
Minor problems of
pregnancy
Objectives:
l
To understand the causes and management of minor
complications of pregnancy.including:
l
Backache
l
Symphysis pubis dysfucnstion
l
Carpal tunnel syndrome
l
Constipation
l
Nausea& Vomiting of pregnancy & hyperemesis
l
Heart burn
l
Haemorrhoids & varicosities
l
Oedema
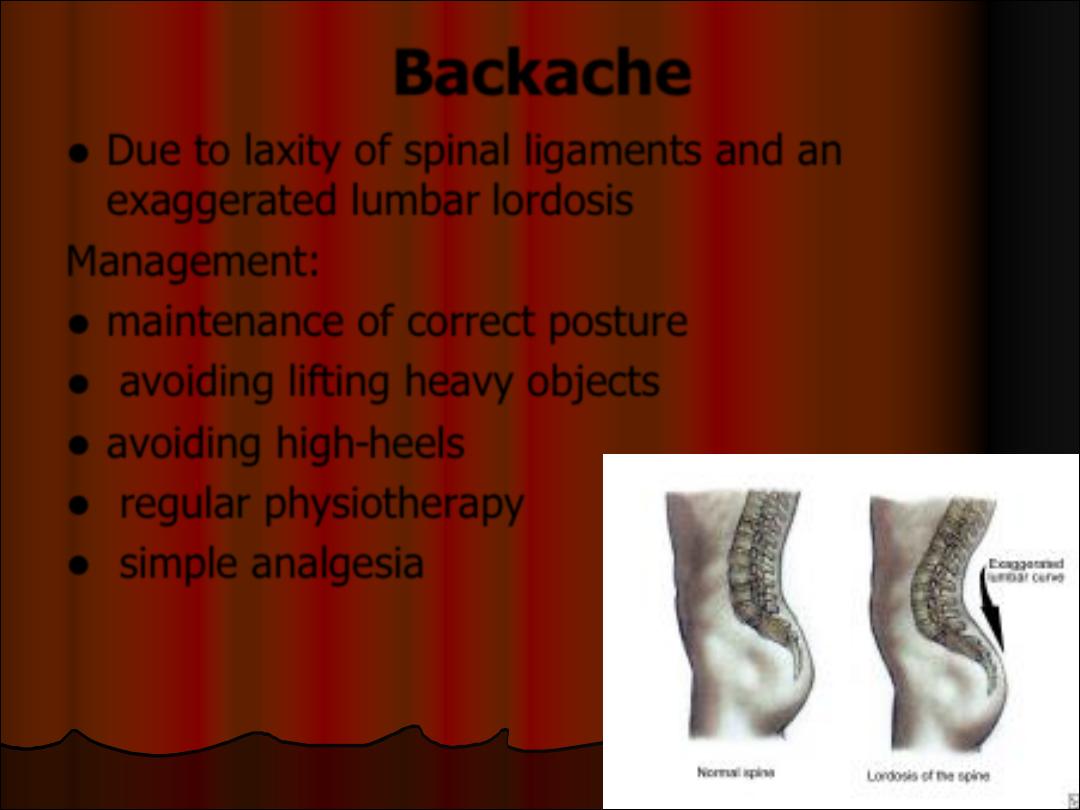
Backache
l
Due to laxity of spinal ligaments and an
exaggerated lumbar lordosis
Management:
l
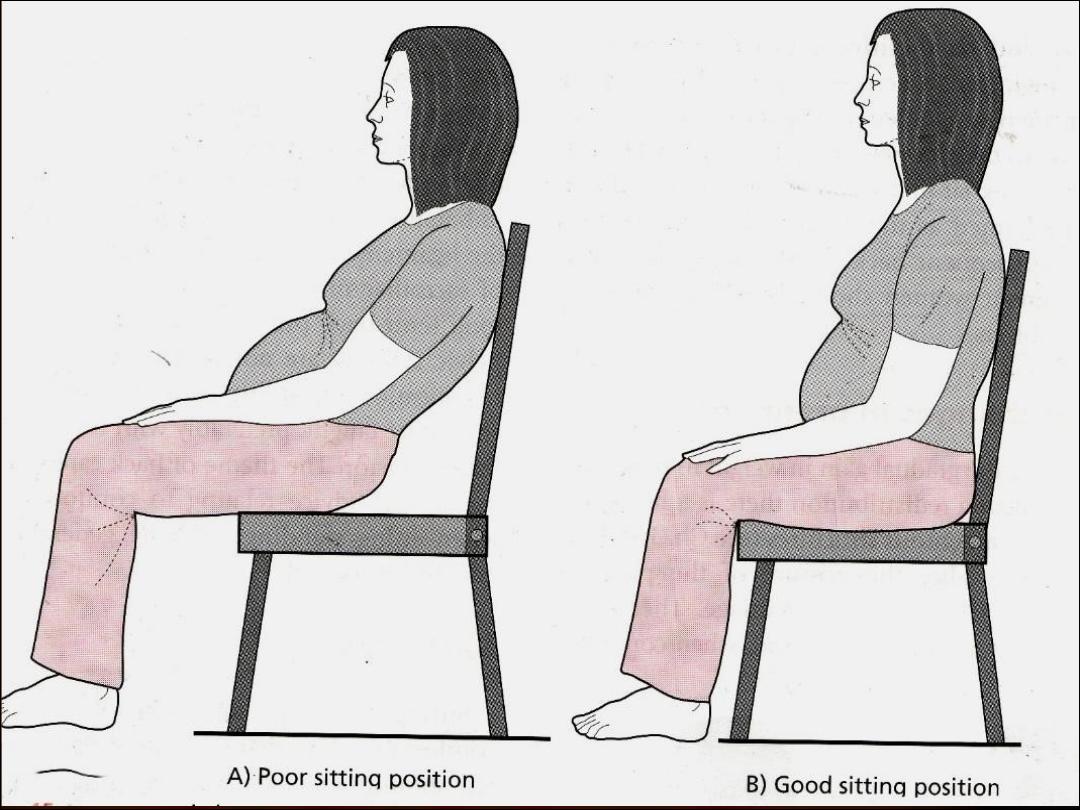
maintenance of correct posture
l
avoiding lifting heavy objects
l
avoiding high-heels
l
regular physiotherapy
l
simple analgesia
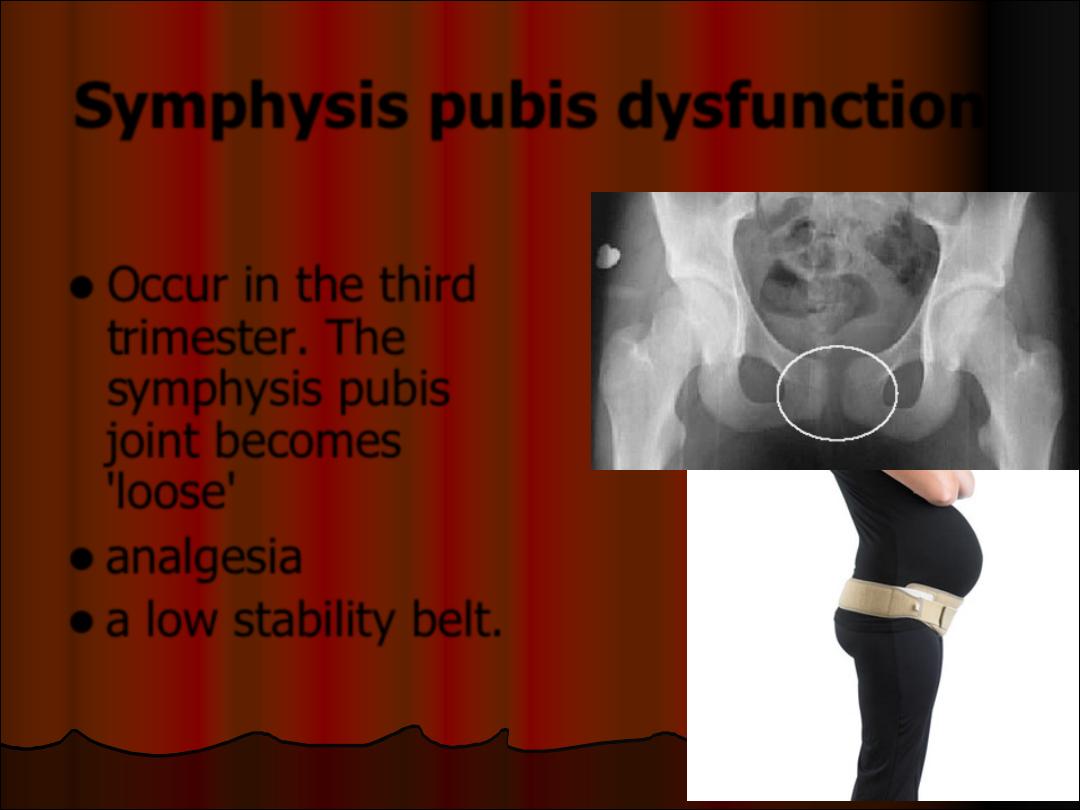
Symphysis pubis dysfunction
l
Occur in the third
trimester. The
symphysis pubis
joint becomes
'loose'
l
analgesia
l
a low stability belt.
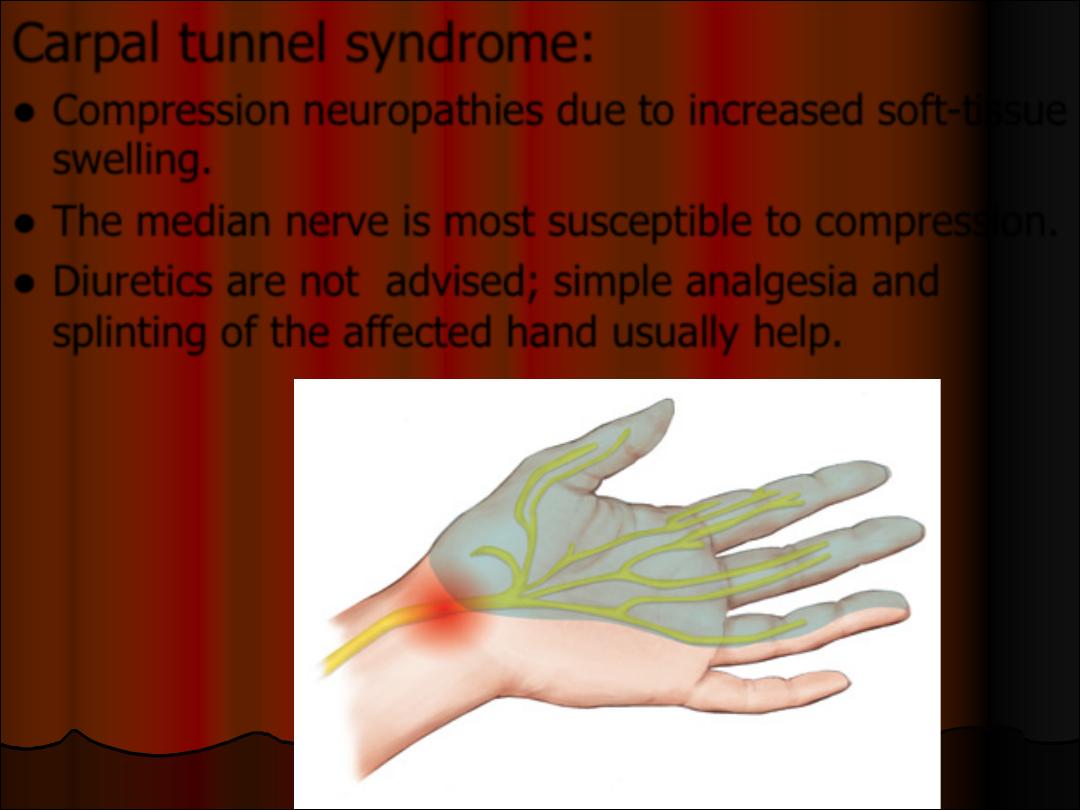
Carpal tunnel syndrome:
l
Compression neuropathies due to increased soft-tissue
swelling.
l
The median nerve is most susceptible to compression.
l
Diuretics are not advised; simple analgesia and
splinting of the affected hand usually help.
Constipation
l
Causes: relaxing effect of progesteron on
GIT, iron therapy, mechanical compression
Management:
l
high-fibre diet
l
increase fluid intake
l
mild (non-stimulant) laxative such as
lactulose.
Nausea & vomiting of pregnancy
& Hyperemesis Gravidarum
l
NVP affects up to 70-80% of pregnants.
l
HG affects about 0.3–2% of pregnant
women
l
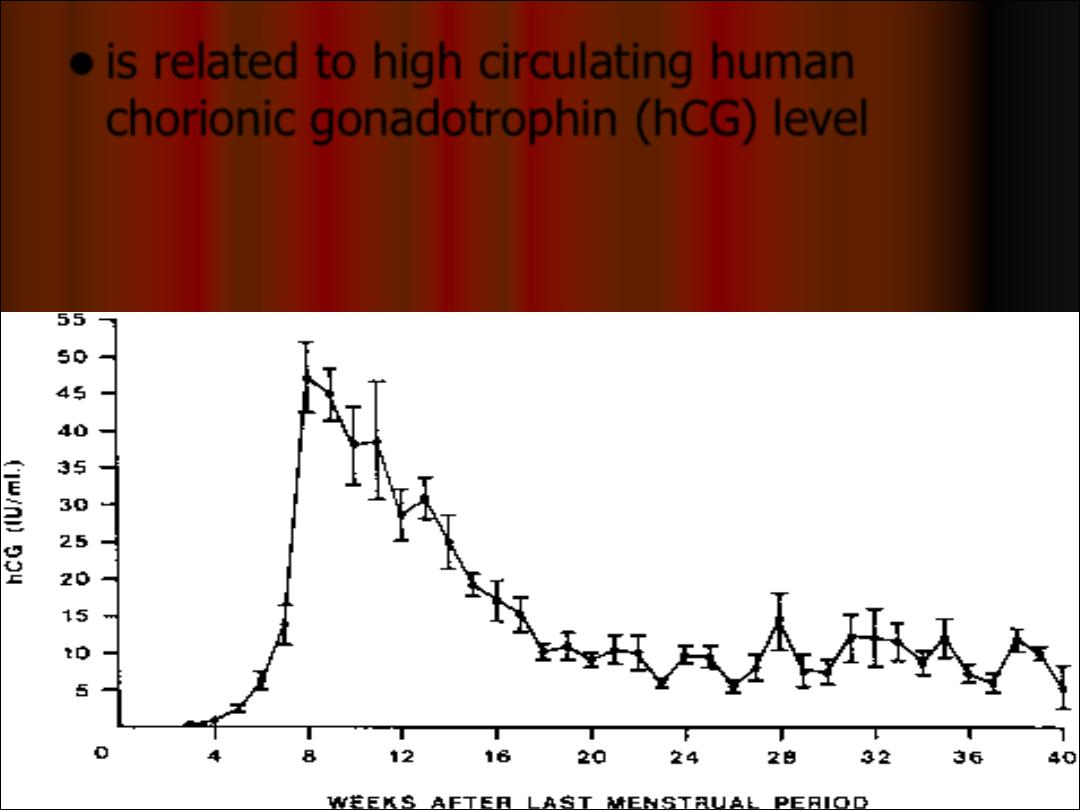
is related to high circulating human
chorionic gonadotrophin (hCG) level
Start at 5-6 weeks' gestation, peek at 9 wks
and improve at 16-20 wk.
Hyperemesis Gravidarum
l
woman is unable to maintain hydration &
nutrition because of severity or duration of
symptoms.
l
HG diagnosed when there is protracted
NVP with the triad of more than 5%
prepregnancy weight loss, dehydration
and electrolyte imbalance.
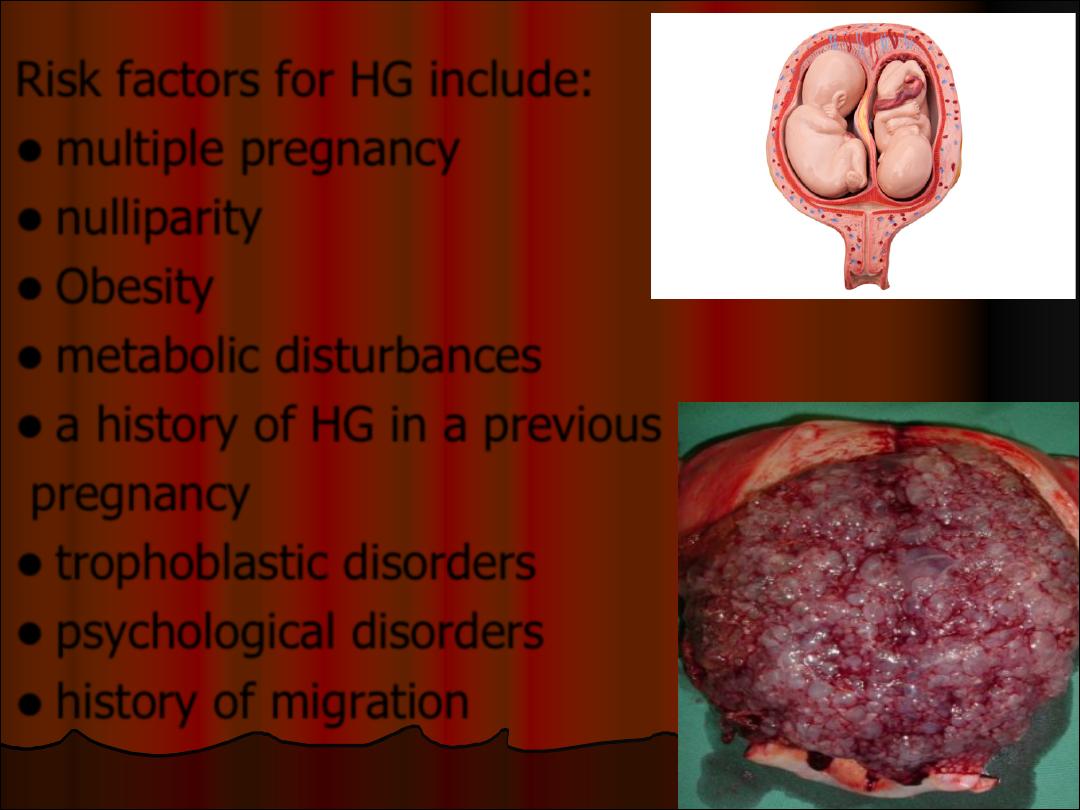
Risk factors for HG include:
l
multiple pregnancy
l
nulliparity
l
Obesity
l
metabolic disturbances
l
a history of HG in a previous
pregnancy
l
trophoblastic disorders
l
psychological disorders
l
history of migration
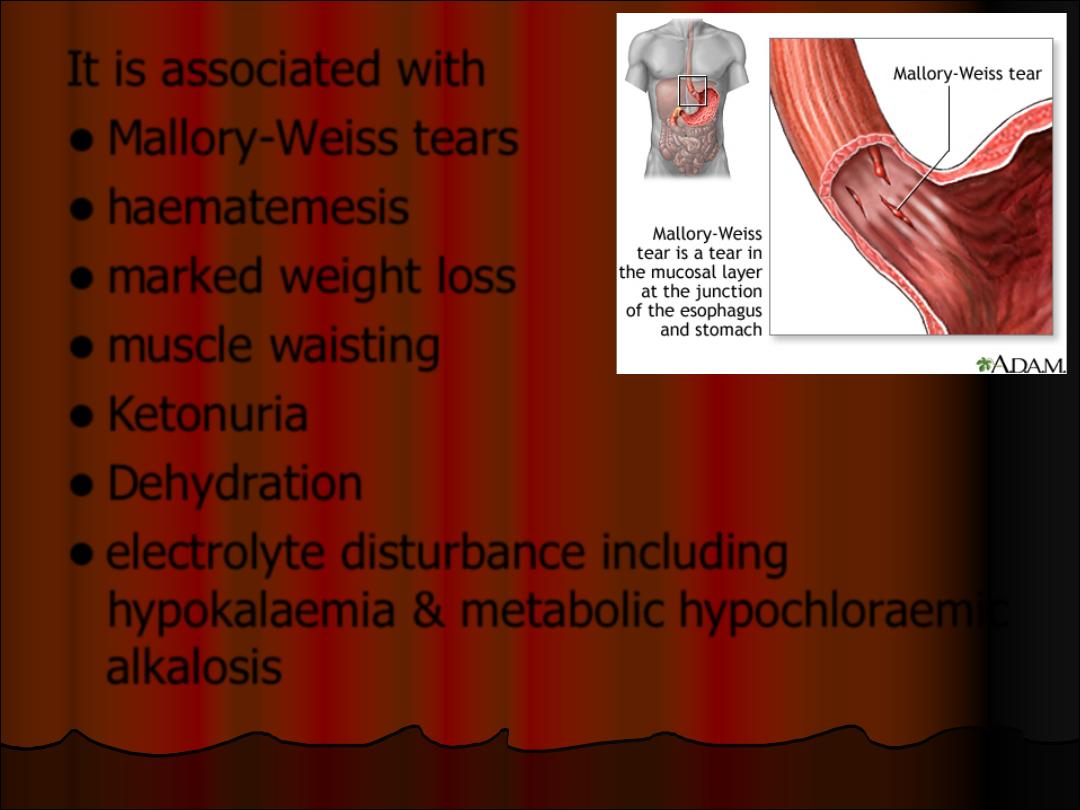
It is associated with
l
Mallory-Weiss tears
l
haematemesis
l
marked weight loss
l
muscle waisting
l
Ketonuria
l
Dehydration
l
electrolyte disturbance including
hypokalaemia & metabolic hypochloraemic
alkalosis
Complications :
l
fetal growth restriction
l
maternal hyponatraemia
l
thiamin deficiency leading to Wernicke's
encephalopathy.
Conditions causing nausea and vomiting in
pregnancy include:
l
Genito-urinary conditions: UTI, pyelonephritis,
ovarian torsion.
l
Endocrine conditions: thyrotoxicosis, diabetic
ketoacidosis, Addison's disease.
l
Gastrointestinal conditions: gastritis, peptic
ulcer, pancreatitis, bowel obstruction, hepatitis,
cholelithiasis, appendicitis.
l
Neurological conditions such as vestibular
disease, migraine.
l
Other pregnancy-related conditions such as
acute fatty liver of pregnancy, pre-eclampsia.
Management:
Exclude other causes of nausea & vomiting
Work up:
•
Urinalysis for ketones and specific gravity
•
Hematocrit
•
Serum electrolytes
•
Liver enzymes and bilirubin
•
An US scan is important to exclude
hydatidiform mole & to diagnose multiple
pregnancy, both of which increase the risk
of hyperemesis.
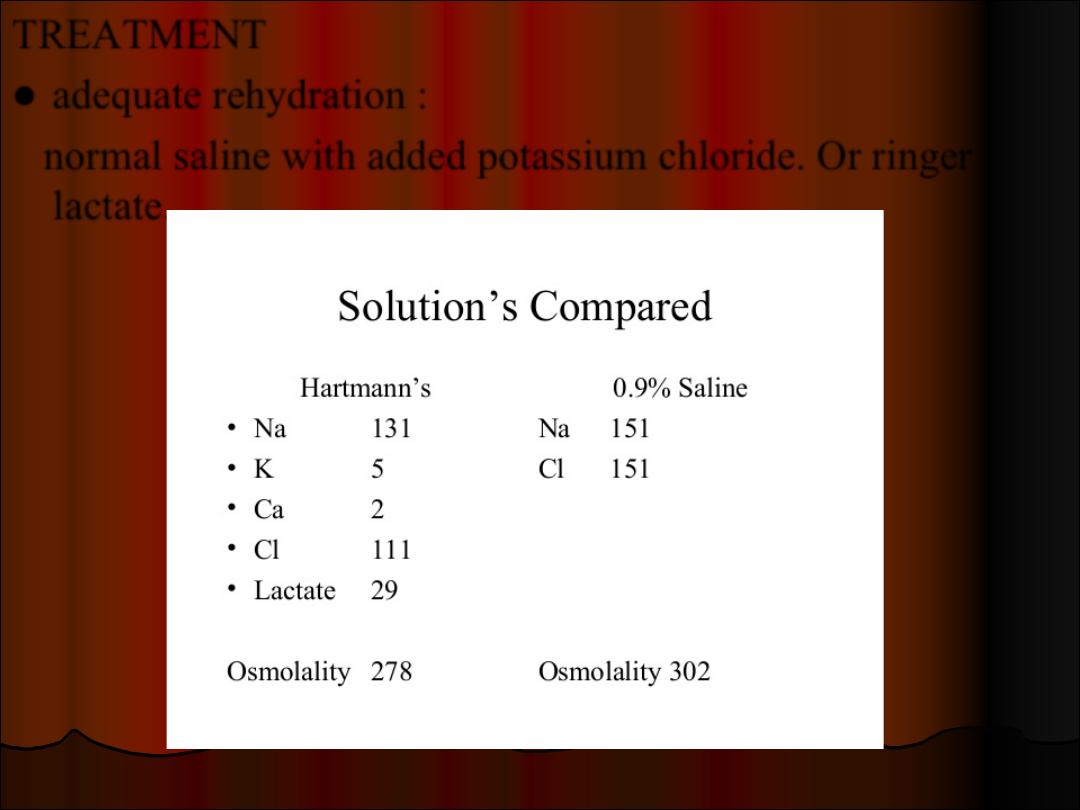
TREATMENT
l
adequate rehydration :
normal saline with added potassium chloride. Or ringer
lactate.
Fluid Replacement
l
If significant ketonuria, 1000 ml 0.9% sodium
chloride intravenously over 2 to 4 hours. Hartmann’s
can also be used.
l
Thereafter fluids should be reduced to 500 ml 4–6
hourly, the regime being guided by U&E results,
which should be performed daily, particularly for
monitoring potassium levels.
l
Avoid glucose initially as it contains insufficient
sodium and especially as Wernicke’s encephalopathy
may be precipitated unless thiamine is given first.
l
Antiemetics such as phenothiazines are safe,
metoclopramide is safe and effective, but
because of the risk of extrapyramidal effects it
should be used as second-line therapy
l
Pyridoxine is not recommended for NVP and
HG
l
Ginger
l
In resistant cases a trial of steroid may be
effective
l
If persistent dehydration, electrolyte loss,
and/or weight loss occur despite above
therapy give Paranteral nutrition
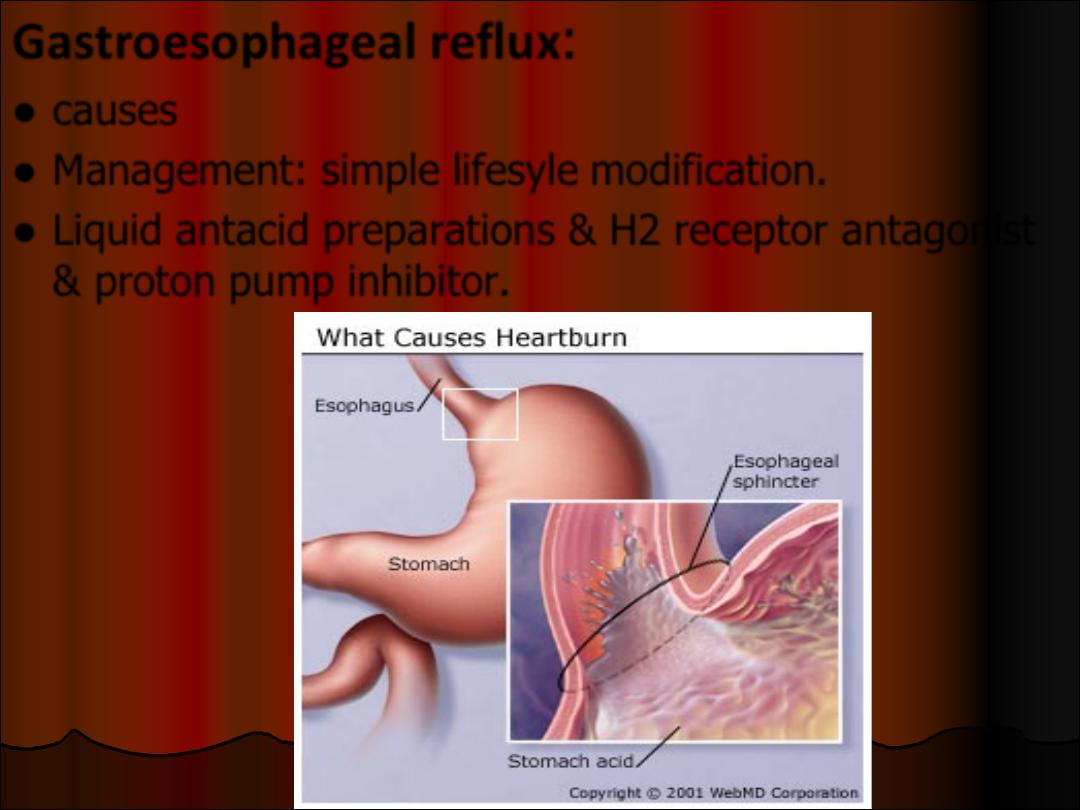
Gastroesophageal reflux
:
l
causes
l
Management: simple lifesyle modification.
l
Liquid antacid preparations & H2 receptor antagonist
& proton pump inhibitor.
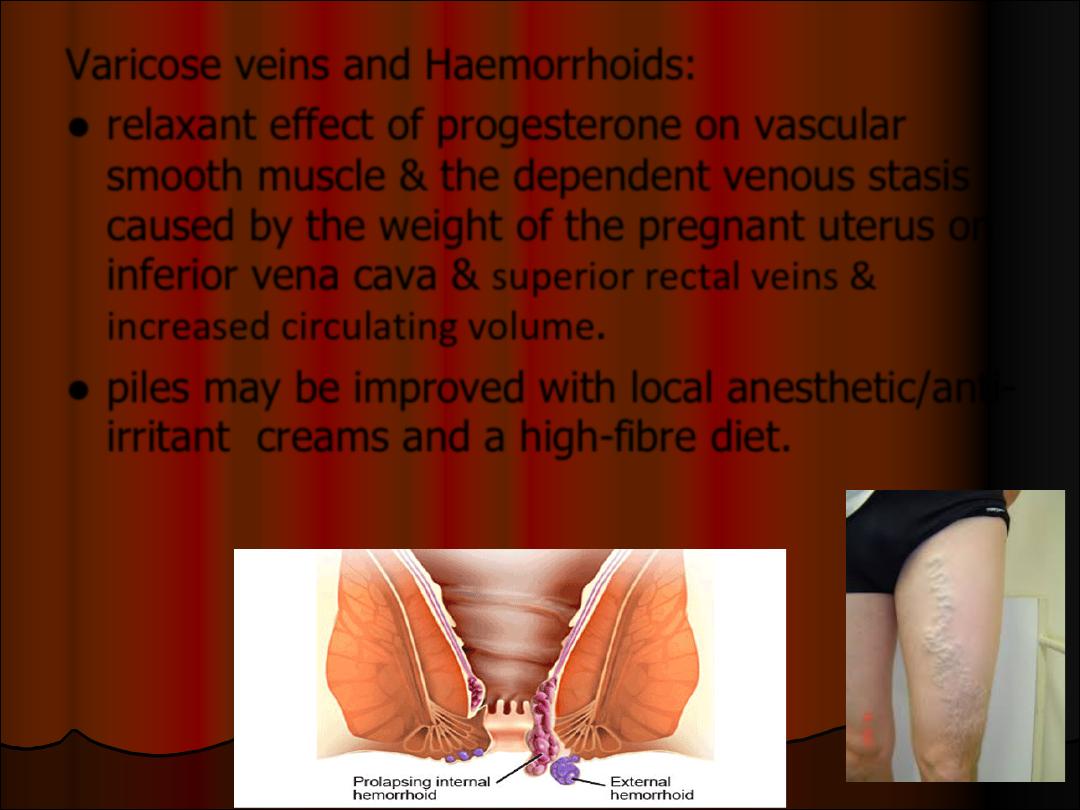
Varicose veins and Haemorrhoids:
l
relaxant effect of progesterone on vascular
smooth muscle & the dependent venous stasis
caused by the weight of the pregnant uterus on
inferior vena cava & superior rectal veins &
increased circulating volume.
l
piles may be improved with local anesthetic/anti-
irritant creams and a high-fibre diet.
l
Varicose veins of the legs may be
symptomatically improved with support
stockings, avoidance of standing for
prolonged periods and simple analgesia
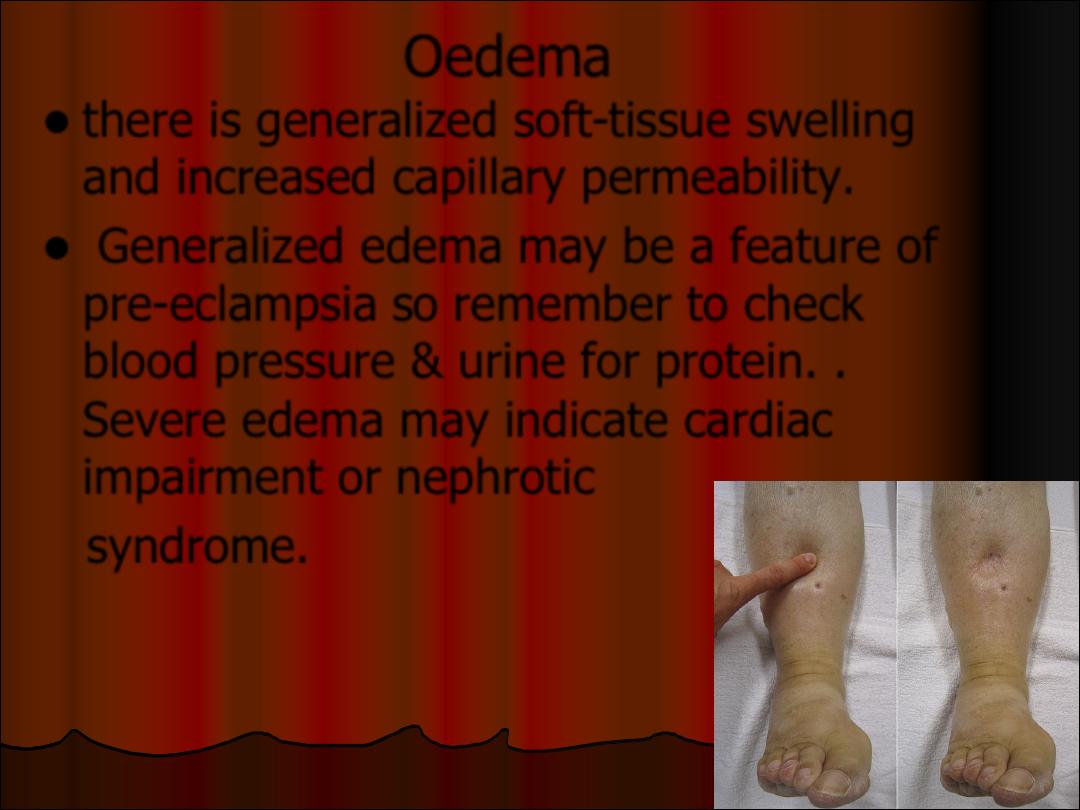
Oedema
l
there is generalized soft-tissue swelling
and increased capillary permeability.
l
Generalized edema may be a feature of
pre-eclampsia so remember to check
blood pressure & urine for protein. .
Severe edema may indicate cardiac
impairment or nephrotic
syndrome.