Drug eruptions
Drug eruptions
• Almost any drug can cause a cutaneous
reaction
• Many inflammatory skin conditions can be
caused or exacerbated by drugs
Mechanisms
1. Non-allergic drug reactions
• result of overdosage, accumulation of drugs,
unwanted pharmaco-logical effects,
idiosyncratic, or a result of alterations of
ecological balance
• They are a normal biological effect
• often predictable
• affect many, or even all, patients taking the
drug at a sufficient dosage for a sufficient time
Mechanisms
2. Allergic drug reactions
• less predictable.
• occur in only a minority of patients receiving a drug
• occur even with low doses
• They are not a normal biological effect of the drug and
usually appear after the latent period required for
induction of an immune response
• Chemically related drugs may cross-react
• majority of allergic drug reactions are caused by cell-
mediated immune reaction
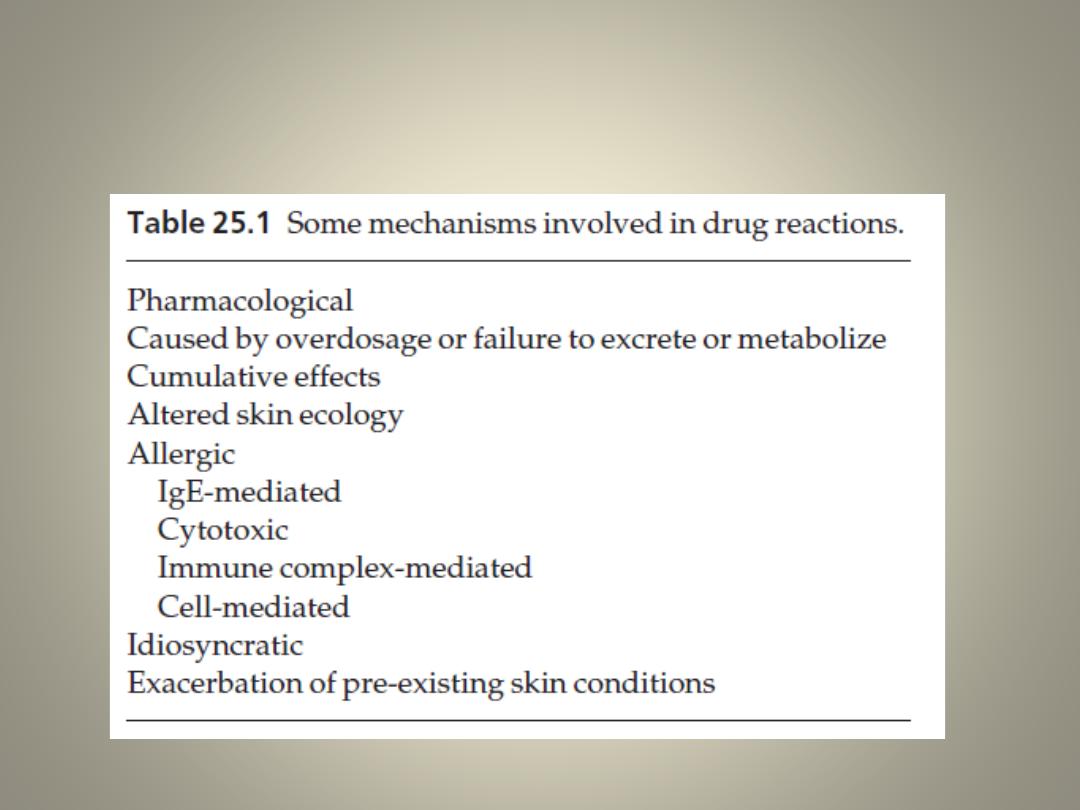
Some mechanisms involved in drug
reactions
Presentation
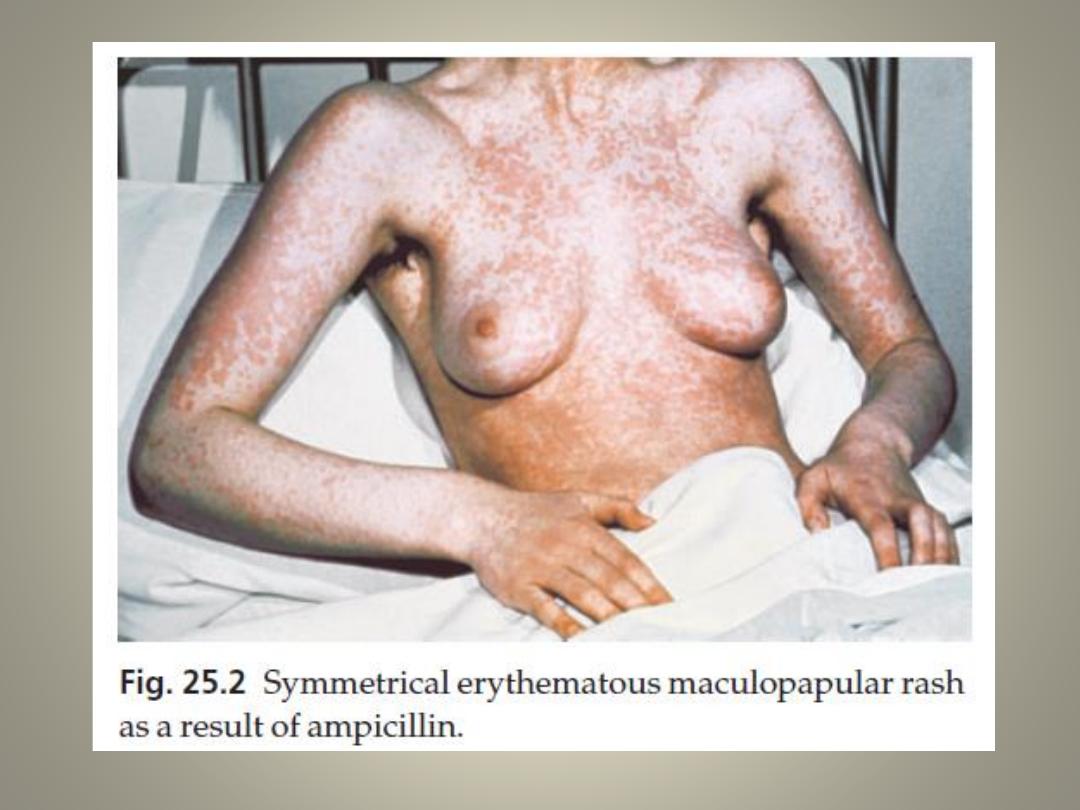
Antibiotics
Penicillins and sulphonamides
• are most commonly causing allergic reactions.
• These are often morbilliform but urticaria, erythema multiforme and fixed
eruptions are common too.
• DDx. Is viral infections as often associated with exanthems
• Most patients with infectious mononucleosis develop a morbilliform rash
if ampicillin is administered.
• Penicillin is a common cause of severe anaphylactic reactions, which can
be life-threatening.
Minocycline
• can accumulate in the tissues and produce a brown or grey colour in the
mucosa, sun-exposed areas or at sites of inflammation, as in the lesions of
acne
• hepatitis, worsen lupus erythematosus or elicit a transient lupus-like
syndrome
Oral contraceptives
• Reactions to these are less common now that
their hormonal content is small.
1. telogen effluvium
2. Melasma, hirsutism
3. erythema nodosum
4. acne
5. photosensitivity
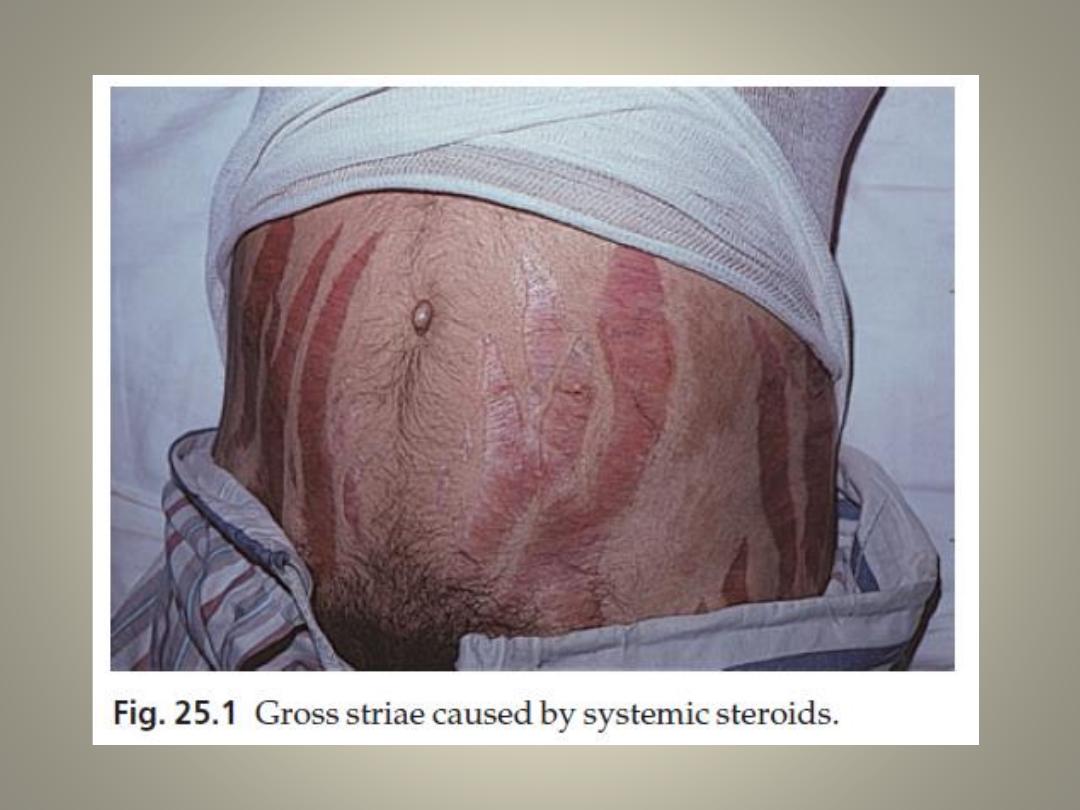
Steroids
Cutaneous side-effects from systemic steroids
include:
• a ruddy face
• cutaneous atrophy
• striae
• hirsutism
• an acneiform eruption
• a susceptibility to cutaneous infections, which
may be atypical
Anticonvulsants
Skin reactions to phenytoin, carbamazepine,
lamotrigine and phenobarbital are common
and include:
• erythematous, morbilliform, urticarial and
purpuric rashes.
• rarely TEN, erythema multiforme, exfoliative
dermatitis, DRESS syndrome and a lupus
erythematosuslike syndrome
Some common reaction patterns and
drugs that can cause them
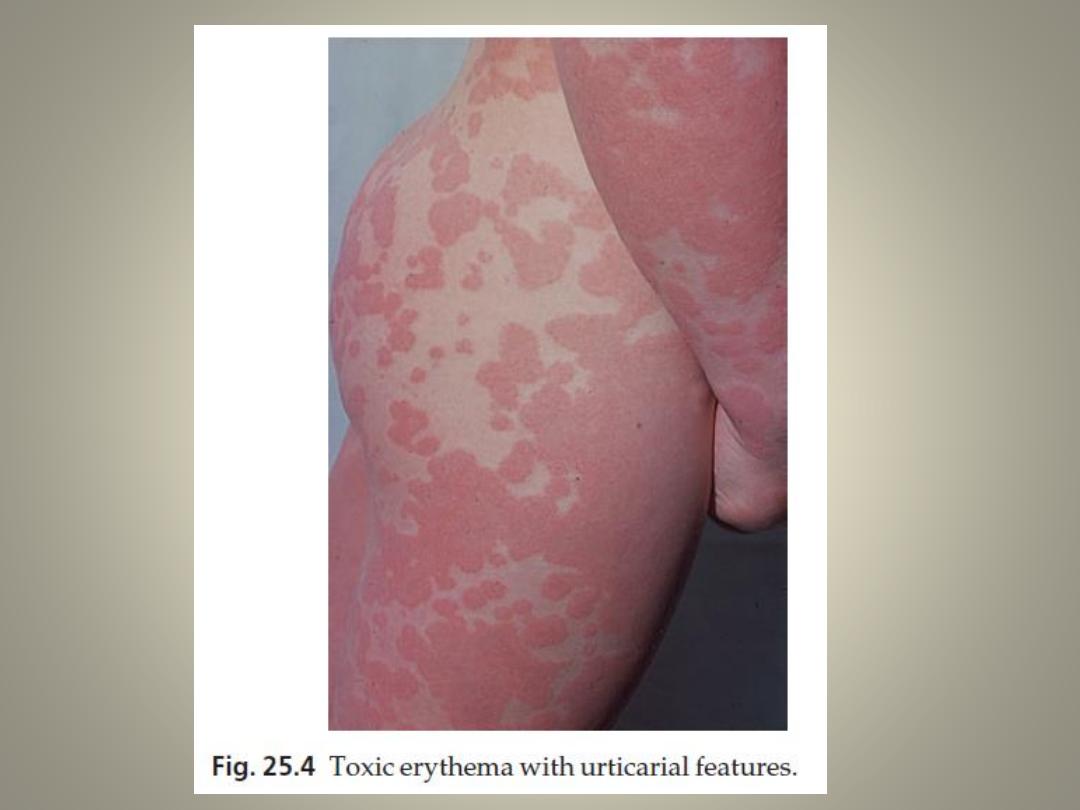
Toxic (reactive) erythema
• most common type of drug eruption
• looking like measles or scarlet fever, and
sometimes showing prominent urticarial or
erythema multiforme-like elements.
• Itching and fever may accompany the rash.
• Culprits include antibiotics (especially ampicillin),
sulphonamides and related compounds (diuretics
and hypoglycaemics) and barbiturates
Urticaria
• salicylates are the most common, often working non-
immunologically as histamine releasers.
• Antibiotics
• Urticaria may be part of a severe and generalized reaction
(anaphylaxis) that includes bronchospasm and collapse
Erythema multiforme and Stevens–Johnson syndrome
• Sulphonamides, barbiturates, lamotrigine and
phenylbutazone
Purpura
• Thiazides, sulphonamides, barbiturates and anticoagulants
Bullous eruptions
• also in Stevens–Johnson syndrome
• Vancomycin, lithium, diclofenac, captopril, furosemide and
amiodarone are associated with development of linear IgA
bullous disease
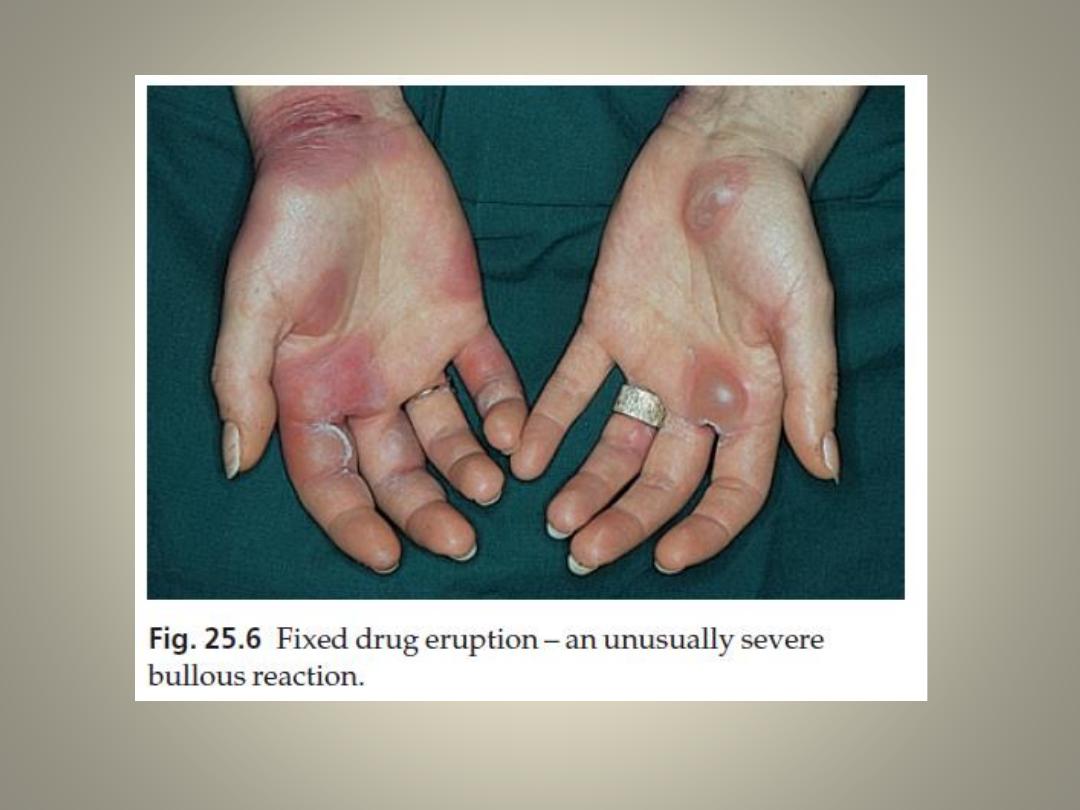
Fixed drug eruptions
• Round erythematous or purple, and sometimes bullous
plaques recur at the same site each time the drug is taken
• Pigmentation persists between acute episodes.
• The glans penis seems to be a favoured site.
• The causes of fixed drug eruptions in any country follow the
local patterns of drug usage
• Paracetamol is currently the most common offender in the
UK
• Trimethoprim-sulfa leads the list in the USA
• NSAIDs (including aspirin), antibiotics, systemic antifungal
agents and psychotropic drugs lie high on the list of other
possible offenders.
Acneiform eruptions
• Lithium, iodides, bromides
• oral contraceptives, androgens or glucocorticosteroids
• Antitub erculosis and anticonvulsant
Lichenoid eruptions
• These resemble lichen planus but mouth lesions are
uncommon and scaling and eczematous elements may
be seen.
• antimalarials, NSAIDs, gold, phenothiazines
Hair loss
• Retinoid
• cytotoxic agents
• oral contraceptive
Hypertrichosis
• dose-dependent effect of diazoxide, minoxidil
and ciclosporin
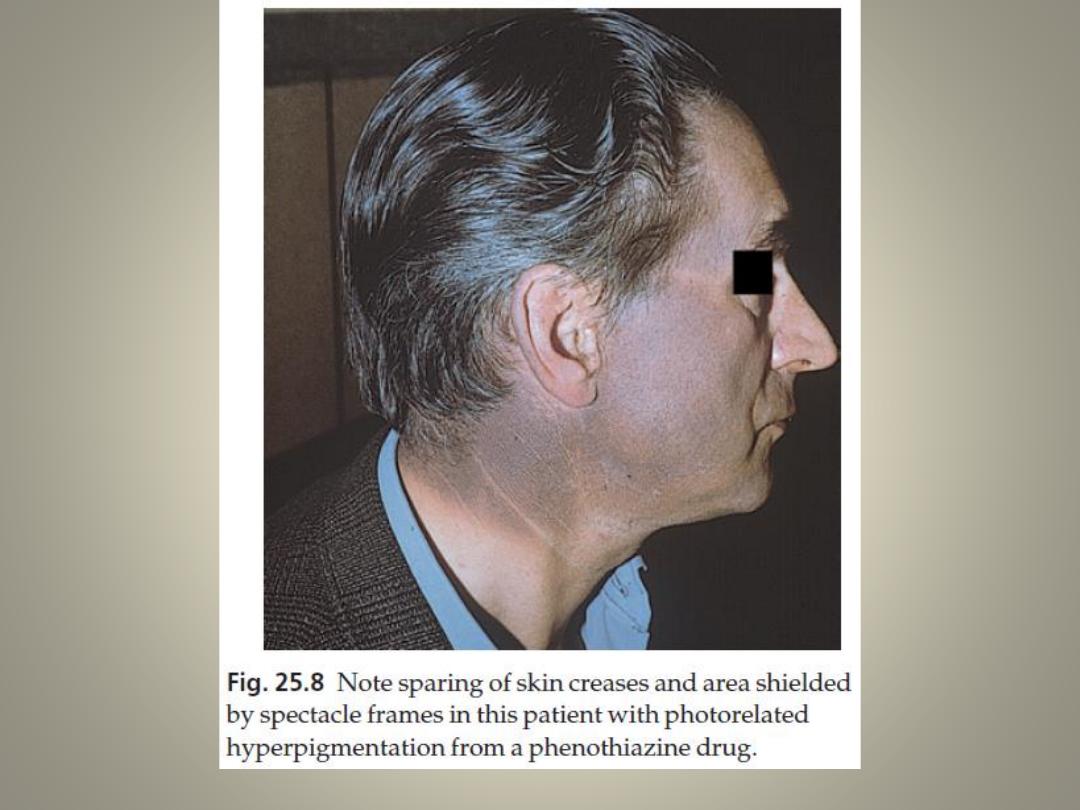
Pigmentation
• Melosma in oral contraceptive plus sun exposure
• Large doses of phenothiazines impart a blue–grey colour to
exposed areas
• clofazimine makes the skin red
• mepacrine turns the skin yellow
• minocycline turns areas of leg skin a curious greenish grey
colour
Xerosis
• oral retinoids
• nicotinic acid
• lithium
Course
• If an allergic reaction occurs during the first
course of treatment, it characteristically begins
late, often about the ninth day, or even after the
drug has been stopped
• In previously exposed patients the common
morbilliform allergic reaction starts 2–3 days after
the administration of the drug
• The speed with which a drug eruption clears
depends on the type of reaction and the rapidity
with which the drug is eliminated
Differential diagnosis
• Ranges over the whole subject of dermatology
• The general rule is never to forget the
possibility of a drug eruption when an atypical
rash is seen. Six vital questions should be
asked
The six vital questions to be asked
when a drug eruption is suspected.
1. Can you exclude a simple dermatosis (e.g. scabies or
psoriasis) and the known skin manifestations of an
underlying disorder (e.g. systemic lupus erythematosus)?
2. Does the rash itself suggest a drug eruption (e.g. urticaria,
erythema multiforme)?
3. Does a past history of drug reactions correlate with
current prescriptions?
4. Was any drug introduced a few days or weeks before the
eruption appeared?
5. Which of the current drugs most commonly cause drug
eruptions (e.g. penicillins, sulphonamides, thiazides,
allopurinol, phenylbutazone)?
6. Does the eruption fit with a well-recognized pattern
caused by one of the current drugs (e.g. an acneiform rash
from lithium)?
Treatment
• The first approach is to withdraw the suspected drug,
accepting that several drugs may need to be stopped at
the same time.
• The decision to stop or continue a drug depends upon:
1. the nature of the drug
2. the necessity of using the drug for treatment
3. the availability of chemically unrelated alternatives
4. the severity of the reaction, its potential reversibility
5. the probability that the drug is actually causing the
reaction.
• Every effort must be made to correlate the
onset of the rash with prescription records.
• Often, but not always, the latest drug to be
introduced is the most likely culprit.
• Prick tests and in vitro tests for allergy are
unreliable to
• Re-administration, as a diagnostic test, is
usually unwise except when no suitable
alternative drug exists
Non-specific therapy depends upon the type of
eruption.
• In urticaria, antihistamines are helpful.
• In some reactions, topical or systemic
corticosteroids can be used, and applications
of calamine lotion may be soothing.
• Plasmapheresis and dialysis can be considered
in certain life-threatening situations
Anaphylactic reactions
• ensure that the airway is not compromised (e.g. oxygen, assisted
respiration or even emergency tracheostomy).
• One or more injections of adrenaline (epinephrine) (1 : 1000) 0.3–
0.5 mL should be given subcutaneously or intramuscularly in adults
• slow (over 1 min) intravenous injection of chlorphenamine
maleate (10–20 mg diluted in syringe with 5–10 mL blood).
• Although the action of intravenous hydrocortisone (100 mg) is
delayed for several hours, it should be given to prevent further
deterioration in severely affected patients.
• Patients should be observed for 6 h after their condition is stable, as
late deterioration may occur.
• If an anaphylactic reaction is anticipated, patients should be taught
how to self-inject adrenaline, and may be given a salbutamol
inhaler to use at the first sign of the reaction
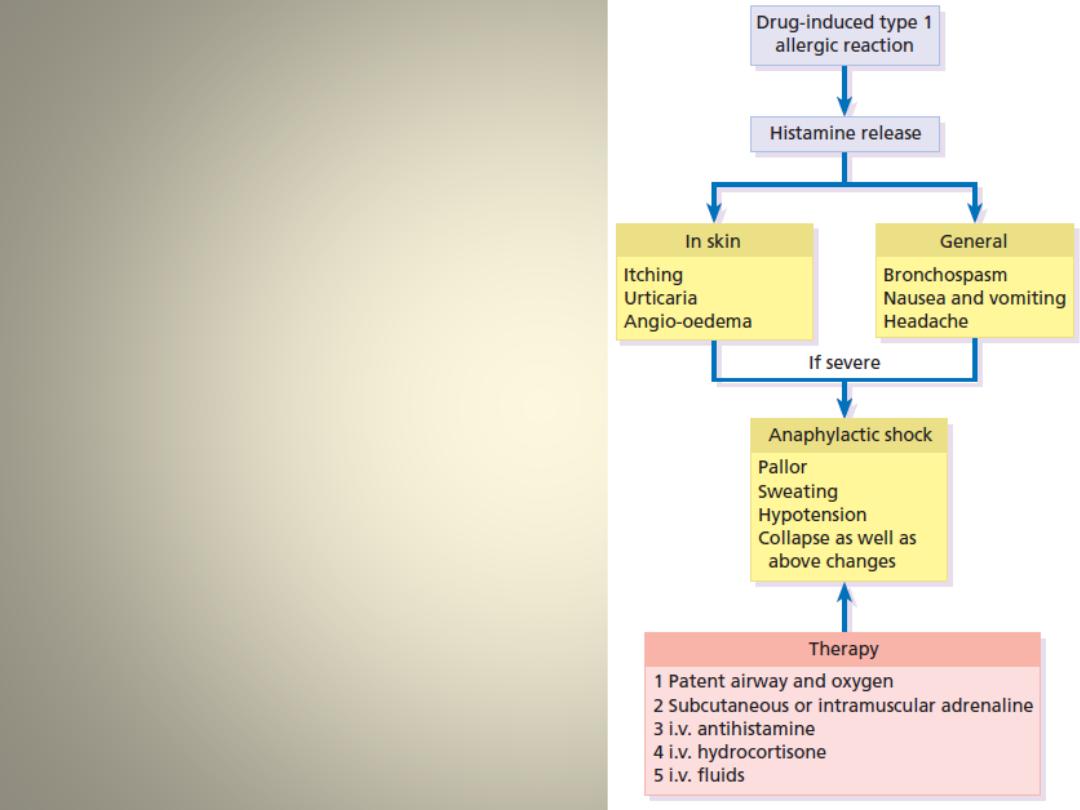
The cause, clinical
features and
treatment of
anaphylaxis.
Desensitization
• is seldom advisable or practical
The End