
Cause
unknown, but may be mediated immunologically.
There may be a genetic susceptibility to idiopathic
lichen planus
Rarely, familial.
Lichen planus is also associated with autoimmune
disorders, such as alopecia areata, vitiligo and
ulcerative colitis
Contact allergy to mercury compounds (in dental
amalgam fillings) seems to be an important cause of
oral lichen planus
Drugs
Some patients have a hepatitis C infection.
Presentation
Skin lesions
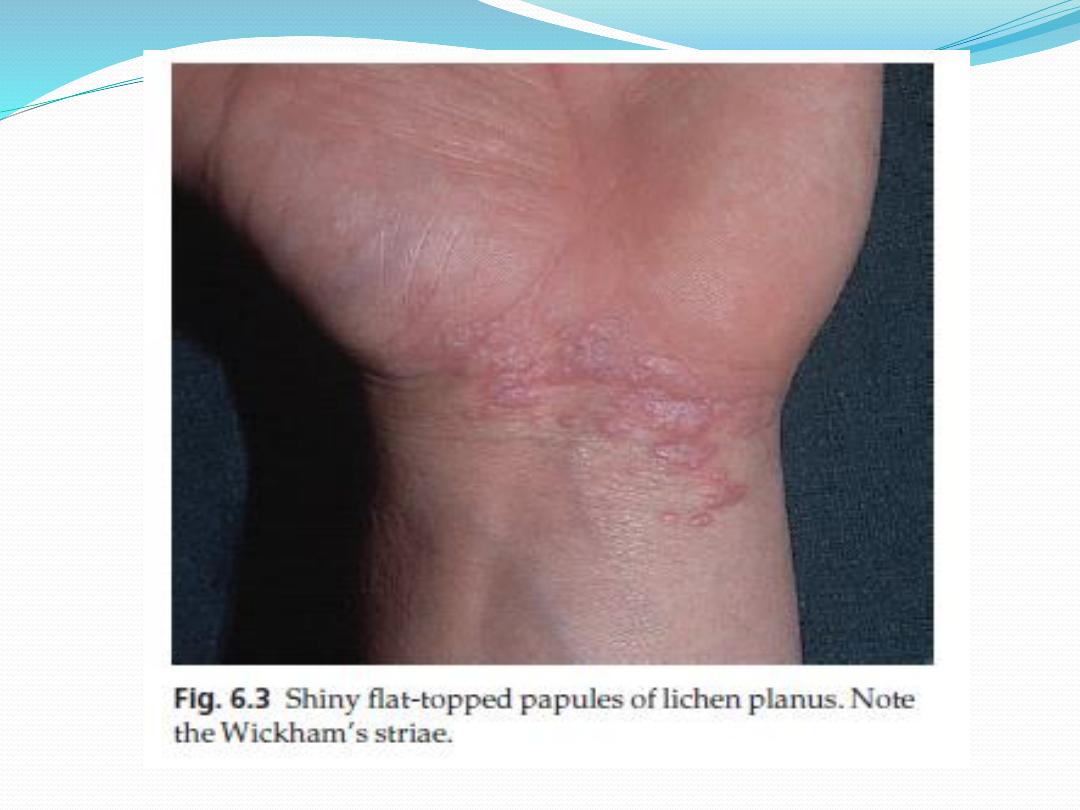
Typical lesions are violaceous or lilac-coloured, intensely itchy, flat-
topped papules that usually arise on the extremities, particularly on the
volar aspects of the wrists and legs
A close look is needed to see a white streaky pattern on the surface of
these papules (Wickham’s striae).
patients rub rather than scratch, so that excoriations are uncommon.
Köbner phenomenon may occur
Variants of lichen planus.
Annular
Atrophic
Bullous
Follicular
Hypertrophic
Presentation
Oral and genital skin lesions
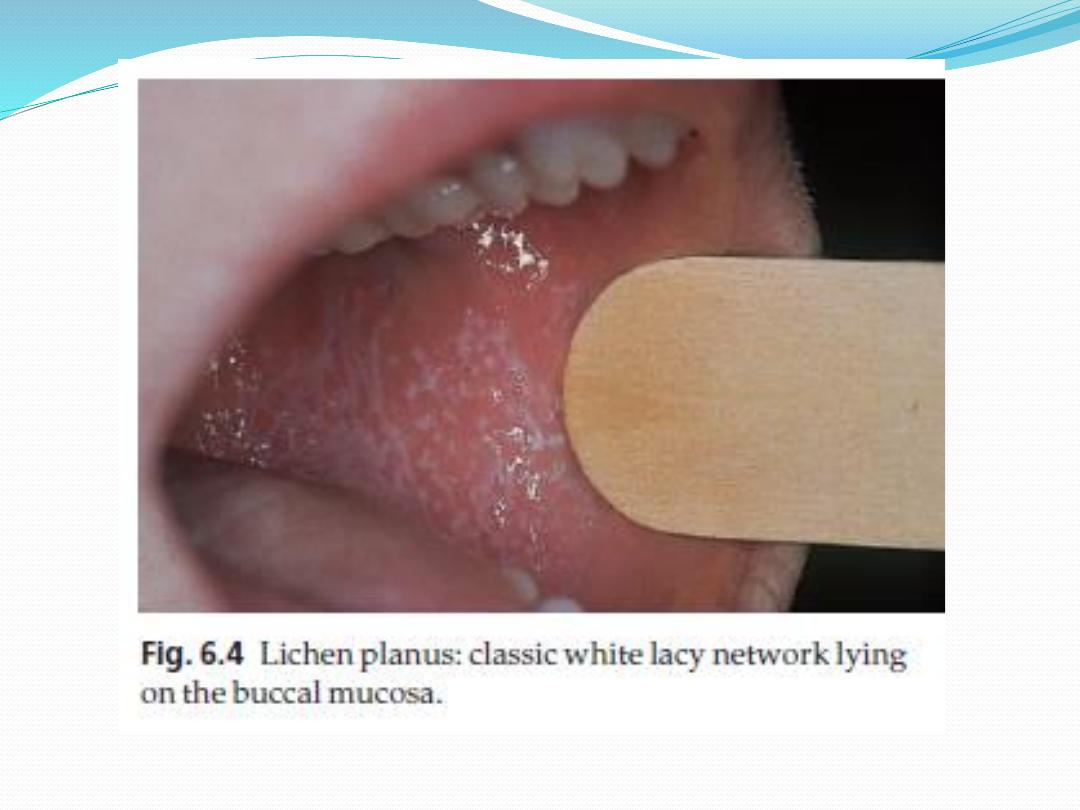
White asymptomatic lacy lines, dots, and occasionally
small white plaques, are also found in the mouth,
particularly inside the cheeks, in about 50% of patients and
oral lesions may be the sole manifestation of the disease.
Nail
The nails are usually normal, but in about 10% of patients
show changes ranging from fine
longitudinal grooves to destruction of the entire nail fold
and bed
Scalp
lesions can cause a patchy scarring alopecia.



Course
Individual lesions may last for many months and the eruption as
a whole tends to last about 1 year.
the hypertrophic variant often lasts for many years.
As lesions resolve, they become darker, flatter and leave discrete
brown or grey macules.
About one in six patients will have a recurrence.
Complications
Nail and hair loss can be permanent
The ulcerative form of lichen planus in the mouth may lead to
squamous cell carcinoma.
Ulceration, usually over bony prominences, may be disabling,
especially if it is on the soles
Differential diagnosis
Lichenoid drug reactions
can mimic lichen planus closely.
Gold and other heavy metals, antimalarials, beta-blockers, non-
steroidal anti-inflammatory drugs, para-aminobenzoic acid,
thiazide diuretics and penicillamine.
Contact with chemicals
used to develop colour photographic film can also produce
similar lesions.
Generalized discoid lupus erythematosus
it may be hard to differentiate from lichen planus
Wickham’s striae or oral lesions favour the diagnosis of lichen
planus.
Oral candidiasis
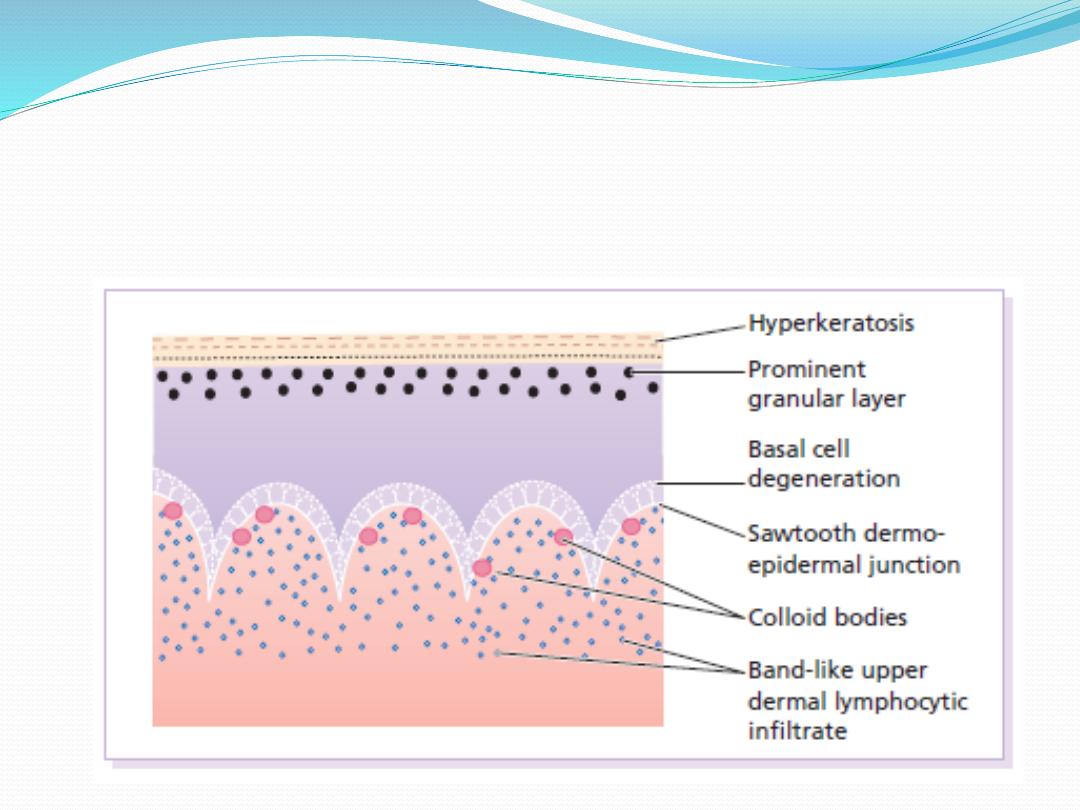
Investigations
histology is characteristic

Treatment
If drugs are suspected as the cause, they should be stopped
and unrelated ones substituted.
Potent topical steroids.
Systemic steroid are recommended in special situations
(e.g. unusually extensive involvement, nail destruction or
painful and erosive oral lichen planus).
PUVA or narrowband UVB
Oral ciclosporin or acitretin with stubborn lichen planus.
Antihistamines may blunt the itch.
Mucous membrane lesions, both oral and genital need no
treatment or use corticosteroid or calcineurin inhibitor.
Pityriasis rosea is a mild inflammatory exanthem
characterized by salmon-colored papular and macular
lesions that are at first discrete but may become
confluent.

Cause
may be caused by reactivation of either human herpes
virus 7 or human herpes virus 6.
The disease may occur in clusters, both geographical
and temporal, and seems not to be contagious.

Presentation
Pityriasis rosea is common, particularly during the winter.
It mainly affects children and young adults, and second
attacks are rare.
Most patients develop one plaque (the ‘herald’ or ‘mother’
plaque) before the others: It is larger (2–5 cm diameter)
than later lesions, and is rounder, redder and more scaly.
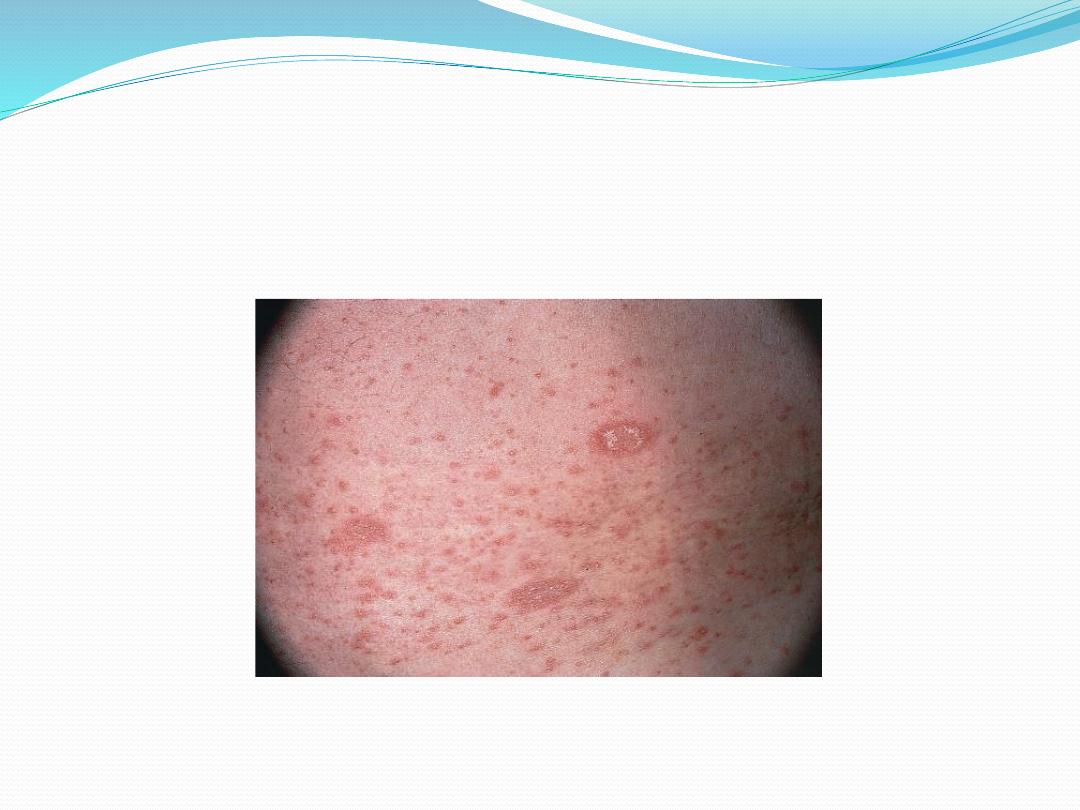
After several days many smaller plaques appear, mainly on
the trunk, but some also on the neck and extremities.
About half of patients complain of itching. An individual
plaque is oval, salmon pink and shows a delicate scaling,
adherent peripherally as a collarette.
Their longitudinal axes run down and out from the spine in
a ‘fir tree’ pattern, along the lines of the ribs.
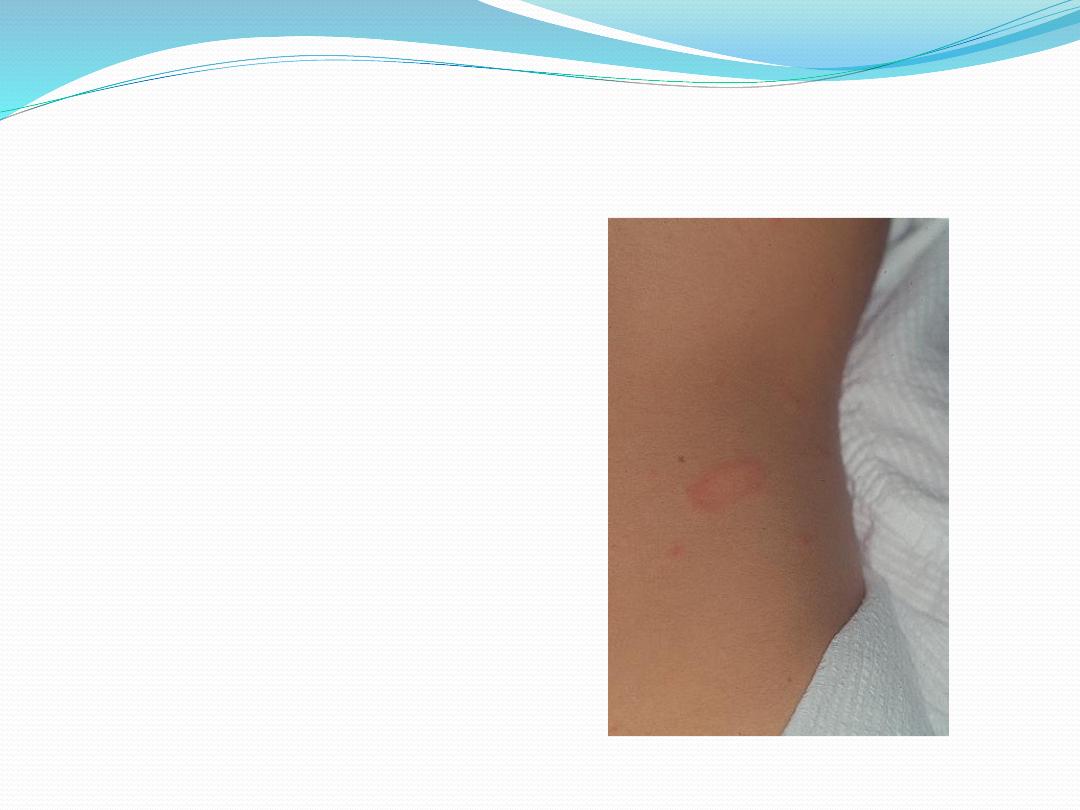
The herald plaque of pityriasis rosea is usually on the
trunk and is larger than the other lesions. Its annular
configuration is shown well here.
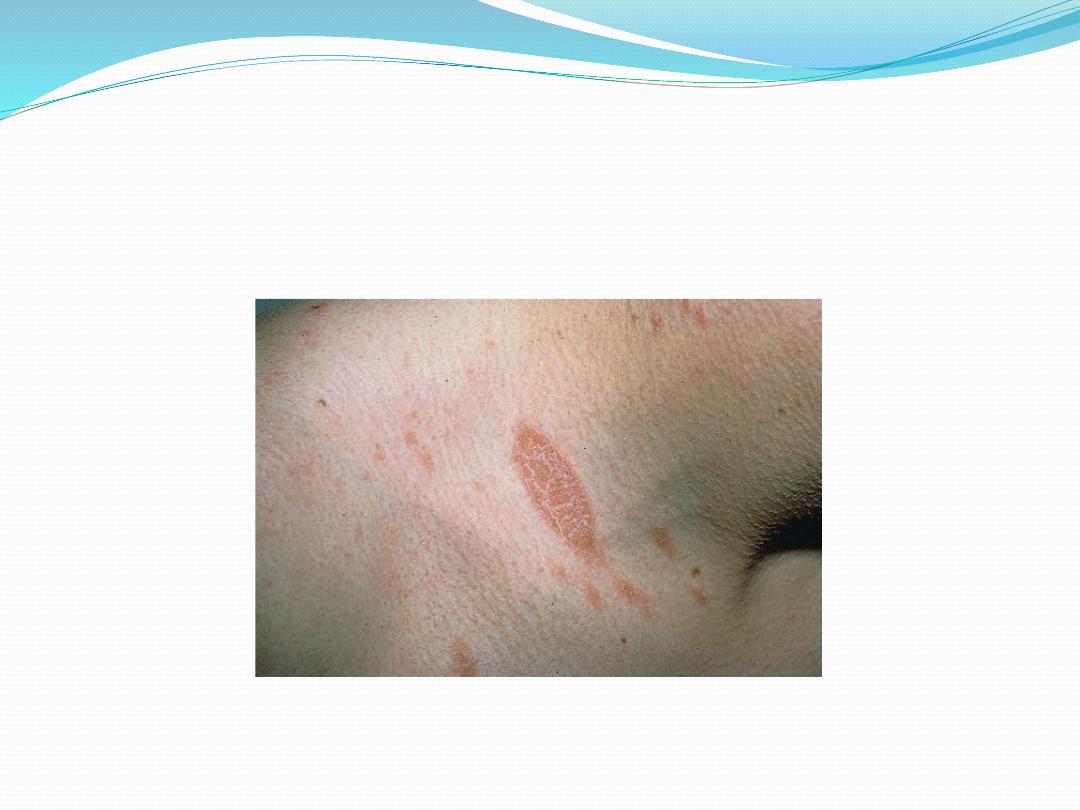
Herald patch of pityriasis rosea

Extensive pityriasis rosea showing
a ‘fir tree’ distribution on the back.
Pityriasis rosea

Course
The herald plaque precedes the generalized eruption
by several days.
Subsequent lesions enlarge over the first week or two.
A minority of patients have systemic symptoms such
as aching and tiredness.
The eruption lasts 2–10 weeks and then resolves
spontaneously, sometimes leaving hyperpigmented
patches that fade more slowly.

Differential diagnosis
Although herald plaques are often mistaken for ringworm
(tinea corporis), the two disorders most likely to be
misdiagnosed early in the general eruption are guttate
psoriasis and secondary syphilis.
Tinea corporis and pityriasis versicolor can be
distinguished by the microscopical examination of scales,
secondary syphilis by its other features (mouth lesions,
palmar lesions, condylomata lata, lymphadenopathy,
alopecia) and by serology.
Gold and captopril are the drugs most likely to cause a
pityriasis rosea-like drug reaction, but barbiturates,
penicillamine, some antibiotics and other drugs can also do
so.

Treatment
No treatment is curative, and active treatment is
seldom needed.
A moderately potent topical steroid or calamine lotion
will help the itching.
One per cent salicylic acid in soft white paraffin or
emulsifying ointment reduces scaling.
Sunlight or artificial UVB often relieves pruritus and
may hasten resolution.
So far, treatment with antiviral agents has not been
helpful.