
Management
The sole objective of antihypertensive therapy is to reduce the
incidence of adverse cardiovascular events, particularly coronary
artery disease, stroke and heart failure.
The relative benefit of antihypertensive therapy (approximately
30% reduction in risk of stroke and 20% reduction in risk of
coronary heart disease) is similar in all patient groups, so the
absolute benefit of treatment (total number of events
prevented) is greatest in those at highest risk.
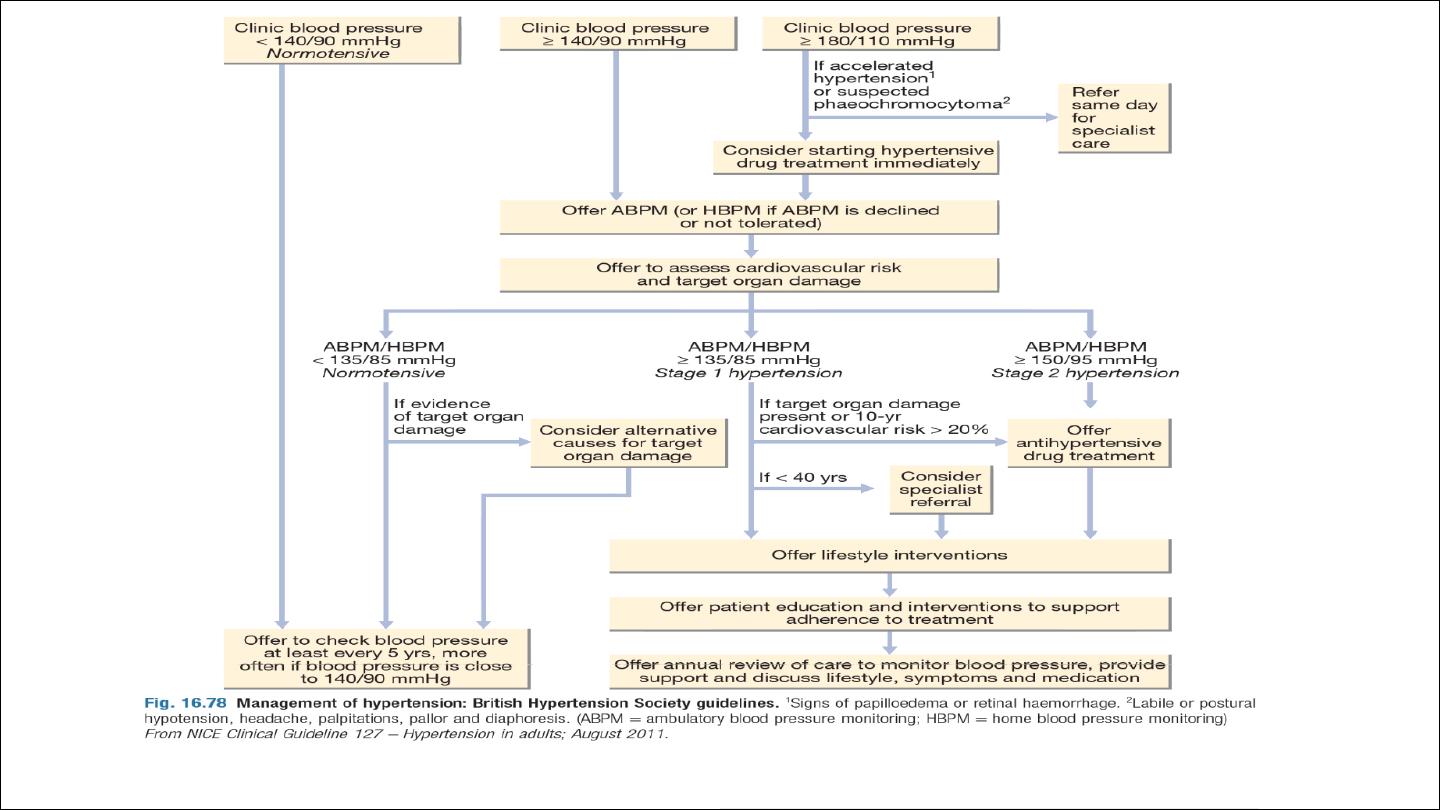
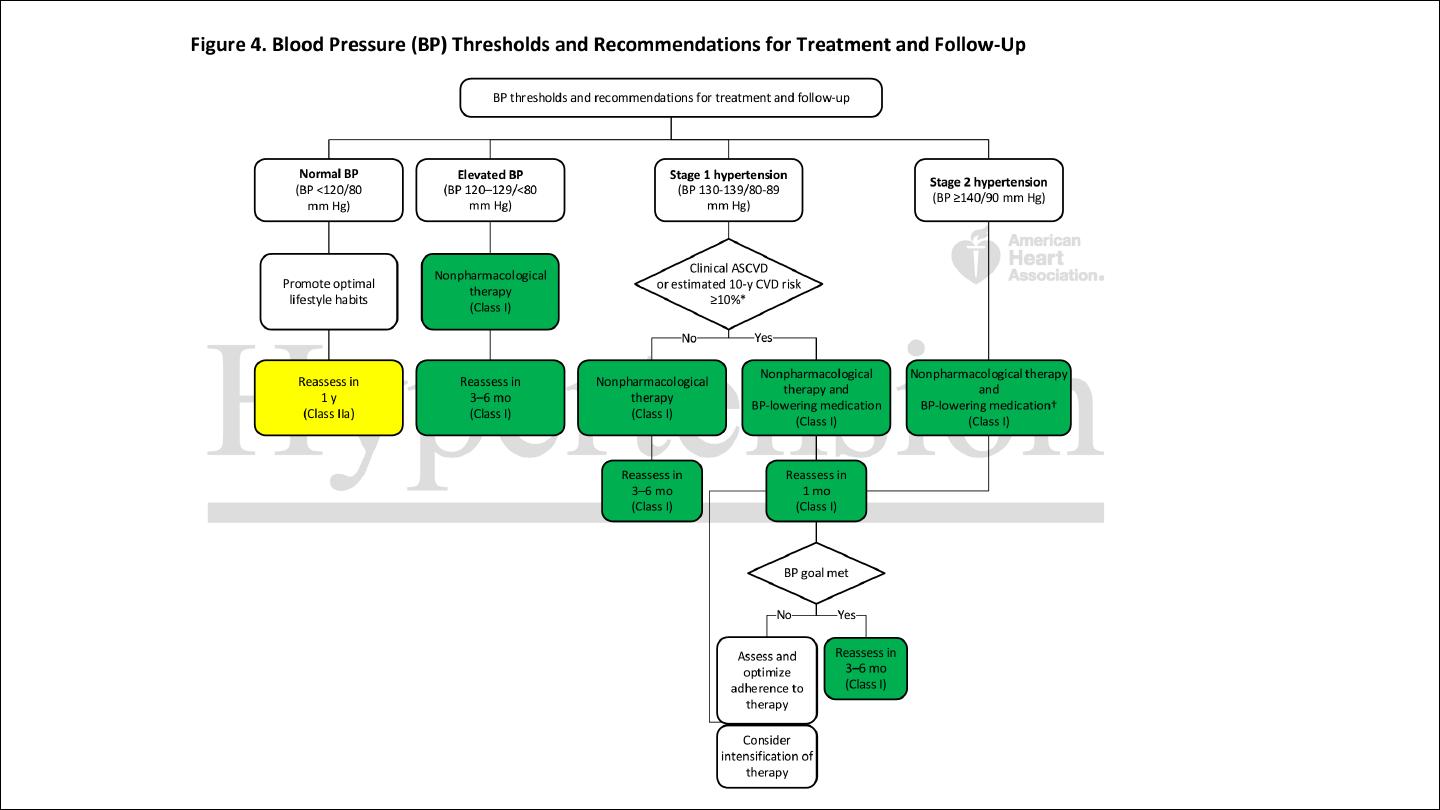
Threshold for intervention
Systolic BP and diastolic BP are both powerful predictors of
cardiovascular risk. The British Hypertension Society
management guidelines therefore utilise both readings, and
treatment should be initiated if they exceed the given threshold
Diabetes and established cardiovascular at particular higher risk, so
the threshold for initiation of therapy is lower.
Patients taking antihypertensive therapy require follow-up at 3 monthly
intervals to monitor BP, minimize side-effects and reinforce lifestyle
advice.
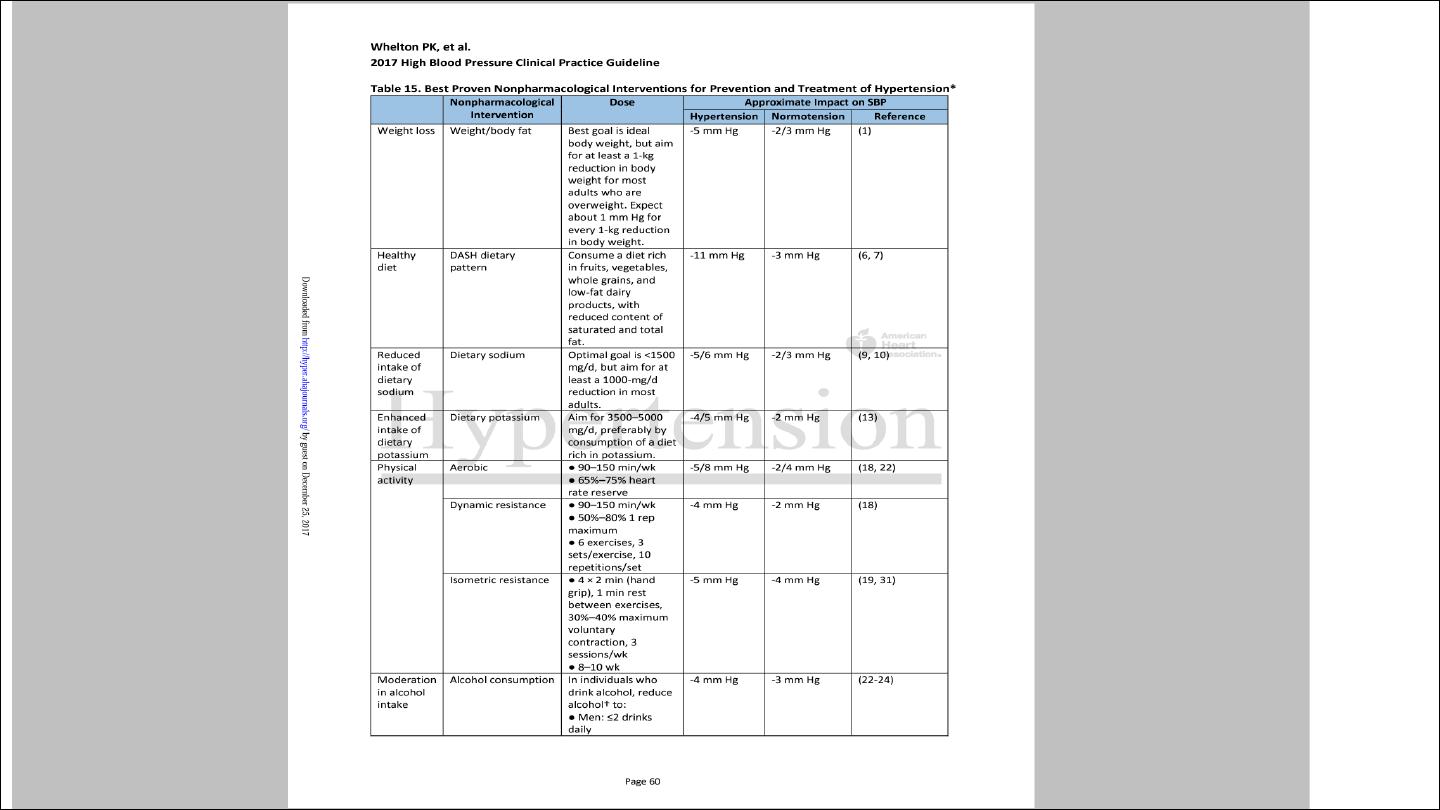
Non drug therapy
Correcting obesity, reducing alcohol intake, restricting salt intake,
taking regular physical exercise and increasing consumption of fruit
and vegetables can all lower BP.
Moreover, quitting smoking, eating oily fish and adopting a diet that is
low in saturated fat may produce further reductions in cardiovascular
risk.

Antihypertensive drugs
Diuretics
Thiazide :
The mechanism of action of these drugs is incompletely understood and it may take up to a
month for the maximum effect to be observed.
e.g Bendroflumethiazide 2.5 mg, Hydrochlorthalidone 50 mg, indapamide 1.5 mg.
S.E : hypokalemia, hyperuremia ( can cause gout), hyperglycemia , hypertriglycerimia
Loop diuretics
: used as antihypertensive in cases with CRF, GFR less than 30 ml/kg/min
Angiotensin converting enzyme inhibitors:
Angiotensin l converted via ACE to angiotensin ll which cause
vasoconstriction and Stimulate the release of aldosterone from adrenals.
Blocking this pathway result in hypotensive effect.
ACE inhibitors should be used with particular care in patients with impaired
renal function or renal artery stenosis because they can reduce the filtration
pressure in the glomeruli and precipitate renal failure.
Electrolyte should be checked 1 to 2 weeks after initiation of therapy up to 30
% woresning in renal function is accepted, more woresning indicate stopping
ACE inhibitors.
e.g Captopril , enalopril, lisinporil, ramipril, perindopril.
S.E: Dry cough 15 %, angioedema 1 %, hyperkalemia, rash, renal
dysfunction, Neutropenia(captopril)

•
Bradykinin is inflammatory mediators which promote vasodilatation,
degraded by ACE, ACE inhibitors result in accumulation of bradykinin
which give additional antihypetensive effect.
•
Bradykinin is the cause of ACE inhibitors dry cough.
•
ACE inhibtors induced dry cough is indication to stop ACE I hibitors and
to swich to ARB
ARB: angiotensin receptor blockers
e.g: Losartan, Valsartan, telmisartan, candesartan, irbesartan.
Block angiotensin 2 receptor.
Combination of ACE and ARB has no additional antihypertensive effect ,
carry high risk of hyperkalemia and should be avoided.
ARB causing No dry cough, no angioedema, but share the same side
effect with ACE inhibitors Hyperkalemia and renal dysfunction.

Calcium channel antagonists
Dihyropyridine: Nifedipine, felodipine, amlodipine
Non dihydropidine : diltiazim, verapamil
S.E: Flushing , leg edema, effect on HR ( tachycardia with
dihydropyridine and bradycardia with non dihydropyridine)
Constipation

Beta-blockers.
These are no longer used as first-line antihypertensive therapy, except
in patients with another indication for the drug (e.g. angina).
Carvedilol and labetalol combined alpha and beta blocker

OTHER DRUGS
q
Alpha blockers: such as prazosin (0.5–20 mg daily in divided doses),
indoramin (25–100 mg twice daily) and doxazosin (1–16 mg daily
q
Alpha methyl dopa
q
Direct vasodilator: hydralazine (25–100 mg twice daily) and minoxidil
(10–50 mg daily).
Side-effects include first-dose and postural hypotension, headache,
tachycardia and fluid retention. Minoxidil also causes increased facial
hair and is therefore unsuitable for female patients.
Choice of antihypertensive
:
Trials that have compared thiazides, calcium antagonists, ACE inhibitors
and angiotensin receptor blockers have not shown consistent differences
in outcome, efficacy, side-effects or quality of life. Beta-blockers, which
previously featured as first-line therapy in guidelines, have a weaker
evidence base.
The choice of antihypertensive therapy is initially dictated by the patient’s
age and ethnic background, although cost and convenience will affect the
exact drug and preparation used. Response to initial therapy and side-
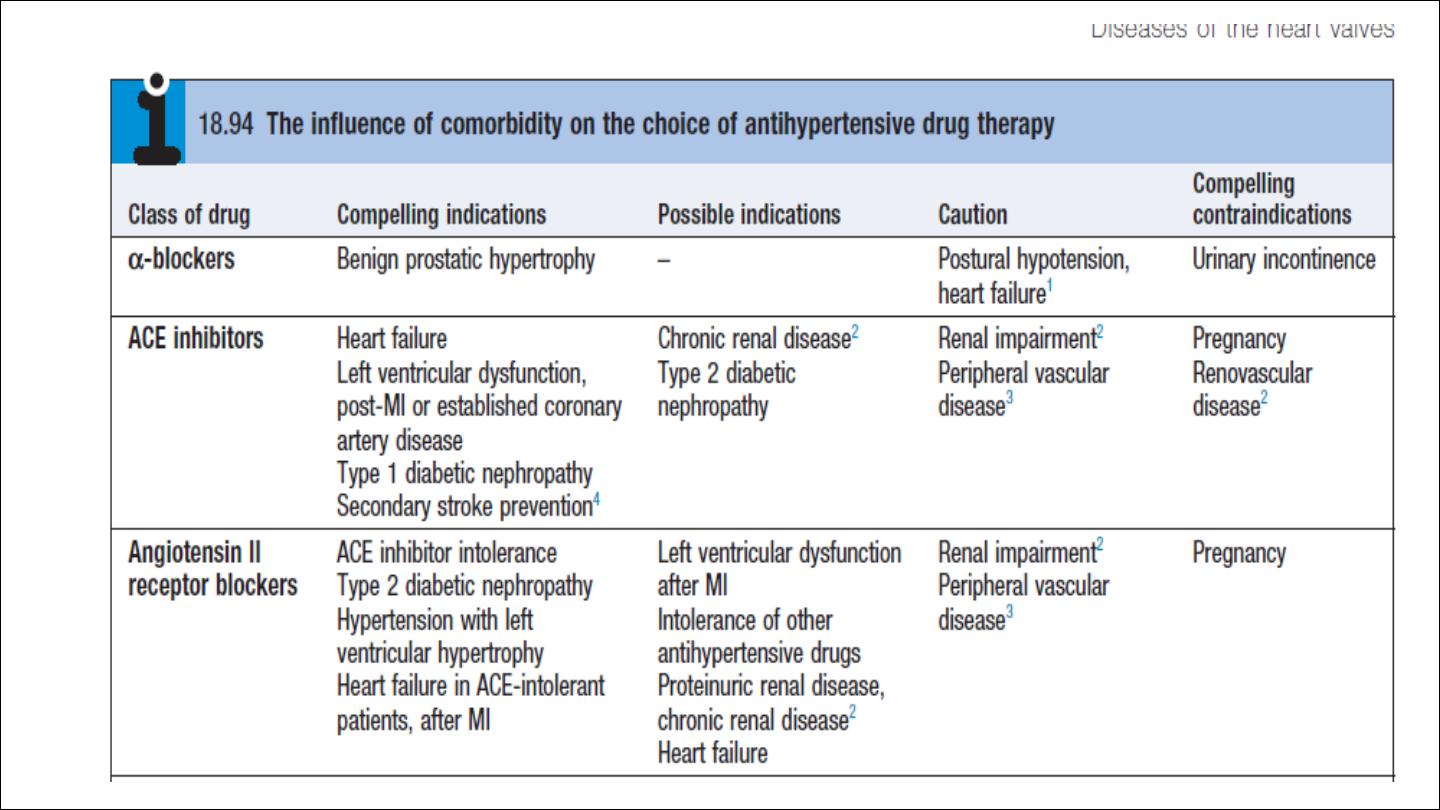
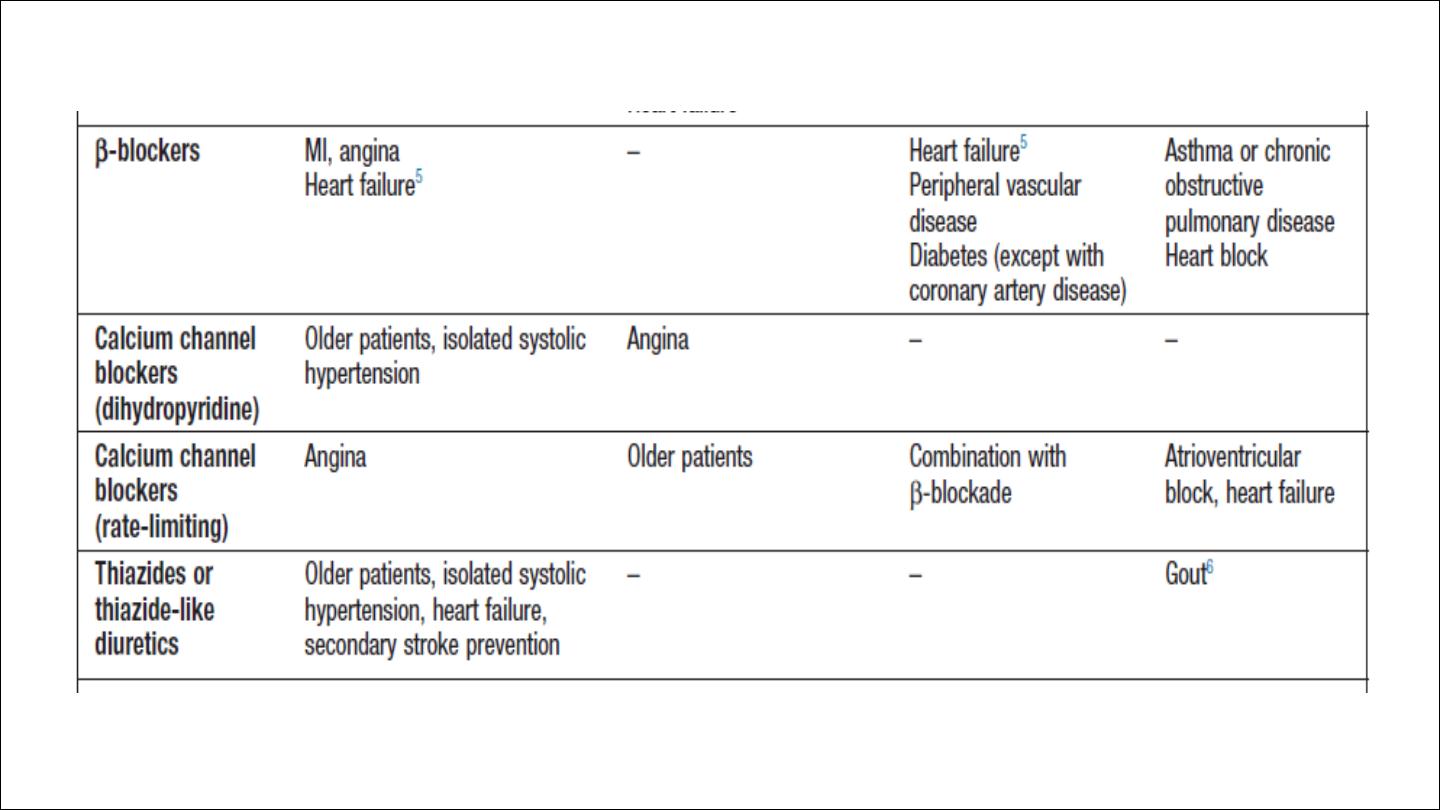
effects dictate subsequent treatment. Comorbid conditions also have an
influence on initial drug selection for example, a β-blocker might be the
most appropriate treatment for a patient with angina. Thiazide diuretics
and dihydropyridine calcium channel antagonists are the most suitable
drugs for the treatment of high BP in older people
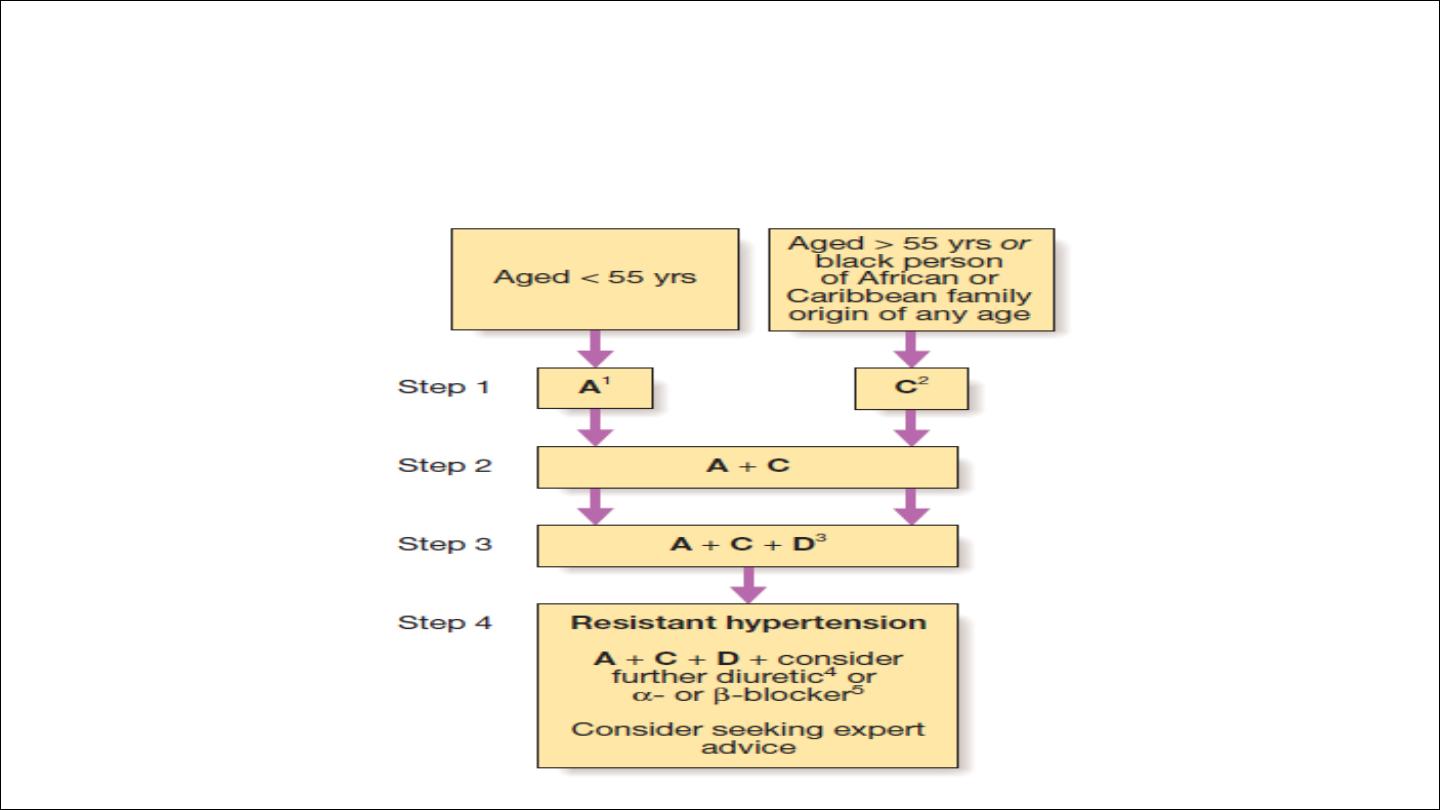
Choice of antihypertensives drugs according to age
q
Combination versus monotherapy
Although some patients can be satisfactorily treated with a single
antihypertensive drug, a combination of drugs is often required to
achieve optimal BP control.
Combination therapy may be desirable for other reasons; for example,
low-dose therapy with two drugs may produce fewer unwanted effects
than treatment with the maximum dose of a single drug. Some drug
combinations have complementary or synergistic actions; for example,
thiazides increase activity of the renin–angiotensin system while ACE
inhibitors block it.
Emergency treatment of accelerated phase or malignant hypertension
In accelerated phase hypertension, lowering BP too quickly may compromise
tissue perfusion (due to altered autoregulation) and can cause cerebral
damage, including occipital blindness, and precipitate coronary or renal
insufficiency.
Even in the presence of cardiac failure or hypertensive encephalopathy, a
controlled reduction to a level of about 150/90 mmHg over a period of 24–48
hours is ideal.
In most patients, it is possible to avoid parenteral therapy and
bring BP under control with bed rest and oral drug therapy.
Intravenous or intramuscular labetalol (2 mg/min to a maximum
of 200 mg), intravenous glyceryl trinitrate (0.6–1.2 mg/hr),
intramuscular hydralazine (5 or 10 mg aliquots repeated at half
hourly intervals) and intravenous sodium nitroprusside (0.3–1.0
μg/kg body weight/min) are all effective but require careful
supervision, preferably in a high dependency unit.

Causes of refractory hypertension:
Poor compliance
Inadeqaute therapy
Secondory cause
Feature suggestive of secondary HPT:
AGE less than 30 , above 55 years, REFRACTORY HPT