibrocystic disease is most frequently seen, between the ages of 25 and 45
years. the exact pathogenesis remains unknown ,and its primarily affects the
TDLU. The involved areas, by palpation, may have an ill-defined diffuse
increase in consistency as well as discrete nodularities. Cysts are the most
common cause of a palpable mass and are alarming when they are solitary,
firm.
Fibrocystic changes includes a number of morphologic changes which
includes: cystic changes, fibrosis, adenosis.
Morphology.
(1) Cystic change:
Small cysts form by the dilation of lobules, and it may coalesce to form larger
cysts. Cysts are lined either by a flattened atrophic epithelium or by
metaplastic apocrine cells
(
cells have an abundant granular, eosinophilic
cytoplasm, with round nuclei) This is a very common change. There is no
evidence that patients with atypical apocrine metaplasia are at an
2
increased risk for the development of carcinoma.The cysts either contain
turbid or semi-translucent fluid.
(2) Fibrosis:
Cysts frequently rupture, releasing secretory material into the adjacent stroma.
The resulting chronic inflammation and fibrosis contribute to the palpable
firmness of the breast.
(3) Adenosis :
Adenosis is defined as an increase in the number of acini per lobule. A normal
physiologic adenosis occurs during pregnancy.In nonpregnant women,
adenosis can occur as a focal change. The acini are often enlarged but are not
distorted as seen in sclerosing adenosis . Calcifications are occasionally
present within lumens .
Proliferative Breast Disease without Atypia
These lesions are characterized by proliferation of ductal epithelium and/or
stroma without cytologic or architectural features suggestive of carcinoma.
These changes includes: moderate or florid epithelial hyperplasia, sclerosing
adenosis, papilloma, complex sclerosing lesion (radial scar) and
fibroadenoma.
These changes rarely form palpable masses. More commonly, they are
detected as mammographic densities (e.g., complex sclerosing lesions or
sclerosing adenosis), as calcifications (e.g., sclerosing adenosis), or as
incidental findings in biopsies performed for other reasons (e.g.,
hyperplasia), as nipple discharge ( more than 80% of large duct papillomas
produce a nipple discharge).
Although each lesion can be found in isolation, typically more than one lesion
is present together.
1-Epithelial Hyperplasia: Normal breast ducts and lobules are lined by a
double layer of basally located myoepithelial cell layer (cells with dark,
compact nuclei and scant cytoplasm) and luminal cell layer (cells with larger
oval nuclei, and more abundant cytoplasm), epithelial hyperplasia is defined
by the presence of more than two cell layers.

3
2-Sclerosing Adenosis: The number of acini per terminal duct is increased to
at least double the number found in uninvolved lobules. The average age of
the patient is about 30 years.
The normal lobular arrangement is maintained. The acini are compressed and
distorted by dense stroma in the central portions of the lesion but
characteristically dilated at the periphery.
The elongated and compressed
proliferating tubules are lined by two cell types that are themselves elongated
along the tubular axisie i.e myoepithelial cells are usually prominent.
Calcifications are frequently present within the lumens of the acini and
necrosis are absent.
3-Papillomas
Its neoplastic papillary growth within a duct. Intraductal papilloma of the
breast occurs at an average age of 48 years. It can arise in large or small
ducts; clinically
it can give rise to bloody nipple discharge and may be
palpable in a subareolar location.
Gross features: the lesion is usually solitary (approximately 90% of cases
are solitary), soft and fragile,but its diameter rarely exceeds 3 cm, a point of
importance in the differential diagnosis with papillary carcinoma
,.
Microscopical features:: Papillomas are composed of multiple branching
fibrovascular cores, each having a connective tissue axis lined by luminal and
myoepithelial cells, growth occurs within a dilated duct.
4-Fibroadenoma
This is the most common benign tumor of the female breast, most occur in
women in their 20s and 30s, and they are frequently multiple and bilateral.
The epithelium of the fibroadenoma is hormonally responsive, and an
increase in size during pregnancy, which may be complicated by infarction
and inflammation.
Fibroadenomas were originally grouped with other “proliferative changes
without atypia” in conferring a mild increase in the risk of subsequent cancer.
However, in one study the increased risk was limited to fibroadenomas
associated with cysts larger than 0.3 cm, sclerosing adenosis, epithelial
calcifications, or papillary apocrine change (“complex fibroadenomas”)
4
Morphology of fibroadenoma:
Gross features:
The tumor is freely movable, spherical, well-circumscribed, rubbery, grayish
white nodules that vary in size from less than 1 cm to large tumors may reach
up to 10 cm in diameter
.
large tumors are referred to as giant fibroadenoma
and often contain slitlike spaces.
Microscopical features
There is a loose fibroblastic stroma containing epithelium– lined duct- like
spaces of various forms and sizes,with presence of fibrous capsule .
There are intracanalicular when the connective tissue invaginates into the
glandular spaces so that it appears to be within them, and pericanalicular
when the regular round or oval glandular configuration of the glands is
maintained. Often, both types of growth are seen in the same lesion. The
tubules are composed of cuboidal or low columnar cells with round uniform
nuclei resting on a myoepithelial cell layer. In older women, the stroma
typically becomes densely hyalinized and the epithelium atrophic and may
calcify.
Proliferative Breast Disease with Atypia
Proliferative disease with atypia includes
1 - Atypical ductal hyperplasia
2 - Atypical lobular hyperplasia.
Atypical ductal hyperplasia is present in 5% to 17% of specimens from
biopsies performed for calcifications and is found less frequently in
specimens from biopsies for mammographic densities or palpable masses.
Atypical lobular hyperplasia is an incidental finding and is found in fewer
than 5% of specimens from biopsies performed for any reason.
5
Morphology
Atypical ductal hyperplasia
It consists of a relatively monomorphic proliferation of regularly spaced cells,
sometimes with cribriform spaces. It is distinguished from DCIS by being
limited in extent and only partially filling ducts.
Atypical lobular hyperplasia
It consists of a proliferation of cells identical to those of lobular carcinoma in
situ, but the cells do not fill or distend more than 50% of the acini within a
lobule.
Clinical Significance of Benign Epithelial Changes
Multiple epidemiologic studies have classified the benign changes in the
breast and determined their association with the later development of invasive
cancer.
Nonproliferative changes do not increase the risk of cancer.
Proliferative disease is associated with a mild increase in risk.
Proliferative disease with atypia confers a moderate increase in risk.
Both breasts are at increased risk.
Risk reduction can be achieved by bilateral prophylactic mastectomy or
treatment with estrogen antagonists, such as tamoxifen.
However, more than 80% of women with atypical hyperplasia will not
develop breast cancer, and many choose careful clinical and radiologic
surveillance over intervention.
6
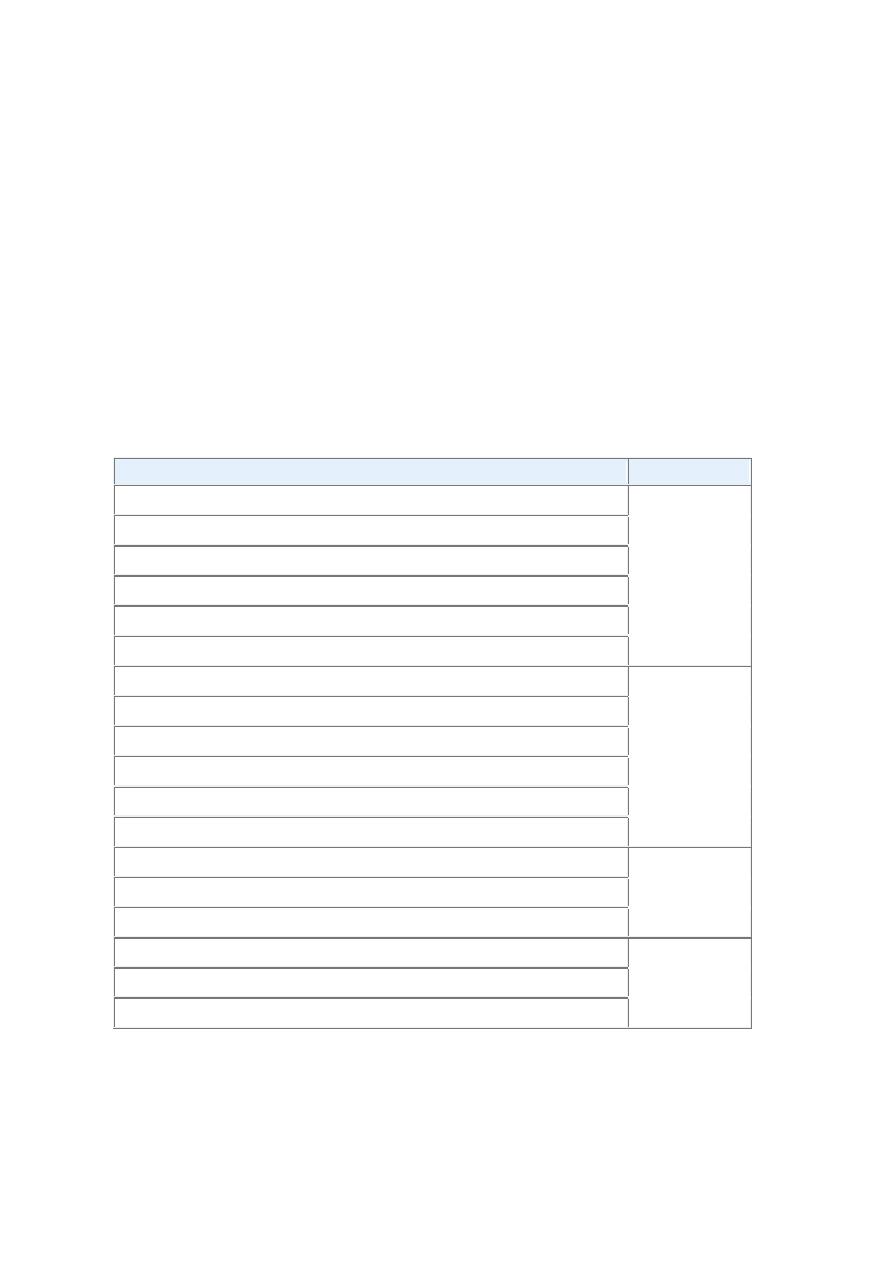
Table-Epithelial breast lesions and the risk of developing invasive carcinoma.
Pathologic Lesion
Relative Risk
Nonproliferative Breast Changes (Fibrocystic changes)
1.0
Duct ectasia
Cysts
Apocrine change
Mild hyperplasia
Adenosis
Proliferative Disease Without Atypia
1.5 to 2.0
Moderate or florid hyperplasia
Sclerosing adenosis
Papilloma
Complex sclerosing lesion (radial scar)
Fibroadenoma with complex features
Proliferative Disease With Atypia
4.0 to 5.0
Atypical ductal hyperplasia (ADH)
Atypical lobular hyperplasia (ALH)
Carcinoma In Situ
8.0 to 10.0
Lobular carcinoma in situ (LCIS)
Ductal carcinoma in situ (DCIS)
The next lecture is about carcinoma of breast