Fungal infections
Dermatophyte infections (ringworm)
Cause
• Three genera of dermatophyte fungi cause tinea infections
(ringworm).
1.
Trichophyton – skin, hair and nail infections.
2.
Microsporum – skin and hair.
3.
Epidermophyton – skin and nails.
• Dermatophytes invade only into the stratum corneum, and the
inflammation they cause is a result of metabolic products of the
fungus or delayed hypersensitivity.
• Zoophilic fungi (those transmitted to humans by animals) cause a
more severe inflammation
• Anthropophilic fungi (spread from person to person) cause less
inflammation
Presentation and course
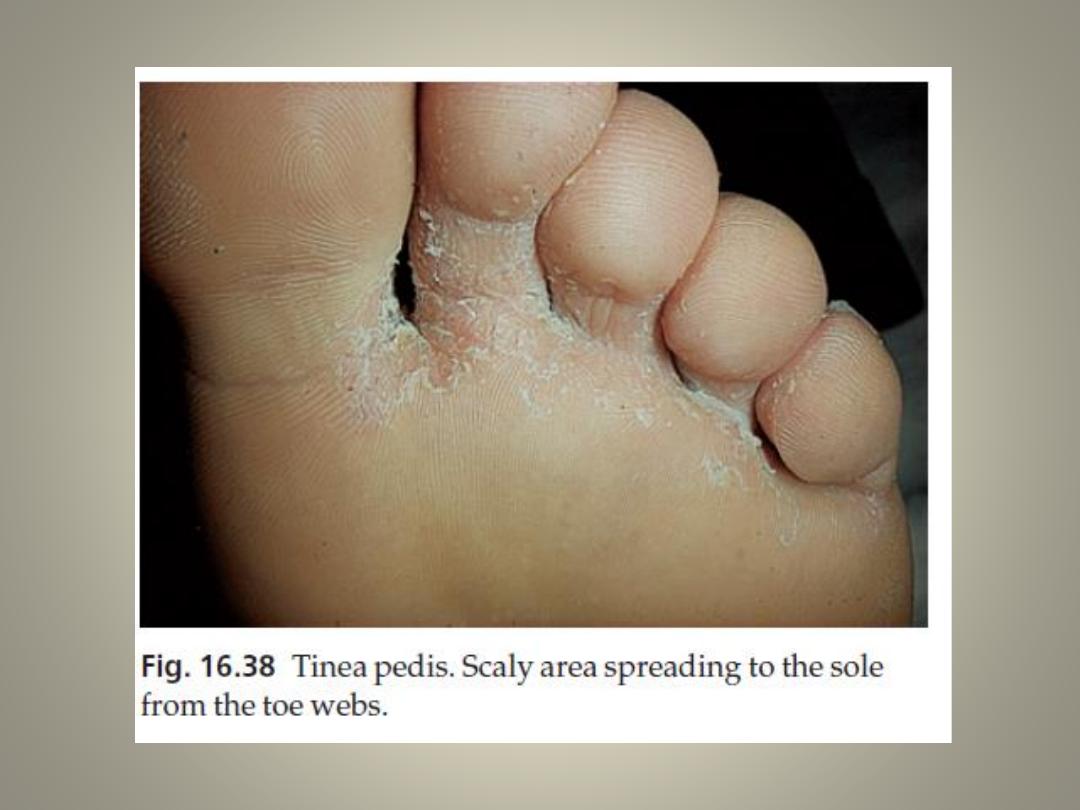
Tinea pedis (athlete’s foot)
• This is the most common type of fungal infection
• The sharing of wash places (e.g. in showers) and of swimming pools
predisposes to infection
• Most cases are caused by one of three organisms:
1.
Trichophyton rubrum (the most common and the most stubborn)
2.
Trichophyton mentagrophytes var. interdigitale
3.
Epidermophyton floccosum.
There are three common clinical patterns.
1. Soggy interdigital scaling, particularly in the fourth and fifth
interspace (all three organisms).
2. A diffuse dry scaling of the soles (usually T. rubrum).
3. Recurrent episodes of vesication (usually T. mentagrophytes var.
interdigitale or E. floccosum).

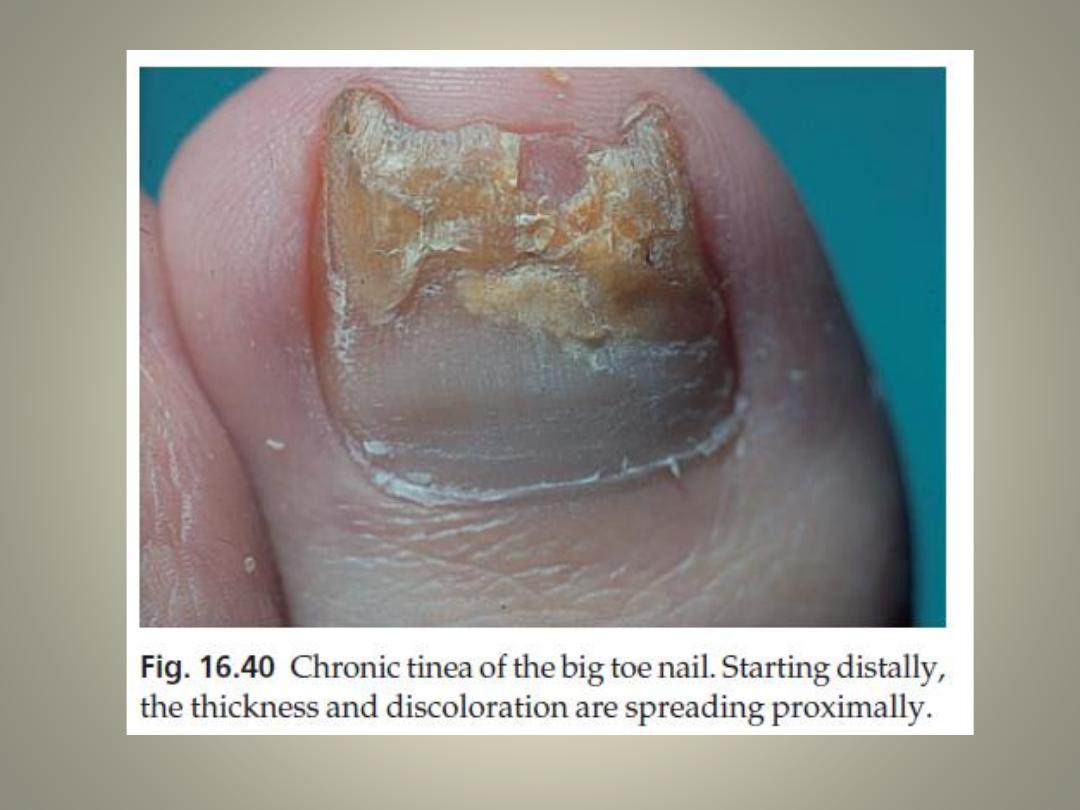
Tinea of the nails
• Toe nail infection is usually associated with tinea
pedis.
• The initial changes occur at the free edge of the
nail, which becomes yellow and crumbly
sometimes with subungual hyperkeratosis
• Usually, only a few nails are infected but rarely all.
• Finger nail lesions are similar, but less common,
and are seldom seen without a chronic T. rubrum
infection of the skin of the same hand.
Tinea of the hands
• This is usually asymmetrical and associated with tinea pedis
and unilateral onychomycosis.
• Trichophyton rubrum may cause a barely perceptible
erythema of one palm with a characteristic powdery scale
in the creases.
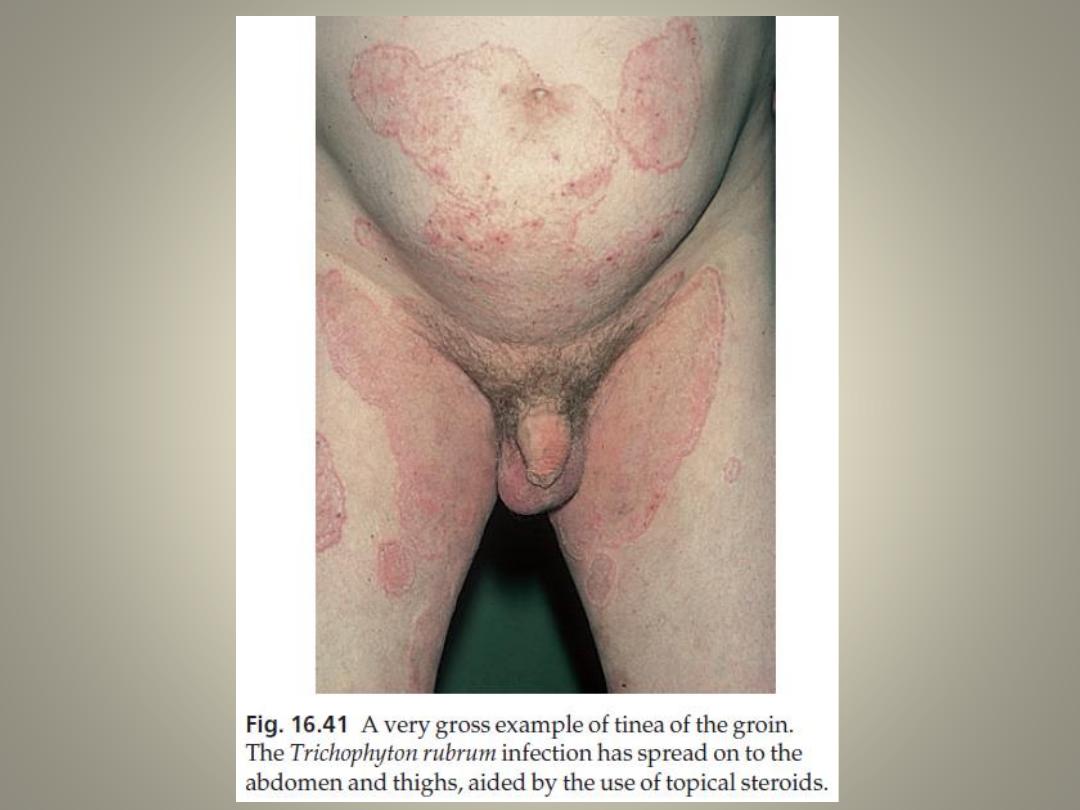
Tinea of the groin
• common and affects men more often than women.
• sometimes unilateral or asymmetrical
• The upper inner thigh is involved and lesions expand slowly
to form sharply demarcated plaques with peripheral scaling
• the scrotum is usually spared.
• A few vesicles or pustules may be seen within the lesions.
• The organisms are the same as those causing tinea pedis.
Tinea of the trunk and limbs
• characterized by plaques with scaling and
erythema most pronounced at the periphery.
A few small vesicles and pustules may be seen
within them.
• lesions expand slowly and healing in the
centre leaves a typical ring-like pattern
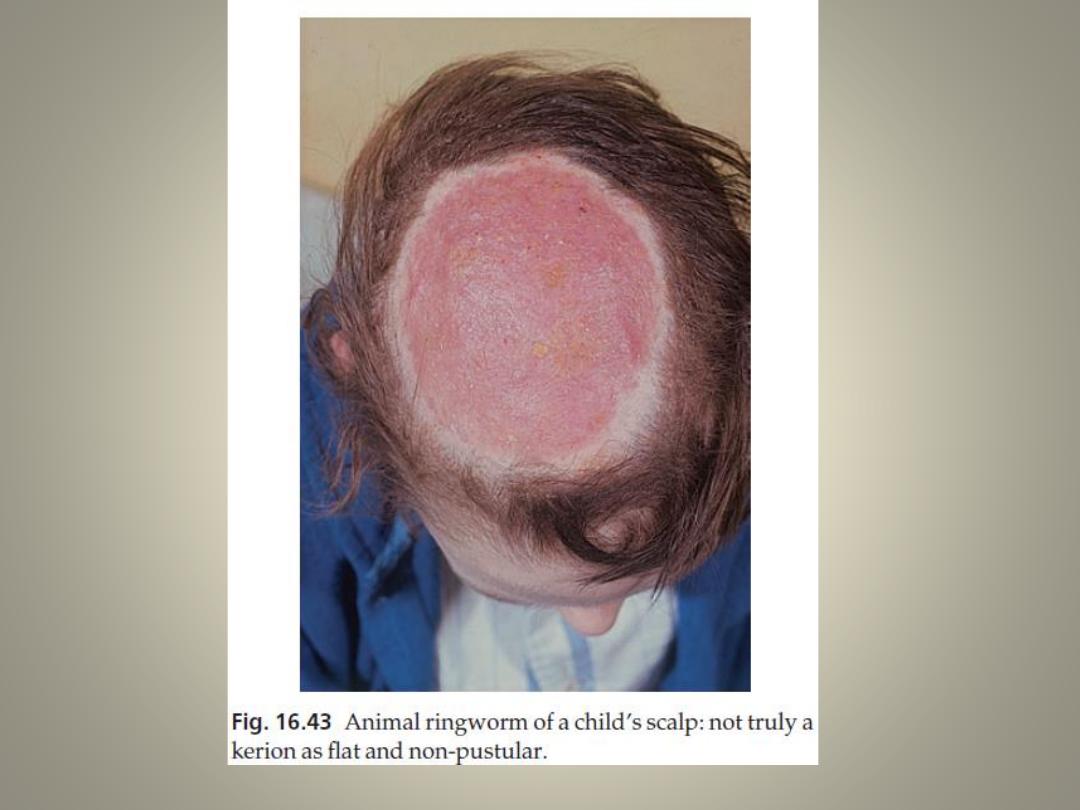
Tinea of the scalp (tinea capitis)
• usually a disease of children
• Fungi coming from human sources (anthropophilic
organisms) cause bald and scaly areas, with minimal
inflammation and hairs broken off 3–4 mm from the scalp.
• Fungi coming from animal sources (zoophilic fungi) induce
a more intense inflammation with boggy swelling,
pustulation and lymphadenopathy (kerion)
• The hair loss associated may be permanent
• Favus, caused by Trichophyton schoenleini, is foul-smelling
yellowish crusts surrounding many scalp hairs, and
sometimes leading to scarring alopecia.
• The scalp and hair of black children are especially prone to
infection with Trichophyton tonsurans
Complications
1. Fierce animal ringworm of the scalp can lead to a
permanent scarring alopecia.
2. A florid fungal infection anywhere can induce
vesication on the sides of the fingers and palms (a
trichophytid or ‘id reaction’).
3. Epidemics of ringworm occur in schools.
4. The usual appearance of a fungal infection can be
masked by mistreatment with topical steroids
(tinea incognito).

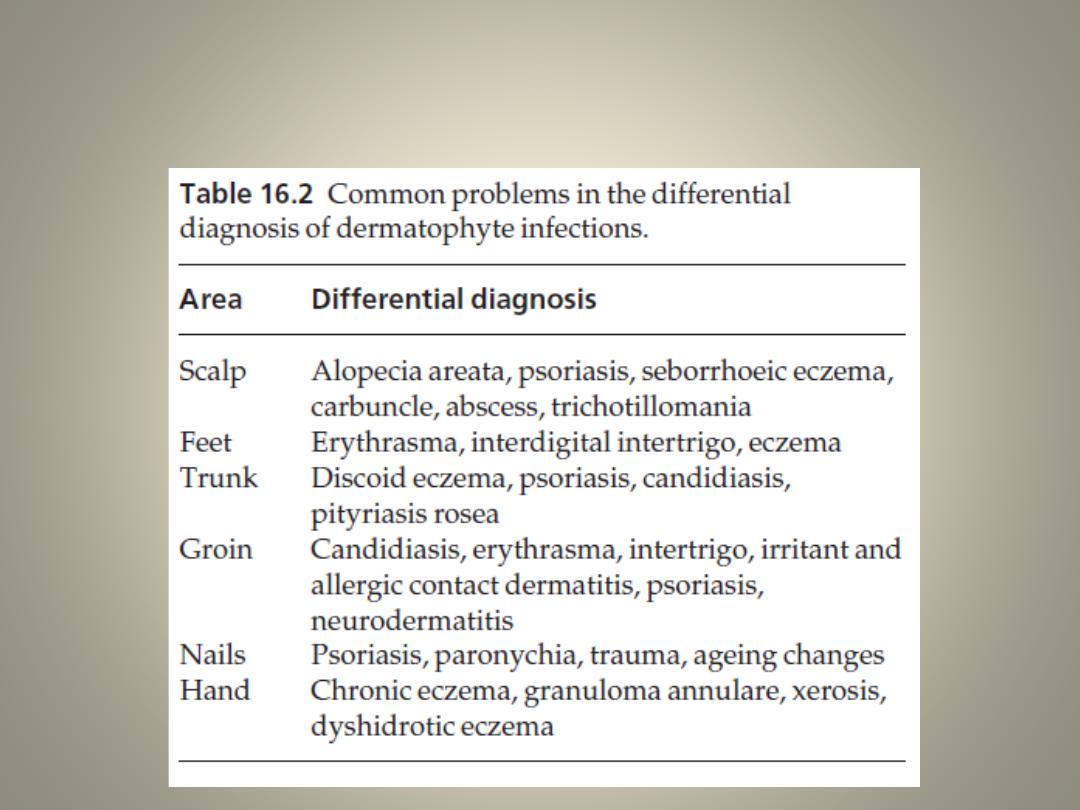
Differential diagnosis
Investigations
• Microscopic examination of a skin scraping, nail
clipping or plucked hair
• Cultures
• Wood’s light (ultraviolet light) examination of the scalp
usually reveals a green fluorescence of the hairs in
Microsporum audouini and M. canis infections, a
technique is useful for screening children in institutions
where outbreaks of tinea capitis still sometimes occur
• The most common fungus causing tinea capitis
(Trichophyton tonsurans) does not fluoresce.
Treatment
Local
• This is all that is needed for minor skin infections.
• imidazole preparations (e.g. miconazole and clotrimazole) and applied
twice daily.
• Magenta paint (Castellani’s paint), although highly coloured, is helpful for
exudative or macerated areas in body folds or toe webs.
• Occasional dusting with an antifungal powder is useful to prevent
relapses.
• Topical nail preparations such as nail lacquer containing amorolfine
ciclopirox can be used as adjuncts to systemic therapy
Systemic
Used in:
• scalp
• nails
• widespread
• chronic infections of the skin that have not responded to local measures
• Tinea incognito
Terbinafine
• It is fungicidal
• cures chronic dermatophyte infections more quickly
and more reliably than griseofulvin.
• For tinea capitis in children, a 4-week course of
terbinafine is as effective as an 8-week course of
griseofulvin.
• Cure rates of 70–90% can be expected for infected
finger nails after a 6-week course of terbinafine, and
for infected toe nails after a 3-month course.
• It is not effective in pityriasis versicolor or Candida
infections.
Itraconazole
• is now preferred to ketoconazole, which occasionally
damages the liver, and is a reasonable alternative to
terbinafine if this is contraindicated.
• interferes with the cytochrome P-450 system, interfere
with the metabolism of other drugs
• It is effective in tinea corporis, cruris and pedis and also
in nail infections.
• Fungistatic
• Also useful in pityriasis versicolor and candidiasis
Griseofulvin
• largely reserved for the treatment of tinea
capitis.
• It has proved to be a safe drug
• treatment may have to be stopped because of
persistent headache, nausea, vomiting or skin
eruptions.
• should not be given in pregnancy or to
patients with liver failure or porphyria.
Candidiasis
Cause
• Candida albicans is a classic opportunistic pathogen.
Predisposing factors
• obesity
• moisture and maceration
• immobility
• diabetes
• pregnancy
• the use of broad-spectrum antibiotics
• the use of the contraceptive pill
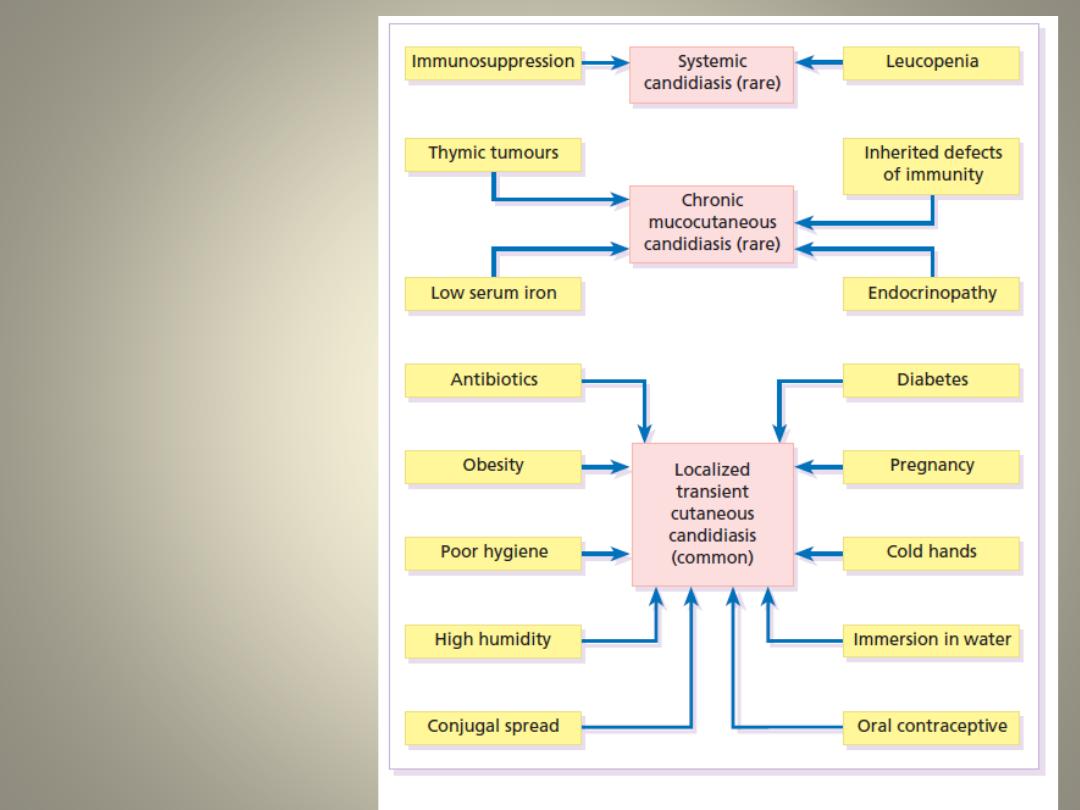
Factors predisposing
to
the different types
of candidiasis
Presentation
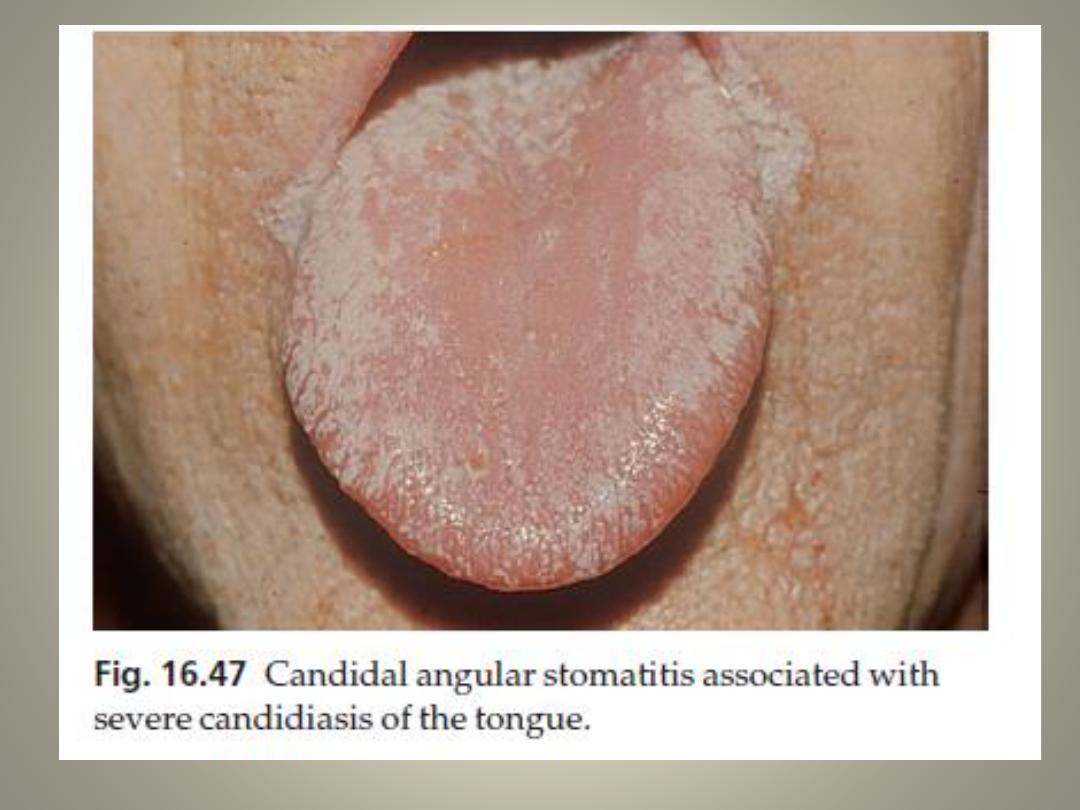
Oral candidiasis
• One or more whitish adherent plaques (like bread sauce)
appear on the mucous membranes, if wiped off they leave
an erythematous base.
Angular stomatitis
• usually in denture wearers may be candidal.
Candida intertrigo
• A moist glazed area of erythema and maceration appears in
a body fold; the edge shows soggy scaling, and outlying
satellite papulopustules.
• These changes are most common under the breasts, and in
the armpits and groin, but can also occur between the
fingers of those whose hands are often in water.
Genital candidiasis
• Most commonly presents as a sore itchy vulvovaginitis, with
white curdy plaques adherent to the inflamed mucous
membranes and a whitish discharge.
• The eruption may extend to the groin folds.
• Diabetes, pregnancy and antibiotic therapy are common
predisposing factors.
Paronychia
• Acute paronychia is usually bacterial, but in chronic
paronychia Candida may be the sole pathogen, or be found
with other opportunists such as Proteus or Pseudomonas
sp.
• Predisposing factors include wet work, poor peripheral
circulation and vulval candidiasis.
Treatment
• Predisposing factors should be sought and eliminated
• Infected skin folds should be separated and kept dry.
• Those with chronic paronychia should keep their hands warm and
dry.
• Amphotericin, nystatin and the imidazole group of compounds are
all effective topically.
• For the mouth, these are available as oral suspensions, lozenges
and oral gels
• For other areas of candidiasis use creams, ointment and pessaries
• In chronic paronychia, the nail folds can be packed with an
imidazole cream or drenched in an imidazole solution several times
a day.
• Genital candidiasis responds well to a single day’s treatment with
either itraconazole and fluconazole
Pityriasis versicolor
Cause
• caused by commensal yeasts Pityrosporum orbiculare
• Carboxylic acids released by the organisms inhibit the
increase in pigment production by melanocytes that occurs
normally after exposure to sunlight.
• The condition should be regarded as non-infectious.
Presentation and course
• The fawn or depigmented areas, with their slightly branny
scaling and fine wrinkling
• they are symptom-free or only slightly itchy.
• Lesions are most common on the upper trunk but can
become widespread.
• Recurrences are common.

Differential diagnosis
• vitiligo
• Seborrhoeic eczema
• Pityriasis alba
• Pityriasis rosea
• tinea corporis
• secondary syphilis
• leprosy
Investigations
• KOH of scrapings show a mixture of short branched hyphae and
spores (a ‘spaghetti and meatballs’ appearance).
• Culture is not helpful because the organism does not grow on
Sabouraud’s medium.
Treatment
• A topical preparation of one of the imidazole group of
antifungal drugs applied at night to all affected areas for 2–
4 weeks.
• Selsun shampoo is a 2.5% selenium sulphide mixture in a
detergent base, it should be lathered on to the patches
after an evening bath, and allowed to dry. Next morning it
should be washed off. Three applications at weekly
intervals are adequate.
• ketoconazole shampoo
• For widespread or stubborn infections, systemic
itraconazole (200 mg/day for 7 days), fluconazole or
ketoconazole may be curative
• Recurrence is common after any treatment
Thanks