ECZEMA
20% of all new patients referred to
clinics
Terminology
• The word ‘eczema’ comes from the Greek for
‘boiling’ – a reference to the tiny vesicles
(bubbles) that are often seen in the early
acute stages of the disorder
• ‘Dermatitis’ means inflammation of the skin
and is therefore, strictly speaking, a broader
term than eczema
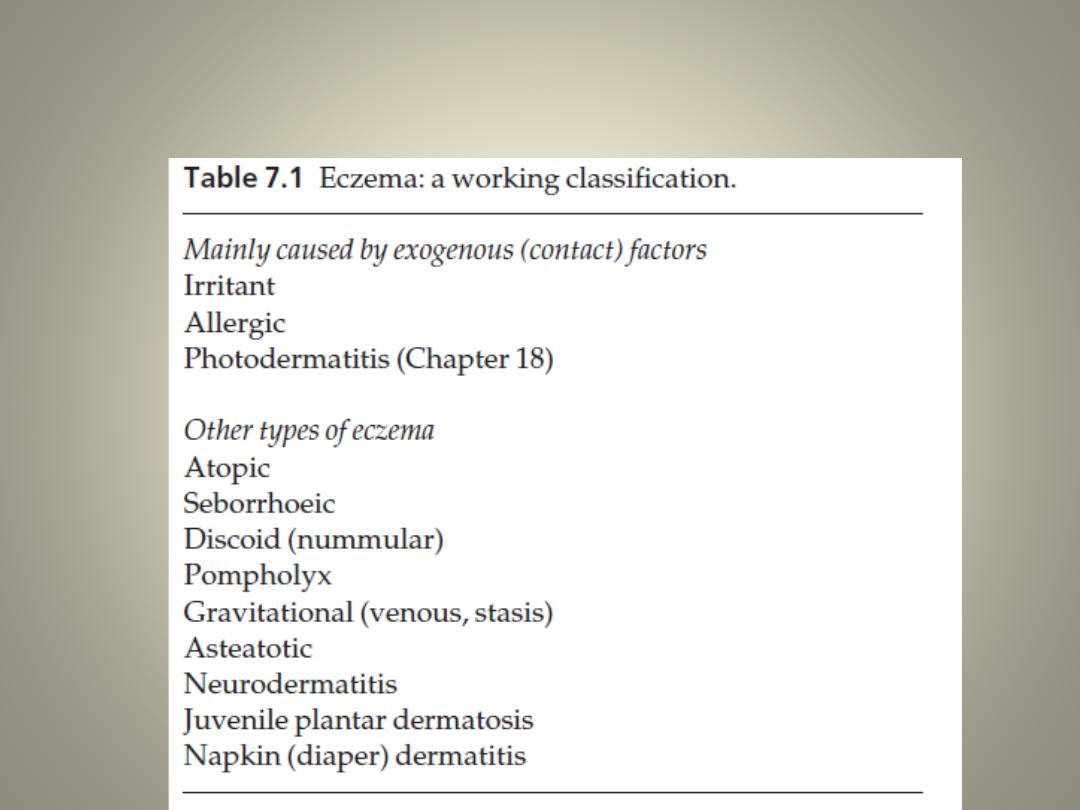
Classification
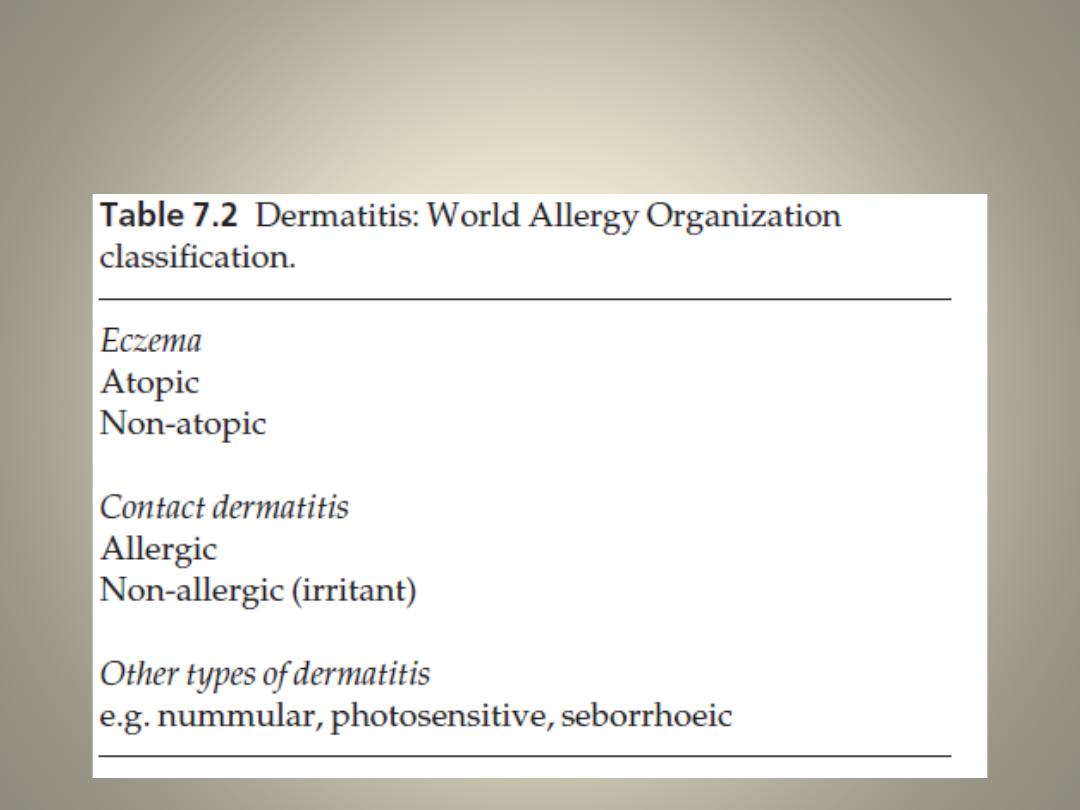
Classification
Histology
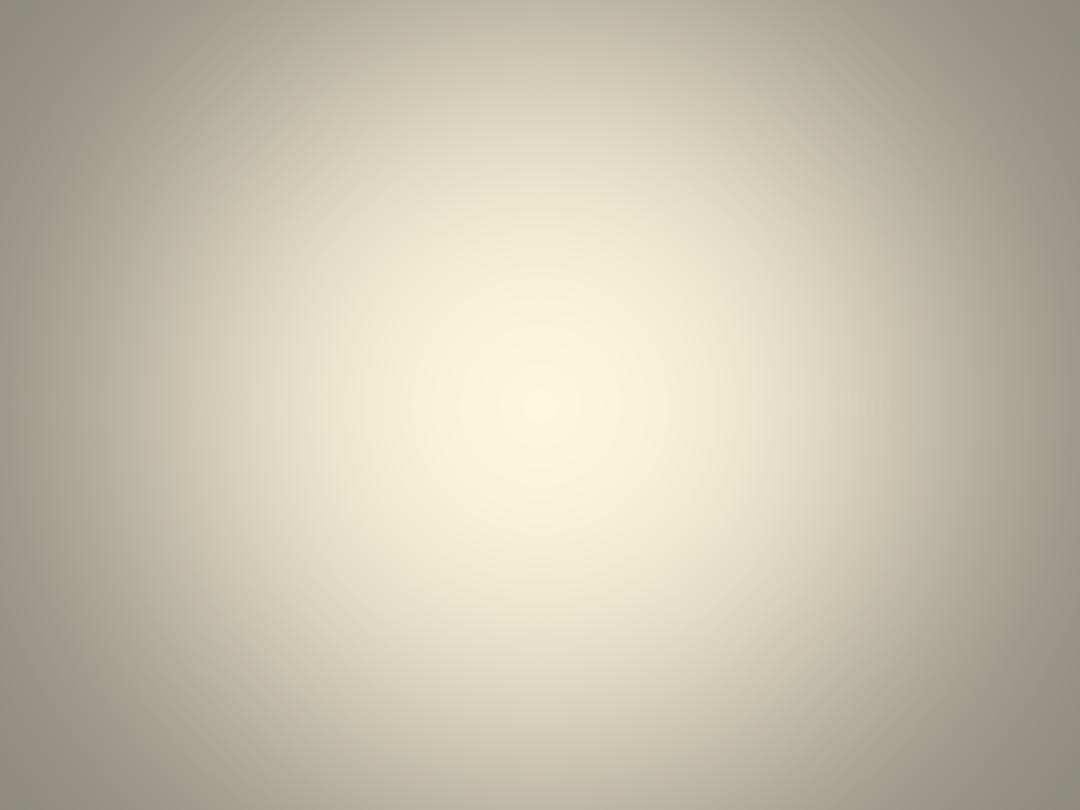
• In the acute stage, oedema in the epidermis
(spongiosis) progresses to the formation of intra-
epidermal vesicles, which may coalesce into
larger blisters or rupture.
• The chronic stages of eczema show less
spongiosis and vesication but more thickening of
the prickle cell layer (acanthosis) and horny layers
(hyperkeratosis and parakeratosis).
• variable degree of vasodilatation and infiltration
with lymphocytes
The sequence of
histological events
in eczema
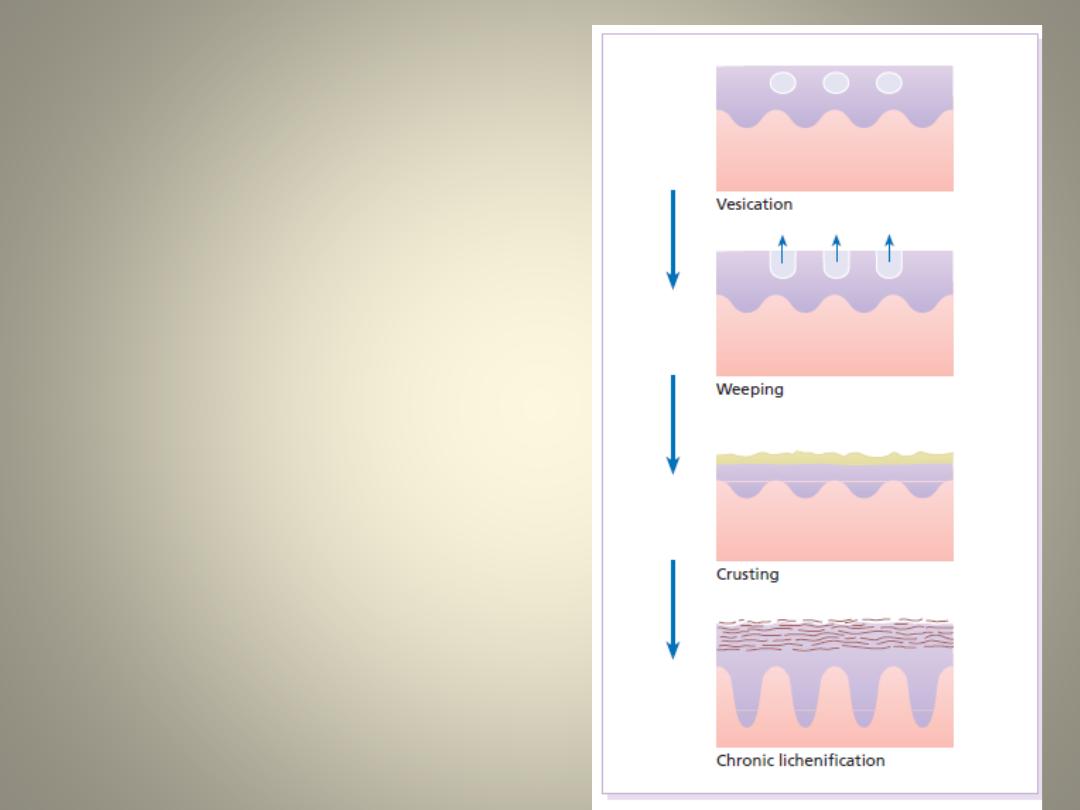
The causes of eczema
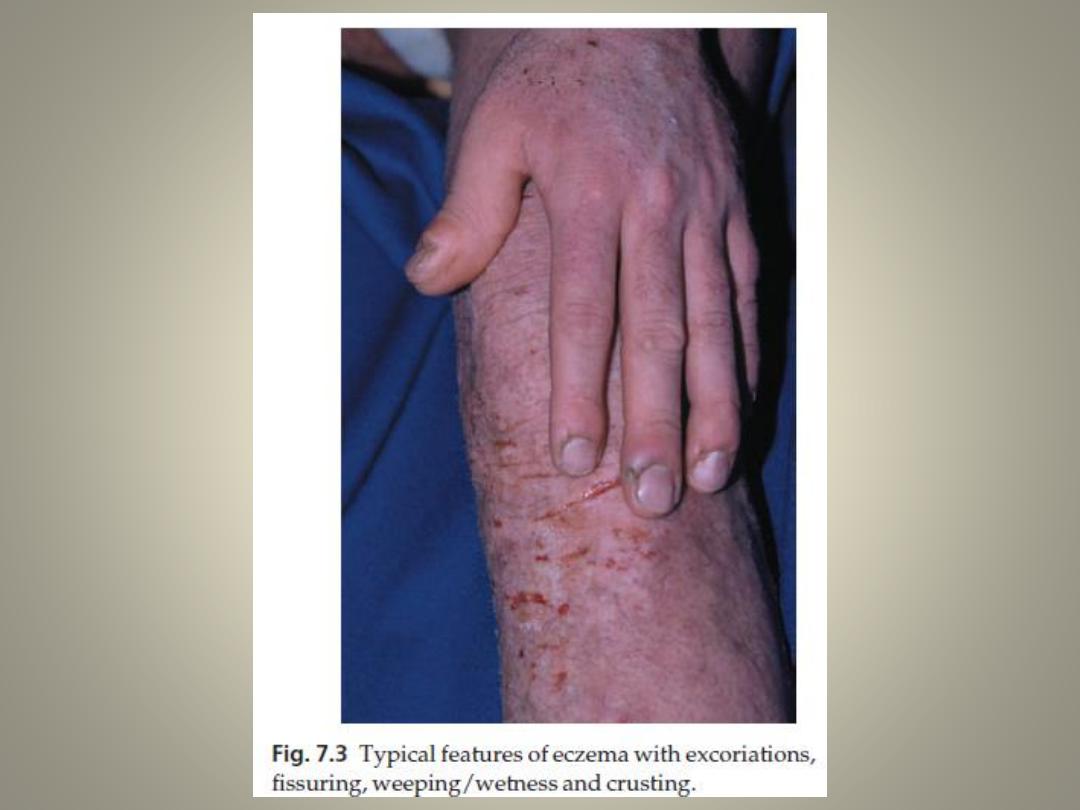
Clinical appearance
• The absence of a sharp margin is a particularly important feature that
separates eczema from most papulosquamous eruptions.
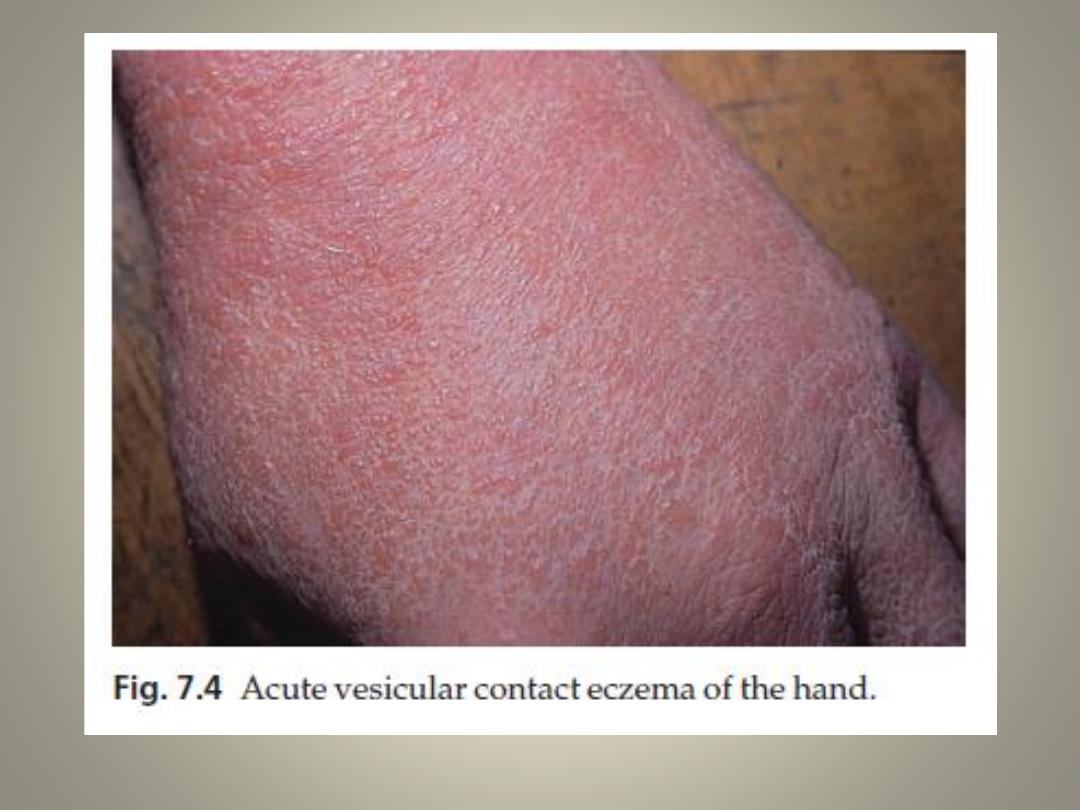
Acute eczema
Acute eczema is recognized by its:
• weeping and crusting
• blistering – usually with vesicles but, in fierce cases, with large blisters
• redness, papules and swelling
• ill-defined border and scaling
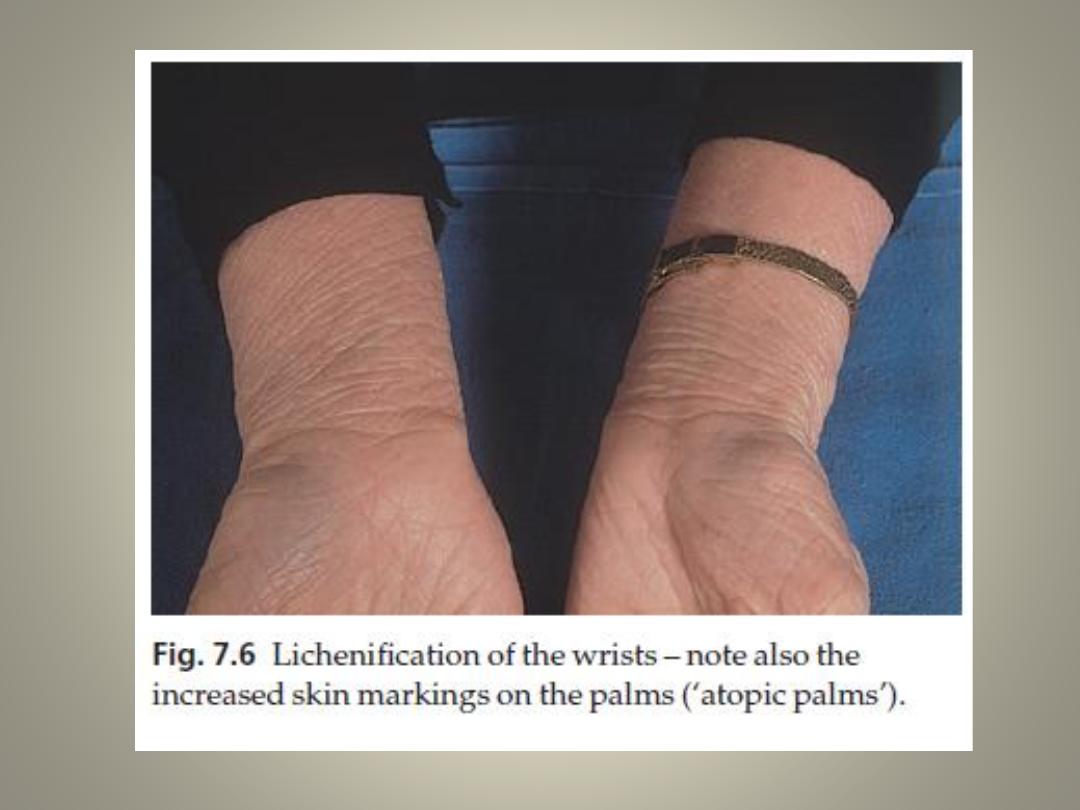
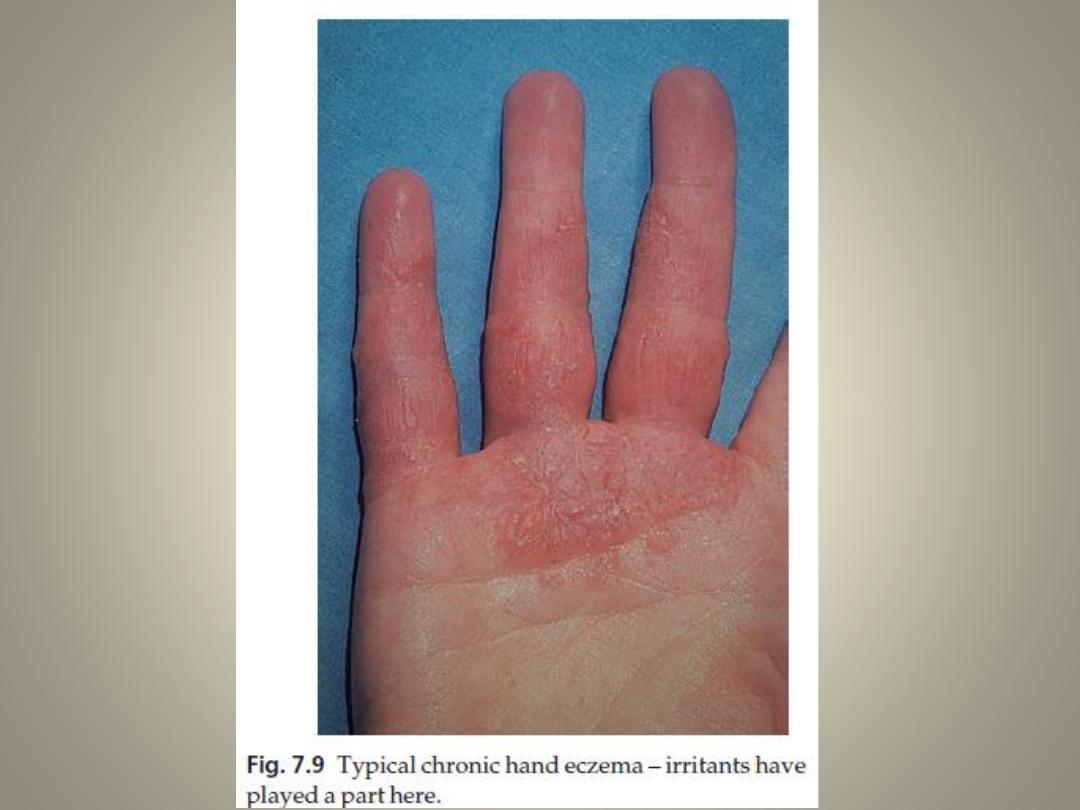
Chronic eczema
Chronic eczema may show all of the above changes but in general is:
• less vesicular and exudative
• more scaly, pigmented and thickened;
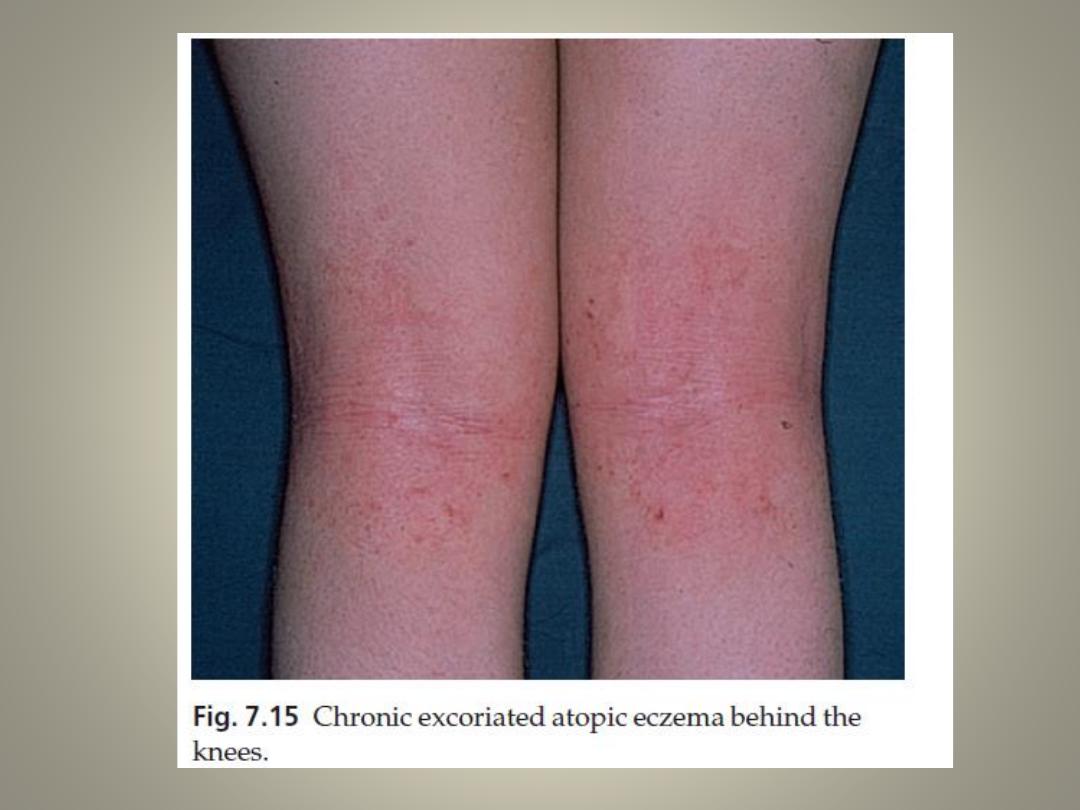
• more likely to show lichenification– a dry leathery thickened state, with
increased skin markings, secondary to repeated scratching or rubbing; and
more likely to fissure

Complications
1. Heavy bacterial colonization is common in all types of
eczema , overt infection is most troublesome in the
seborrhoeic, nummular and atopic types.
2. Local superimposed allergic reactions to medicaments
can provoke dissemination, especially in gravitational
eczema.
3. a huge effect on the quality of life.
4. An itchy sleepless child can wreck family life.
5. Eczema can interfere with work, sporting activities
and sex lives. Jobs can be lost through it
Differential diagnosis
• Papulosquamous dermatoses, such as psoriasis or lichen planus, are
sharply defined and show no signs of epidermal disruption
• Always remember that eczemas are scaly, with poorly defined margins.
• eczemas exhibit features of epidermal disruption such as weeping, crust,
excoriation, fissures and yellow scale (because of plasma coating the
scale).
• Once the diagnosis of eczema becomes solid, look for clinical pointers
towards an external cause. This determines both the need for
investigations and the best line of treatment.
• A contact element is likely if:
1.
there is obvious contact with known irritants or allergens
2.
the eruption clears when the patient goes on holiday, or at the weekend
3.
the eczema is asymmetrical, or has a linear or rectilinear configuration
4.
the rash picks out the eyelids, external ear canals, hands and feet, the
skin around stasis ulcers, or the perianal skin.
Investigations
Exogenous eczema
Patch testing
• to confirm allergic contact dermatitis and to identify the allergens
responsible for it
• In patch testing, standardized non-irritating concentrations of
common allergens are applied to the normal skin of the back. If the
patient is allergic to the allergen, eczema will develop at the site of
contact after 48–96 h.
• Patch testing with irritants is of no value in any type of eczema
Photopatch testing
• A chemical is applied to the skin for 24 h and then the site is
irradiated with a suberythemal dose of ultraviolet irradiation; the
patches are inspected for an eczematous reaction 48 h later.
Other types of eczema
• The only indication for patch testing here is when an
added contact allergic element is suspected. This is
most common in gravitational eczema
• Prick testing in atopic eczema
• Total and specific IgE antibodies are measured by a
radio-allergosorbent test RAST test as it carries no risk
of anaphylaxis, is easier to perform and is less time
consuming
• Cultures for bacteria and Candida if the eczema is
worsening despite treatment, or if there is much
crusting
Acute weeping eczema treatment
• rest and liquid applications
• Weeping eczema of the hands or feet is to use thrice daily
10-min soaks in a cool 0.65% aluminium acetate solution–
saline or even tap water will do almost as well
• each soaking being followed by a smear of a corticosteroid
cream or lotion and the application of a non-stick dressing
or cotton gloves
• One reason for dropping the dilute potassium
permanganate solution that was once so popular is
because it stains the skin and nails brown
• Wider areas on the trunk respond well to corticosteroid
creams and lotions or traditional remedies such as
calamine lotion, and the use of half-strength magenta paint
for the flexures are also effective
Wet wrap dressings
• This is a labour-intensive but highly effective
technique, of value in the treatment of troublesome
atopic eczema in children.
• After a bath, a corticosteroid is applied to the skin and
then covered with two layers of tubular dressing – the
inner layer already soaked in warm water, the outer
layer being applied dry and the dressings can then be
left in place for several hours
• The evaporation of fluid from the bandages cools the
skin and provides rapid relief of itching
Subacute eczema treatment
• Steroid lotions or creams are the mainstay of
treatment
• bacitracin, fusidic acid,mupirocin or neomycin
can be incorporated into the application if an
infective element is present, but watch out for
sensitization to neomycin, especially when
treating gravitational eczema
Chronic eczema treatment
• Steroids in an ointment base, cause best responds, but is also often
helped by non-steroid applications such as ichthammol and zinc cream or
paste
• The strength of the steroid is important
• Nothing stronger than 0.5 or 1% hydrocortisone ointment should be used
on the face or in infancy.
• In adults one should be reluctant to prescribe more than 200 g/week of a
mildly potent steroid, 50 g/week of a moderately potent or 30 g/week of a
potent one for long periods
• Calcineurin inhibitors such as tacrolimus and pimecrolimus work well,
although they lack the potency of strong topical corticosteroids.
• Systemic antibiotics for bacterial superinfection or incorporation of
antibiotics (e.g. fusidic acid, mupirocin, neomycin or chlortetracycline) or
antiseptics (e.g. Vioform) into the steroid formulation
• Salicylic acid (1–6% in emulsifying ointment) or stabilized urea
preparations for chronic localized hyperkeratotic eczema of the palms or
soles
Systemic treatment
• Short courses of systemic steroids may occasionally be
justified in extremely acute and severe eczema,
particularly when the cause is known and already
eliminated (e.g. allergic contact dermatitis). However,
prolonged systemic steroid treatment should be
avoided in chronic cases, particularly in atopic eczema.
• Antihistamines may help at night.
• Systemic antibiotics may be needed in widespread
bacterial superinfection. Staphylococcus aureus
routinely colonizes all weeping eczemas, and most dry
ones as well
Common patterns of eczema
Irritant contact dermatitis
• This accounts for more than 80% of all cases of contact
dermatitis, and for the vast majority of industrial cases
Cause
• Strong irritants elicit an acute reaction after brief
contact but prolonged exposure, sometimes over
years, is needed for weak irritants to cause dermatitis
• Detergents, alkalis, solvents, cutting oils and abrasive
dusts are common culprits.
• Past or present atopic dermatitis doubles the risk of
irritant hand eczema developing
Complications
• The condition may lead to loss of work.
Differential diagnosis
• It is often hard to differentiate irritant from allergic contact
dermatitis, and from atopic eczema of the hands
Investigations
• Patch testing with irritants is not helpful and may be misleading but
patch testing to a battery of common allergens help to detect
allergic element
Treatment
• based upon avoidance of the irritants
• reduced exposure by the use of protective gloves and clothing.
• Moderately potent topical corticosteroids and emollients are
valuable
• Prevention is better than cure because, once started, irritant
eczema can persist long after contact with offending substances has
ceased, despite the vigorous use of emollients and topical
corticosteroids
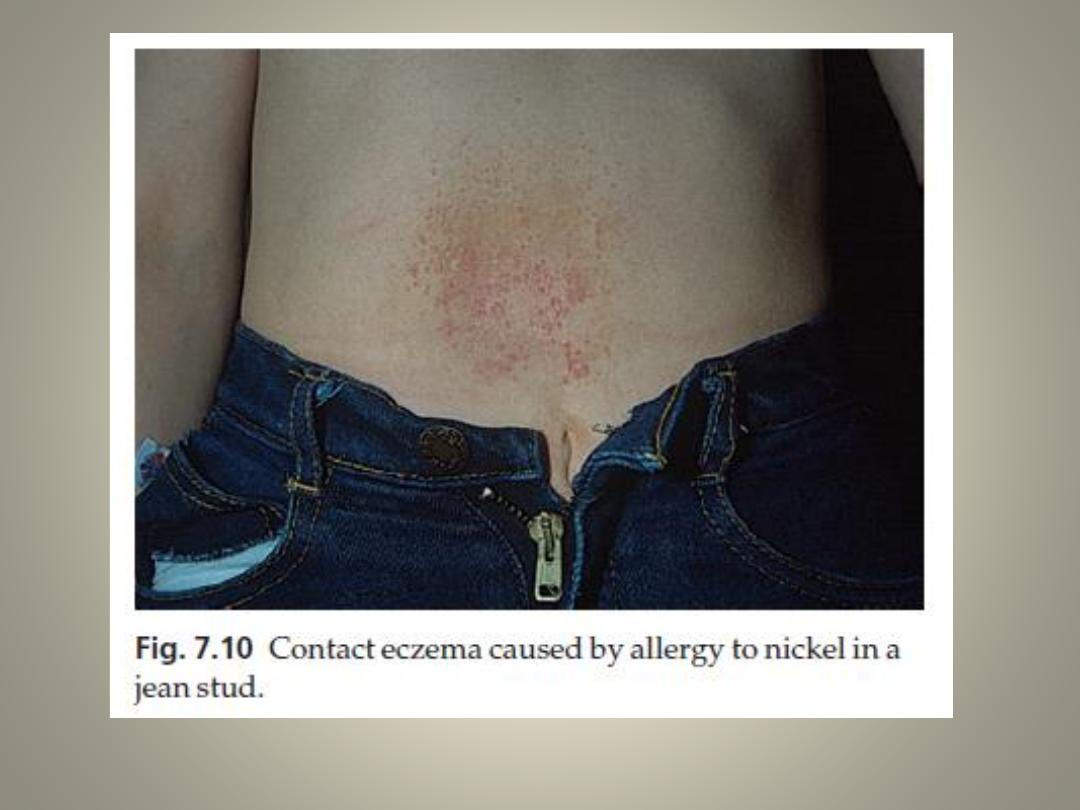
Allergic contact dermatitis
Cause
• The mechanism is that of delayed (type IV)
hypersensitivity,
It has the following features.
1. Previous contact is needed to induce allergy.
2. It is specific to one chemical and its close relatives.
3. After allergy has been established, all areas of skin
will react to the allergen.
4. Sensitization persists indefinitely.
5. Desensitization is seldom possible
Allergens
• Are variable
• Their ability to sensitize varies – from substances that can
do so after a single exposure (e.g. poison ivy) to those that
need prolonged exposure (e.g. chrome – bricklayers take an
average of 10 years to become allergic to it).
Presentation and clinical course
• Allergic contact dermatitis should be suspected if:
1. certain areas are involved (e.g. the eyelids, external
auditory meati, hands or feet, and around gravitational
ulcers)
2. there is known contact with the allergens mentioned
3. the individual’s work carries a high risk (e.g. hairdressing,
working in a flower shop, or dentistry)
Investigations
Patch testing
• Some allergies are more common than others, nickel top of the list,
with a positive reaction in some 15% of those tested; fragrance
allergy usually comes second.
• It is important to remember that positive reactions are not
necessarily relevant to the patient’s current skin problem; some are
simply ‘immunological scars’ left behind by previous unrelated
problems
Treatment
• avoidance of the relevant allergen is most important, Job changes
are sometimes needed
• Reducing exposure is usually not enough
• Topical corticosteroids give temporary relief

Occupational dermatitis
• Dermatitis is the second most common
occupational disorder – second only to
musculoskeletal injuries
• The hands are affected in 80–90% of cases.
Often several factors (constitutional, irritant
and allergic) have combined to cause this
Atopic eczema
Atopic eczema
• The word ‘atopy’ comes from the Greek (a-topos
meaning ‘without a place’).
• Atopy is a state in which an exuberant production
of IgE occurs as a response to common
environmental allergens.
• Atopic subjects may, or may not, develop one or
more of the atopic diseases such as asthma, hay
fever, eczema and food allergies
• Several environmental factors that reduce the risk
of developing atopic disease are: having many
older siblings, growing up on a farm, having
childhood measles and gut infections.
• The ‘hygiene hypothesis’ blaming the early use of
antibiotics and a reduced exposure to orofaecal and
other infections for preventing normal immunological
maturation and shifting the circulating T lymphocytes
of children destined to develop allergies from a Th1 to
a Th2 response.
• Perinatal administration of a Gram-positive probiotic
(Lactobacillus GG) to infants at risk of atopic disease
significantly reduces the incidence of eczema for up to
4 years. Unfortunately, no such benefit is seen
following administration to older children or adults.
Inheritance
• A strong genetic component is obvious, although affected
children can be born to clinically normal parents.
• The concordance rates for atopic eczema in monozygotic
and dizygotic twins are around 80% and 22%, respectively
• Atopic diseases tend to run a specific type within each
family. In some, most of the affected members will have
eczema; in others, respiratory allergy will predominate.
• There is also a tendency for atopic diseases to be inherited
more often from the mother than the father, and if both
parents have atopic eczema, a child has a 75% chance of
developing the disease.
• Loss of function in the filaggrin gene causes ichthyosis
vulgaris but is also strongly predictive for atopic eczema.
Presentation and course
• It affects at least 3% of infants
Onset
• 75% of cases of atopic eczema begin before the
age of 6 months, and 80–90% before the age of 5
years.
• the onset may be delayed until childhood or adult
life.
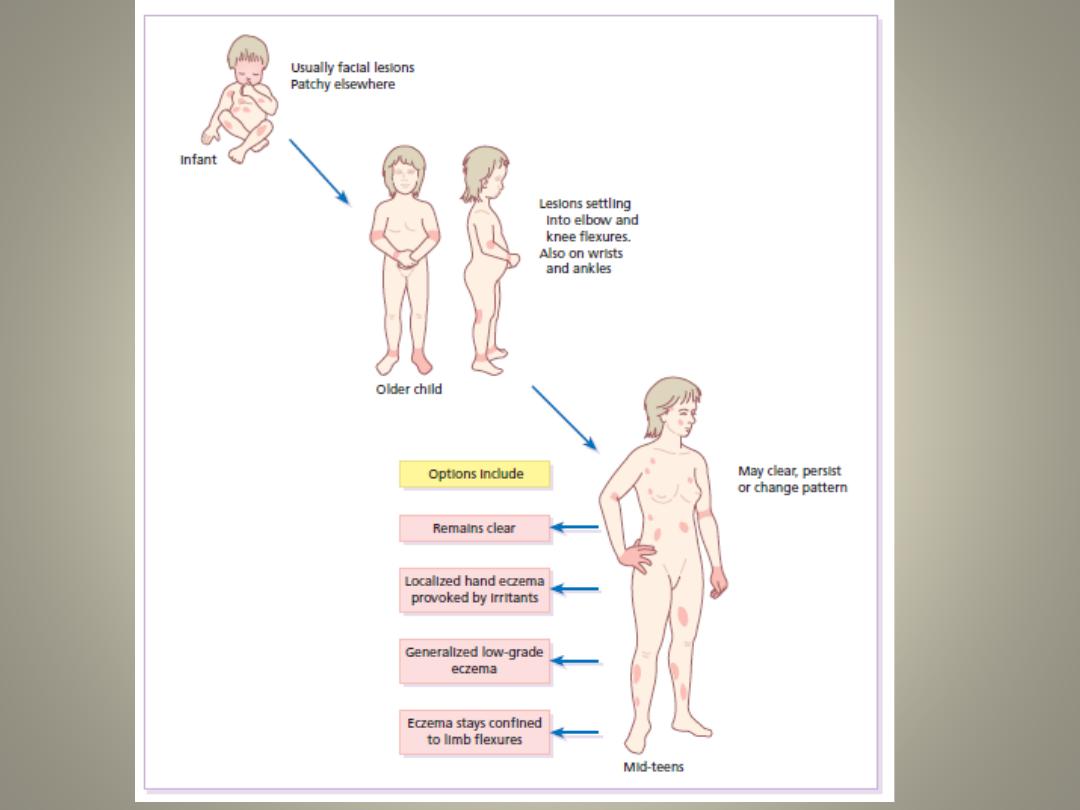
• Some 60–70% of children with atopic eczema will
clear by their early teens, although subsequent
relapses are possible.
Lesions
• The distribution and character of the lesions vary with age but a general
dryness of the skin may persist throughout life.
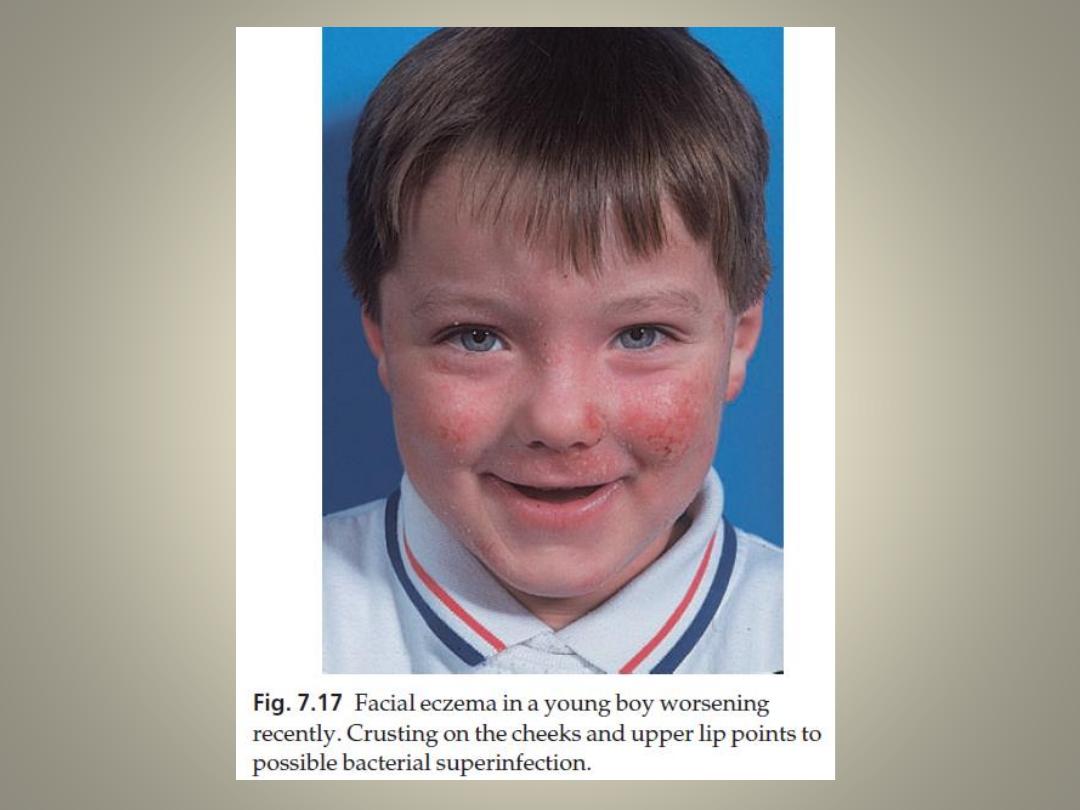
In infancy
• atopic eczema tends to be vesicular and weeping
• often starts on the face with a non-specific distribution elsewhere,
commonly sparing the napkin (diaper) area.
In childhood
• the eczema becomes leathery, dry and excoriated
• affecting mainly the elbow and knee flexures, wrists and ankles.
• A stubborn ‘reverse’ pattern affecting the extensor aspects of the limbs is
also recognized.
In adults
• the distribution is as in childhood with a marked tendency towards
lichenification and a more widespread but low-grade involvement of the
trunk, face and hands.
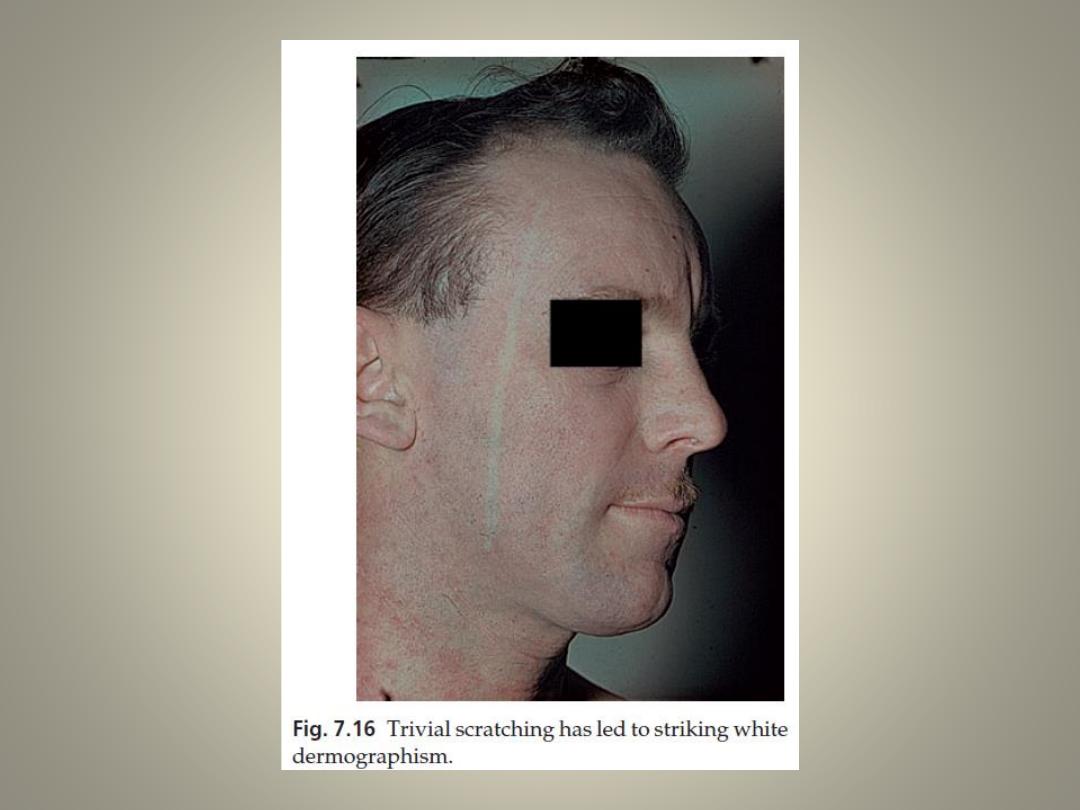
• White dermographism, is often striking, but not diagnostic of atopic
eczema.
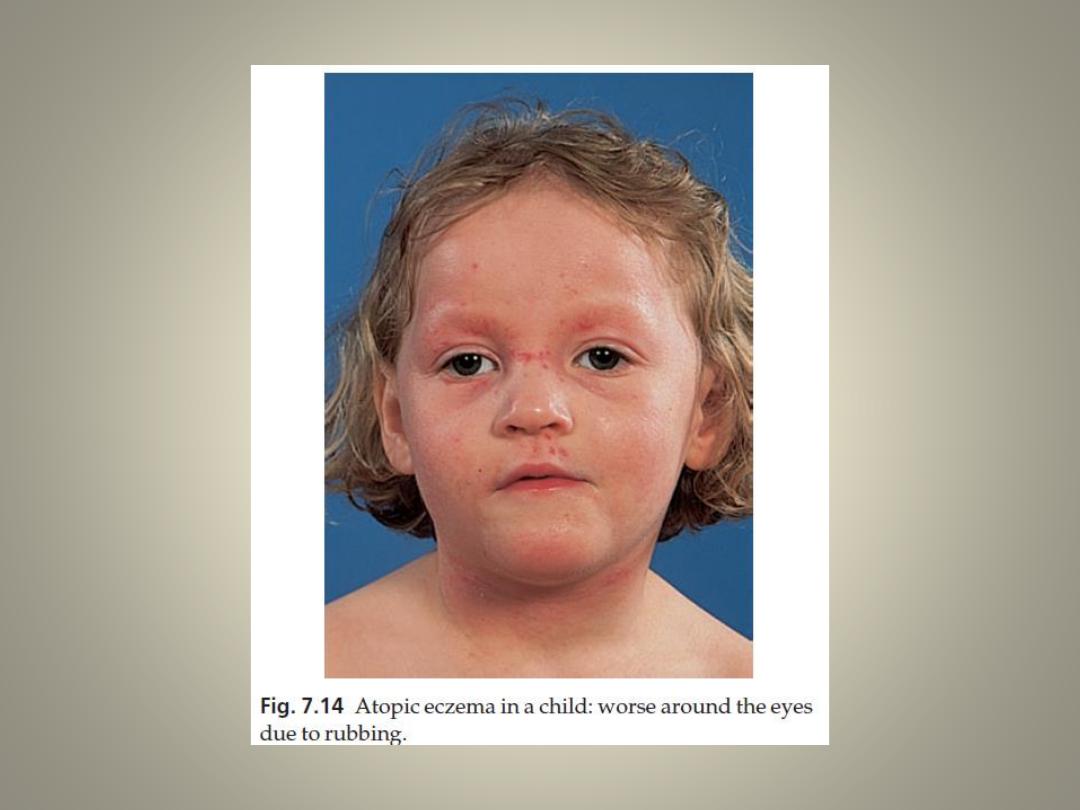
• The cardinal feature of atopic eczema is itching, and
scratching may account for most of the clinical picture.
• Affected children may sleep poorly, be hyperactive and
sometimes manipulative, using the state of their
eczema to get what they want from their parents.
• The condition remits spontaneously before the age of
10 years in at least two-thirds of affected children, but
it may come back at times of stress.
• Eczema and asthma may seesaw, so that while one
improves the other may get worse.
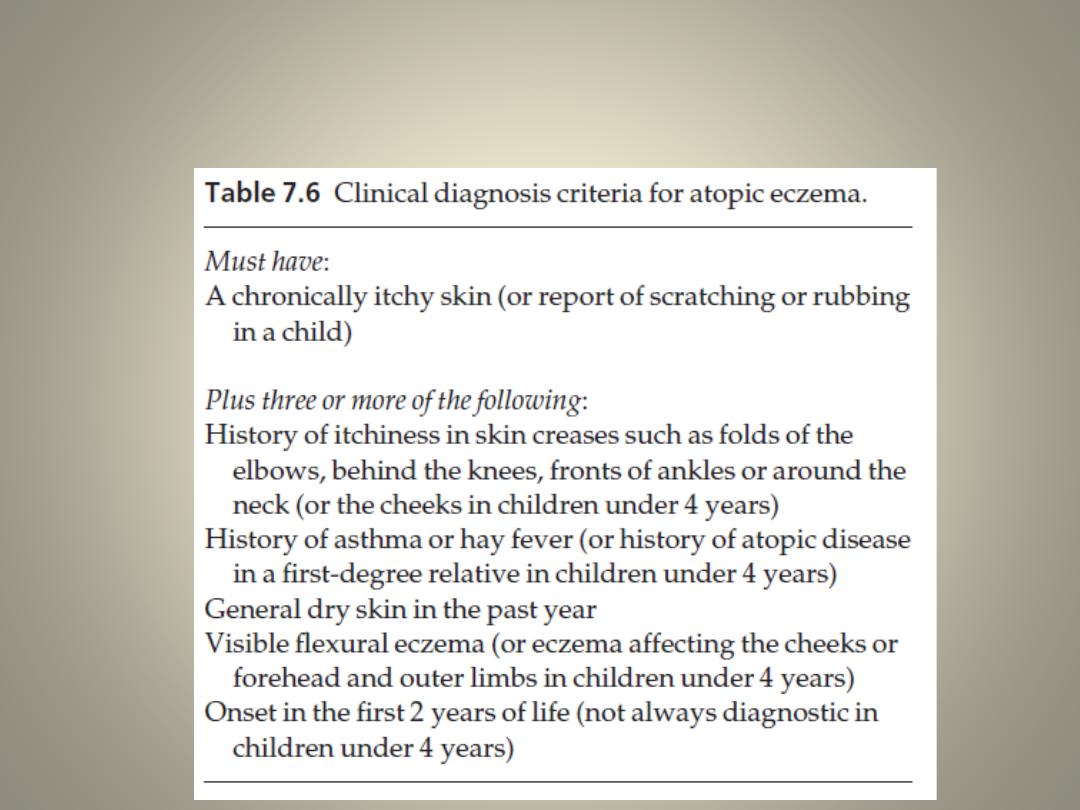
Diagnostic criteria
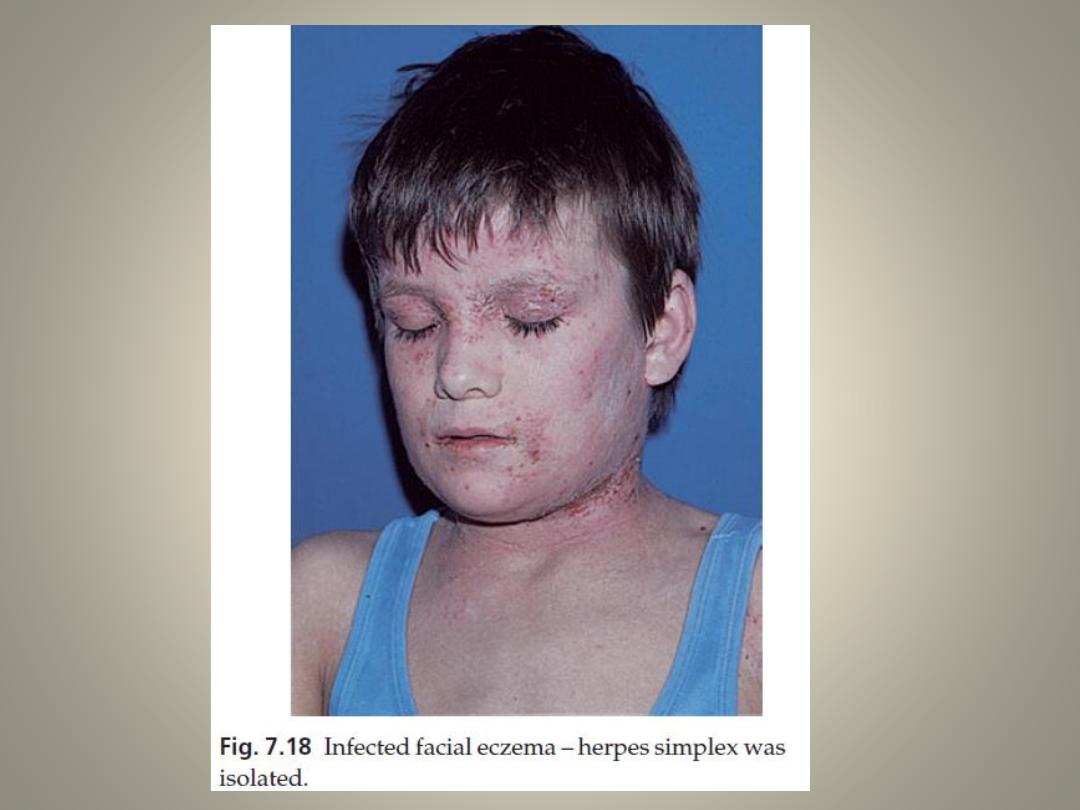
Complications
• Overt bacterial infection
• Viral infections, most dangerously with widespread
herpes simplex (eczema herpeticum), but also with
molluscum contagiosum and warts.
• Growth impairment because of impaired sleep due to
itching and absorption of topical steroids can
contribute
Investigations
• The value of prick testing in atopic eczema remains
controversial. Often the finding of multiple positive
reactions, and a high IgE level, does little more than
support a doubtful clinical diagnosis.
Treatment
• Explanation, reassurance and encouragement.
• Avoidance of exacerbating factors such as
irritants (e.g. woollen clothing next to the skin)
and avoid extremes of temperature, and contact
with soaps and detergents.
• Emollients used regularly. Those with an
associated ichthyosis should generally use
ointments rather than creams.
• Occlusive bandaging to cut the scratch–itch
cycle by (e.g. with a 1% ichthammol paste
bandage). Nails should be kept short.
Topical steroids.
• A technique useful for extensive and troublesome eczema,
particularly in children, is that of ‘wet wrap’ dressings
• Tacrolimus is an immunosuppressant, now available as an ointment
for topical use in eczema unresponsive to conventional therapy.
• The 0.1% ointment is equivalent in strength to a moderate or
potent topical corticosteroid but without the potential to cause skin
atrophy
• Best used for treatment of resistant eczema on sensitive sites, such
as the face, or in patients requiring constant use of topical steroids.
• Local infection might be troublesome and concerns remain about
the development of skin cancer or lymphoma in the long term.
• Patients should be advised to avoid excessive exposure to sunlight
or UV lamps while using tacrolimus.
Sedative antihistamines (e.g. trimeprazine or hydroxyzine)
• are of value if sleep is interrupted, but histamine release is not the
main cause of the itching, so the newer non-sedative
antihistamines help less than might be expected.
Antibiotics
• Acute flares are often induced by the surface proliferation of
staphylococci, even without frank sepsis. A month’s course of a
systemic antibiotic (e.g. erythromycin) may then be helpful.
Allergen avoidance
• as house dust mites, sometimes, but not always, measures to
reduce contact with these allergens help eczema. These measures
should include encasing the mattress in a dustproof bag, washing
the duvets and pillows every 3 months at a temperature greater
than 55°C, and thorough and regular vacuuming in the bedroom,
where carpets should preferably be avoided.
• Do not keep pets to which there is obvious
allergy.
• The role of diet in atopic eczema is debatable,
and treatments based on changing the diet of
patients are often disappointing.
• It is not certain that the avoidance of dietary
allergens (e.g. cow’s milk and eggs) by a pregnant
or lactating woman lessens the risk of her baby
developing eczema. It may still be wise to
breastfeed children at special risk for 6 months
• Routine inoculations are permissible during quiet phases of
the eczema. However, children who are allergic to eggs
should not be inoculated against measles, influenza and
yellow fever.
• Those with active herpes simplex infections should be
avoided to cut the risk of developing eczema herpeticum
In stubborn cases:
• UVB, UVA-1 (340–400 nm) or even PUVA
• Ciclosporin
• Azathioprine
Other
• Chinese herbal remedies
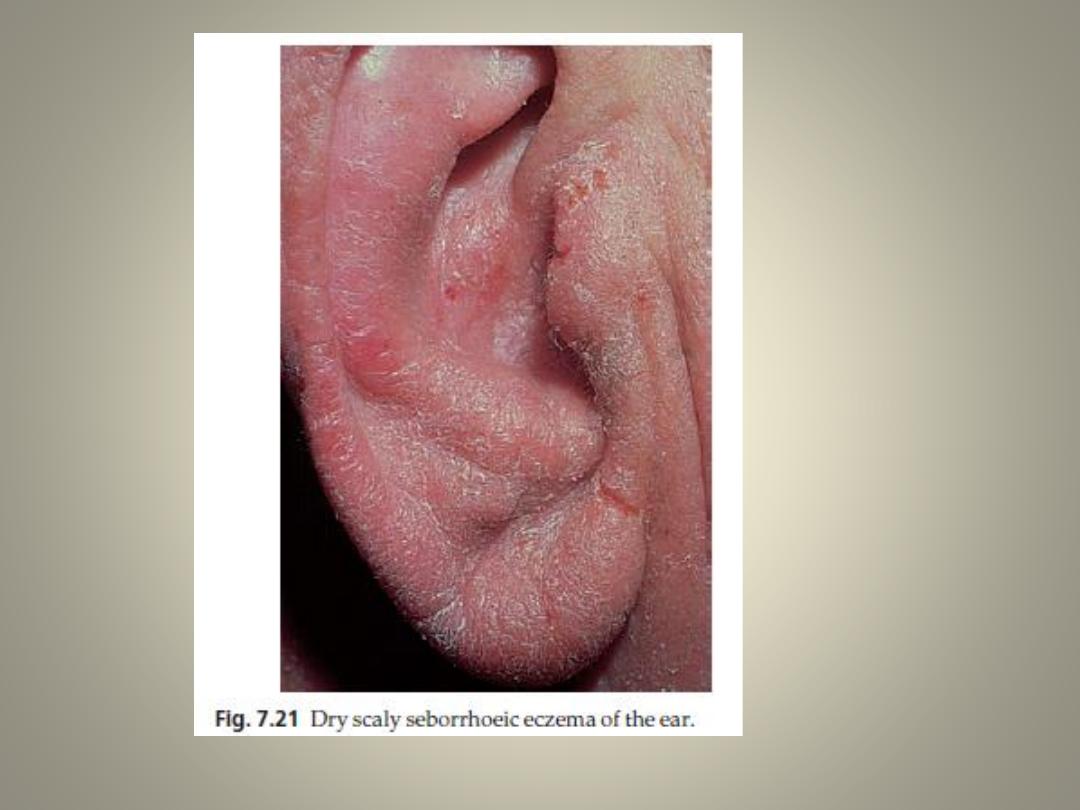
Seborrhoeic eczema
Presentation and course
• mainly affecting hairy areas
• often showing characteristic greasy yellowish scales
• These patterns may merge together
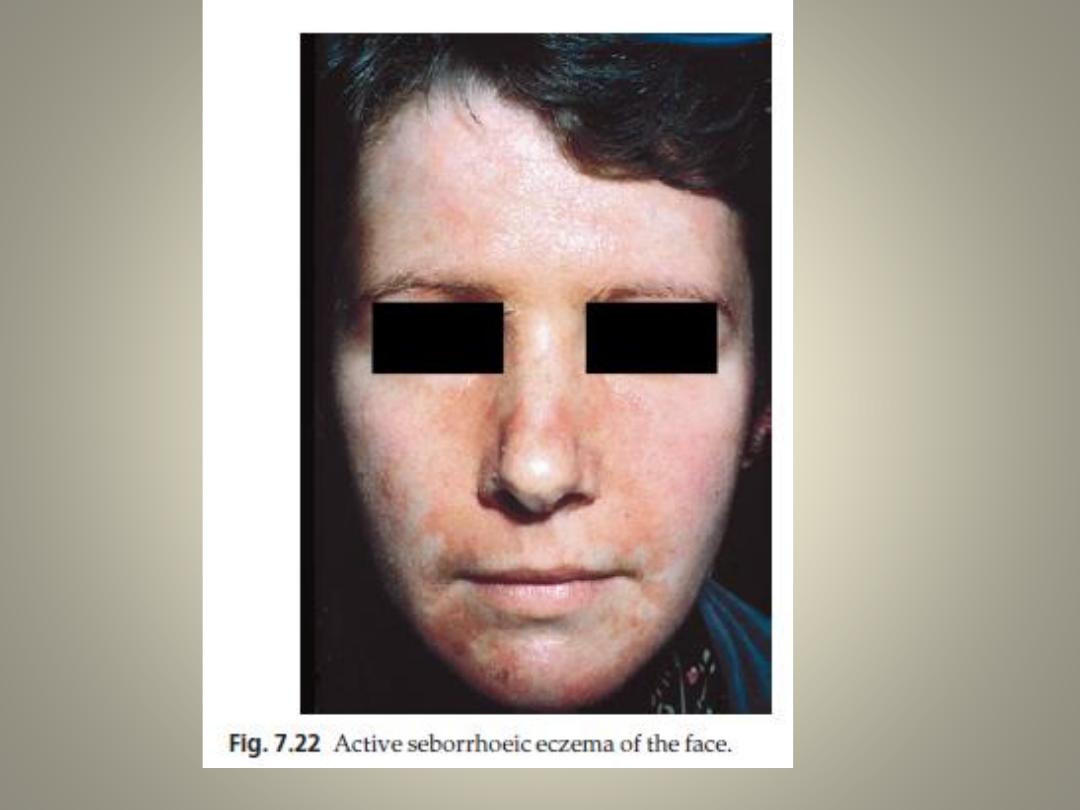
1.
A red scaly or exudative eruption of the scalp, ears, face and
eyebrows.
• May be associated with chronic blepharitis and otitis externa.
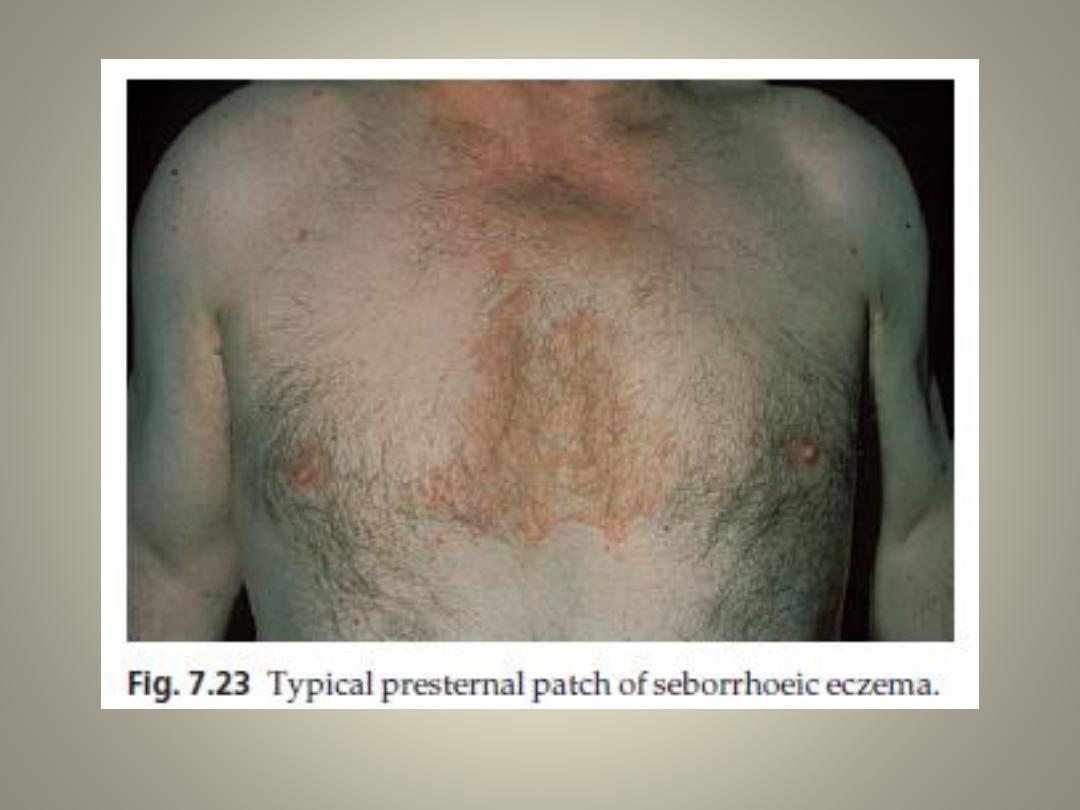
2. Dry scaly ‘petaloid’ lesions of the presternal and interscapular
areas.
• There may also be extensive follicular papules or pustules on the
trunk (seborrhoeic folliculitis or pityrosporum folliculitis).
3. Intertriginous lesions of the armpits, umbilicus or groins, or under
spectacles or hearing aids.
Cause
• not obviously related to seborrhoea.
• It may run in some families
• often affecting those with a tendency to dandruff
• overgrowth of the pityrosporum yeast skin commensals
plays an important part in the development of seborrhoeic
eczema. This fits well with the fact that seborrhoeic eczema
is often an early sign of AIDS, and that it responds to anti-
yeast agents such as topical ketoconazole shampoo or
cream.
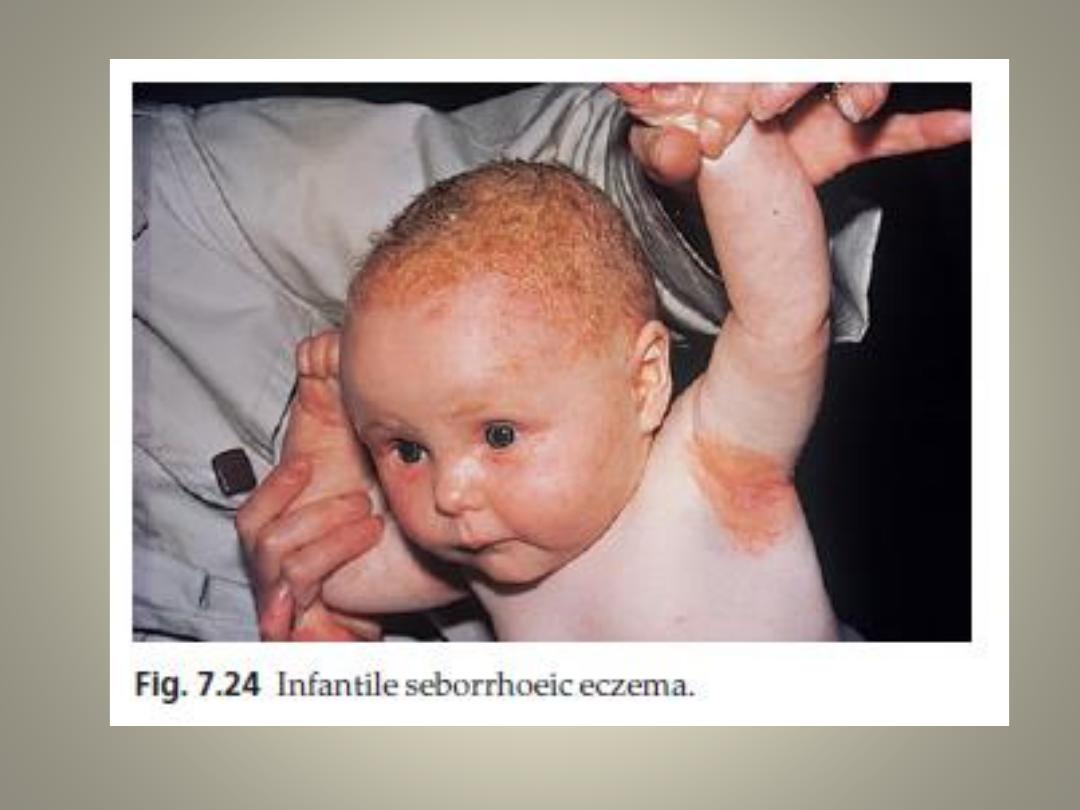
• Seborrhoeic eczema may affect infants but is most common
in adult males.
• In infants it clears quickly but in adults its course is
unpredictable and may be chronic or recurrent
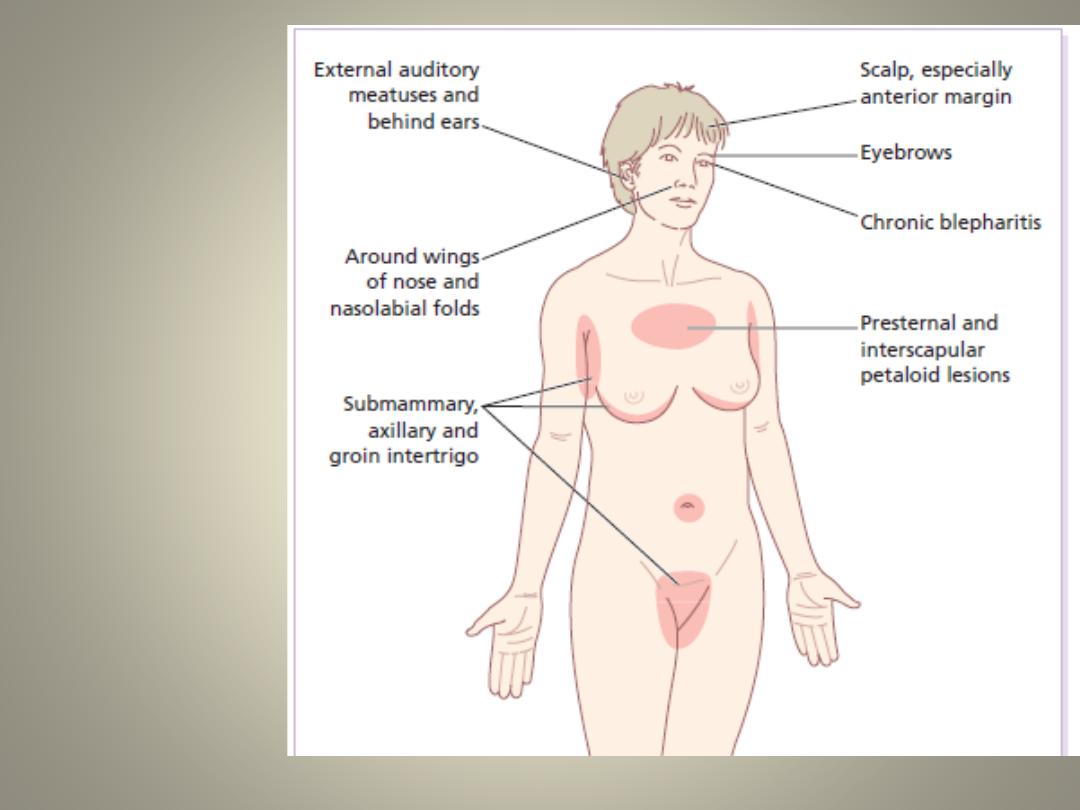
Areas most
often affected
by seborrhoeic
eczemaAreas
most often
affected
by seborrhoeic
eczema
Complications
• Furunculosis
• In the intertriginous type, superadded
Candida infection is common.
Investigations
• None are usually needed, but bear possible
HIV infection and Parkinson’s disease in mind.
Treatment
• Therapy is suppressive rather than curative and
patients should be told this
• Topical imidazoles are perhaps the first line of
treatment.
• 2 % sulphur and 2% salicylic acid in aqueous cream , It
may be used on the scalp overnight
• Shampoo contain ketoconazole, tar, salicylic acid,
sulphur, zinc or selenium sulphide
• For intertriginous lesions, a weak steroid – antiseptic or
steroid – antifungal combination is often effective.
• For severe and unresponsive cases a short course of
oral itraconazole may be helpful.
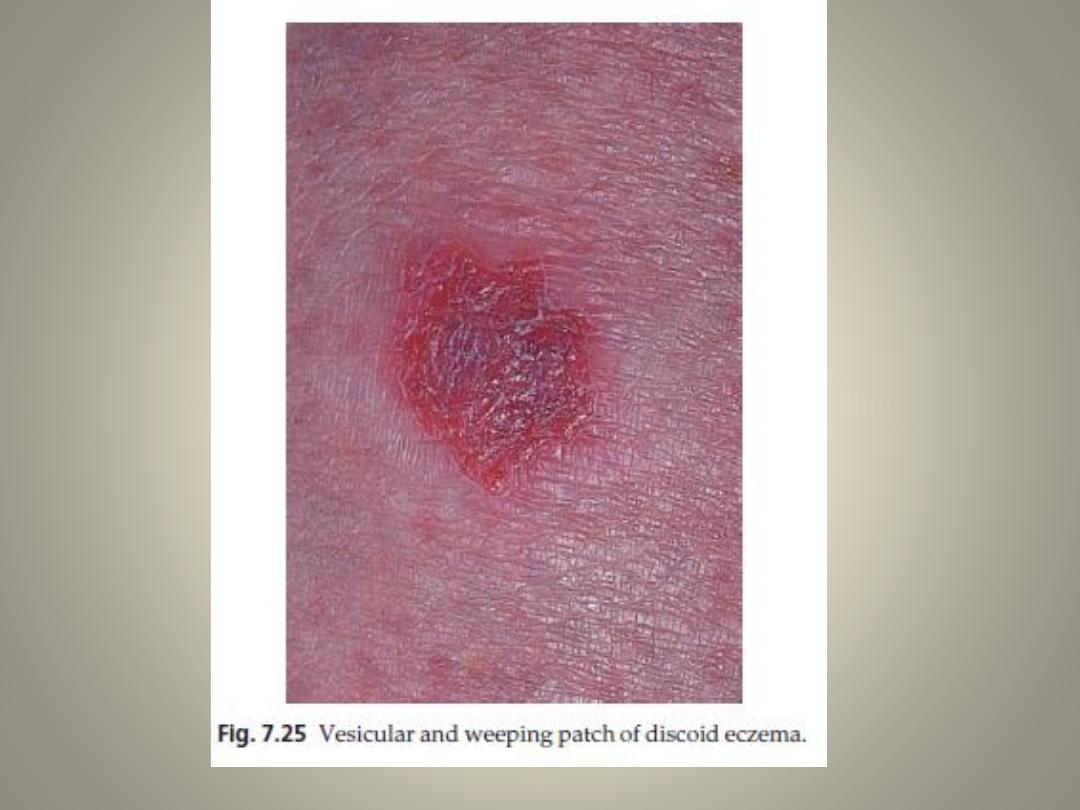
Discoid (nummular) eczema
Cause
• No cause has been established but chronic stress is often present.
• A reaction to bacterial antigens has been suspected as the lesions
often yield staphylococci on culture, and as steroid–antiseptic or
steroid–antibiotic mixtures do better than either separately.
Presentation and course
• common pattern of endogenous eczema
• classically affects the limbs of middle-aged males
• The lesions are multiple, coin-shaped, vesicular or crusted, highly
itchy plaques, usually less than 5 cm across.
• The condition tends to persist for many months, and recurrences
often appear at the site of previous plaques.
Treatment
• With topical steroid–antiseptic or steroid–antibiotic combinations
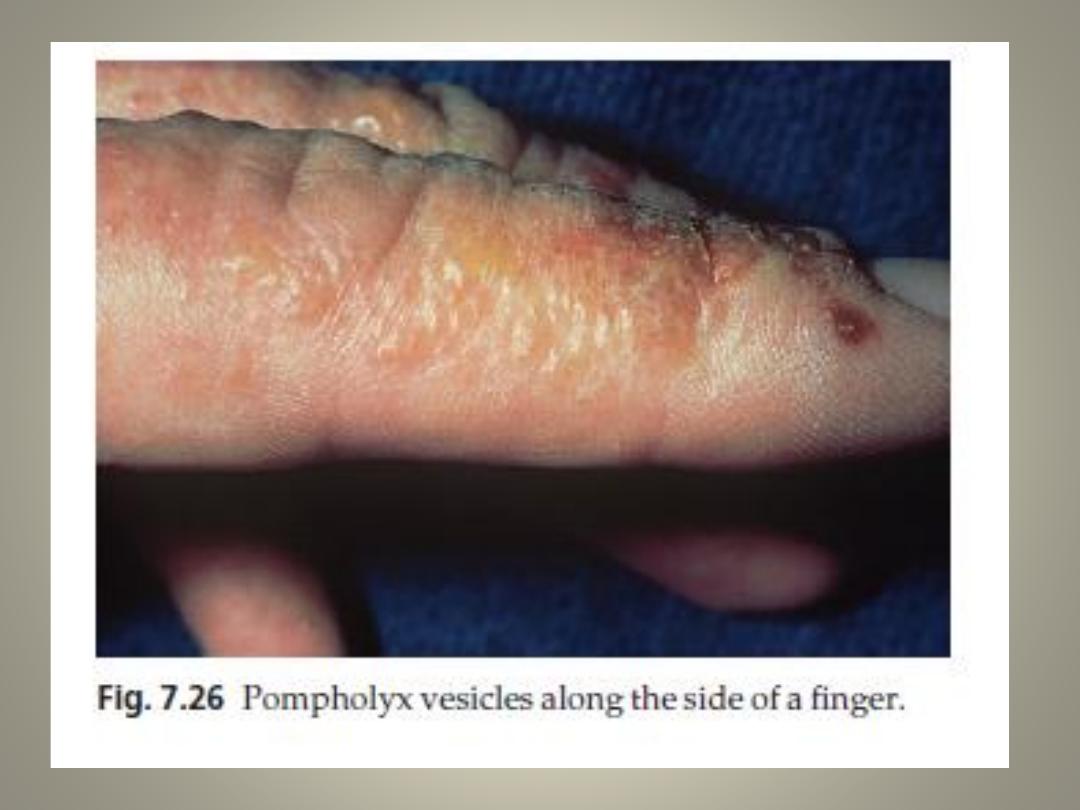
Pompholyx
Cause
• cause is usually unknown, but is sometimes provoked
by heat or emotional upsets or small amounts of nickel
in food, in subjects allergic to nickel
• The vesicles are not plugged sweat ducts.
Presentation and course
• It is tiresome and sometimes very unpleasant form of
eczema
• recurrent bouts of vesicles or larger blisters appear on
the palms, fingers and/or the soles of adults.
• Bouts lasting a few weeks recur at irregular intervals.
• Secondary infection and lymphangitis are a recurrent
problem
Investigations
• Sometimes a pompholyx like eruption of the hands can
follow acute tinea pedis (an ‘ide reaction’).
• Swabs from infected vesicles should be cultured for
bacterial pathogens.
Treatment
• Aluminium acetate or potassium permanganate soaks,
followed by applications of a very potent corticosteroid
cream, are often helpful.
• Appropriate antibiotics should be given for bacterial
infections.
Gravitational (stasis) eczema
Cause
• Poor circulation, often accompanied by obvious venous
insufficiency.
Presentation and course
• A chronic patchy eczematous condition of the lower legs,
sometimes accompanied by varicose veins, oedema and
haemosiderin deposition
• When severe it may spread to the other leg or even become
generalized.
Complications
• Sensitization to local antibiotic applications or to the preservatives
in medicated bandages.
• Ulcer
Gravitational (stasis) eczema
Treatment
• elimination of oedema by elevation, pressure
bandages or diuretics.
• A moderately potent topical steroid may be
helpful, but stronger ones are best avoided.
• Bland applications (e.g. Lassar’s paste or zinc
cream BNF, or medicated bandages)
• It is liable to persist, despite surgery to the
underlying veins.

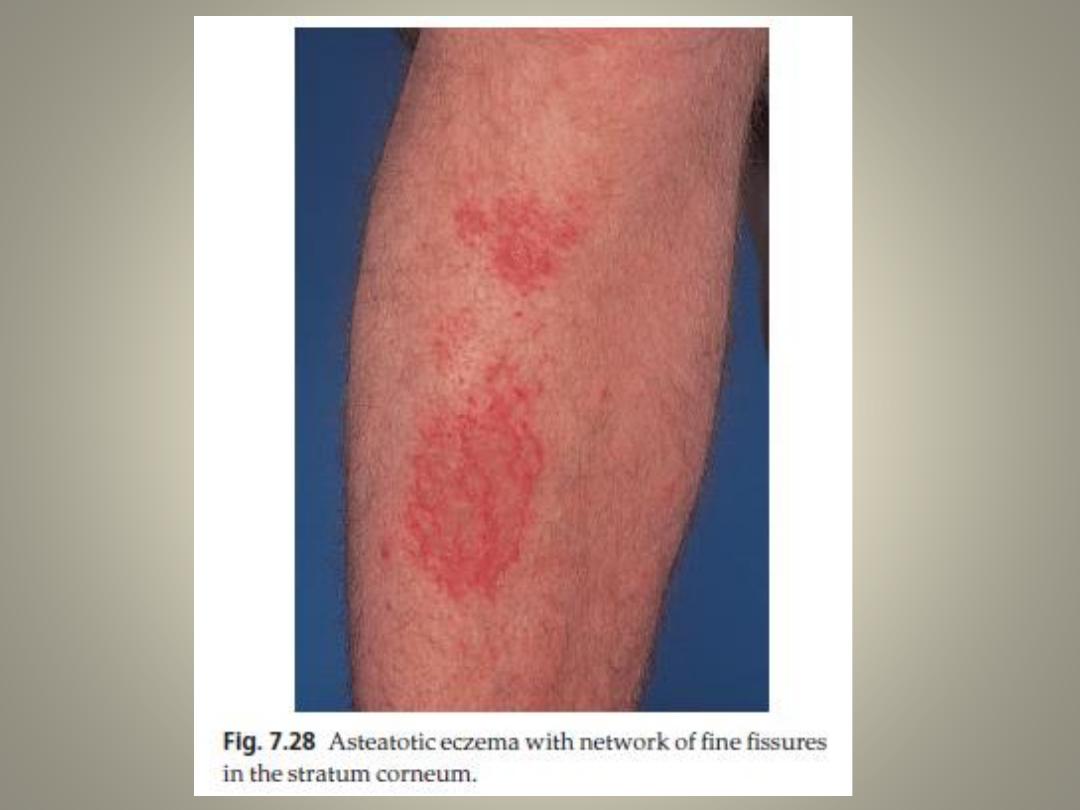
Asteatotic eczema
Cause
• Occur in old age patients always have had a dry skin and a tendency to
chap.
• the removal of surface lipids by over-washing, the low humidity of winter
and central heating, the use of diuretics and hypothyroidism play a rule.
Presentation and course
• common and itchy pattern of eczema occurs usually on the legs of elderly
patients.
• Against a background of dry skin, a network of fine red superficial fissures
creates a ‘crazy paving’ appearance
• Very extensive cases may be part of malabsorption syndromes, zinc
deficiency or internal malignancy.
Treatment
• A mild or moderately potent topical steroid in a greasy base, and aqueous
cream as a soap substitute for the area. Baths should be restricted until
clearance. Thereafter, daily use of unmedicated emollients usually
prevents recurrence.
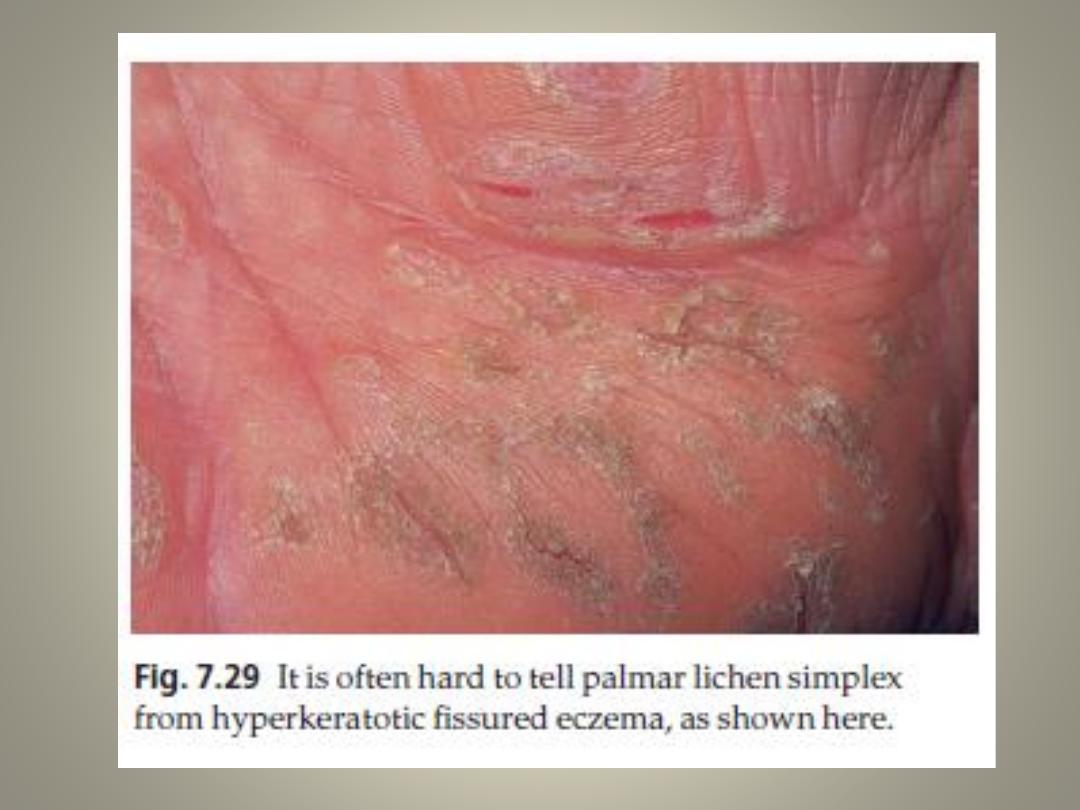
Localized neurodermatitis (lichen simplex)
Cause
• The skin is damaged as a result of repeated rubbing or scratching,
as a habit or in response to stress, but there is no underlying skin
disorder.
Presentation and course
• A single, fixed, itchy, lichenified plaque
• Favourite areas are the nape of the neck in women, the legs in men
and the anogenital area in both sexes.
• Lesions may resolve with treatment but tend to recur either in the
same place or elsewhere.
Treatment
• Potent topical steroids or occlusive bandaging, where feasible, help
to break the scratch–itch cycle.
• Tranquillizers are often disappointing.
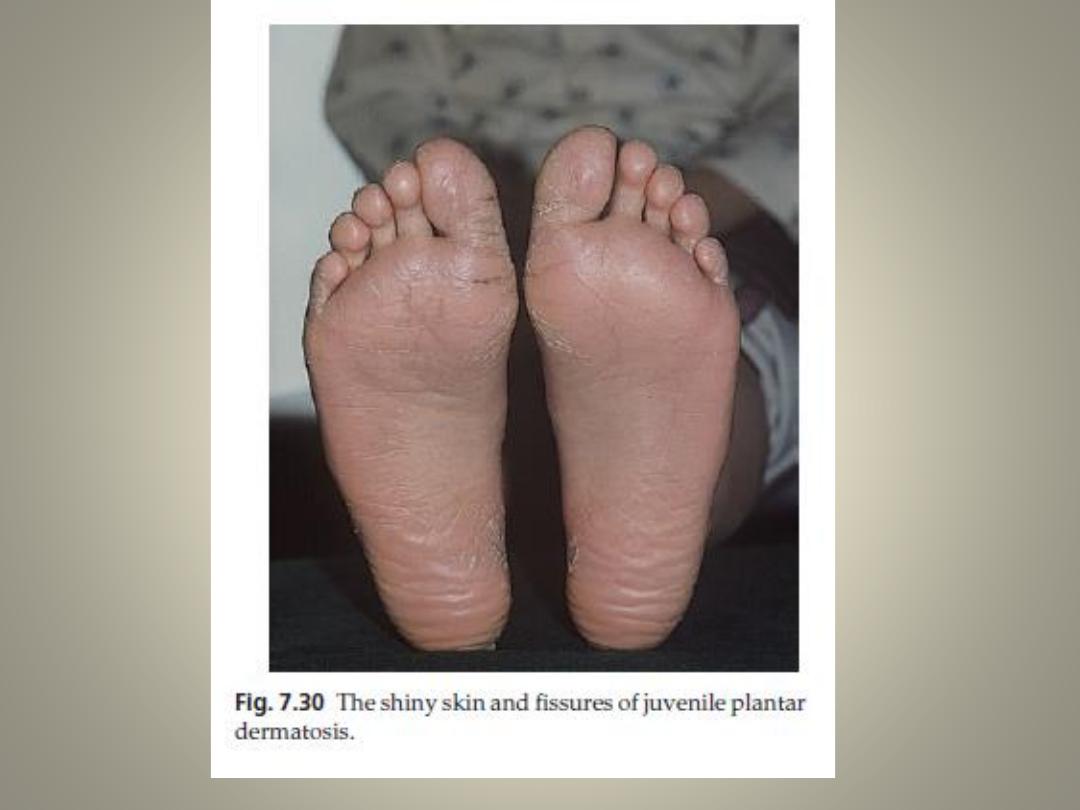
Juvenile plantar dermatosis
Cause
• This condition is thought to be related to the impermeability of modern
socks and shoe linings with subsequent sweat gland blockage, and so has
been called the ‘toxic sock syndrome’! Some feel the condition is a
manifestation of atopy.
Presentation and course
• The skin of the weight-bearing areas of the feet, particularly the forefeet
and undersides of the toes,
• becomes dry and shiny with deep painful fissures that make walking
difficult.
• The toe webs are spared.
• Onset can be at any time after shoes are first worn, and even if untreated
the condition clears in the early teens.
Treatment
• wear cotton or wool socks.
• An emollient such as emulsifying ointment or 1% ichthammol paste, or an
emollient containing lactic acid, is as good as a topical steroid.
Napkin (diaper) dermatitis
Cause
• The most common type of napkin eruption is irritant in origin, and is
aggravated by the use of waterproof plastic pants and the overgrowth of
yeasts.
• The mixture of faecal enzymes and ammonia produced by urea-splitting
bacteria, if allowed to remain in prolonged contact with the skin, leads to
a severe reaction.
Presentation
• The moist, often glazed and sore erythema affects the napkin area
generally with the exception of the skin folds, which tend to be spared.
Complications
• Superinfection with Candida albicans is common, and this may lead to
small erythematous papulesor vesicopustules appearing around the
periphery of the main eruption.
Differential diagnosis
• infantile seborrhoeic eczema
• candidiasis.
Treatment
• It is never easy to keep this area clean and dry, but this is
the basis of all treatment.
• superabsorbent diaper is best and should be changed
regularly, especially in the middle of the night.
• The area should be cleaned at each nappy change with
aqueous cream and water.
• Protective ointments (e.g. zinc and castor oil ointment) or
silicone protective ointments are often useful
• As are topical imidazole preparations that stop yeast
growth
• Potent steroids should be avoided but combinations of
hydrocortisone with antifungals or antiseptics are often
useful

The END