Pleural Effusion
Tikrit University
College of Medicine
Department of Radiology
Chest Series
Normally
• Pleura
are two membranes around the lungs. These two
membranes are called the visceral and parietal pleurae.
• The lung covered by
visceral pleura.
• The mediastinum, chest wall, and diaphragm are lined by
parietal pleura.
• Both layers are in continuity with each other at the hilum.
• Below hilum, they form the
pulmonary ligament.
• Both pleura are separated by a potential space
(Pleural
Sac)
that normally contains only a few ml of fluid
, <15 ml.
• Radiologically
the normal pleura is a hairline of soft
tissue density which is only seen when it is parallel to the
X-ray beam and flanked by air.
Normal physiology
• Less than
15 ml
of fluid is normally present
in the pleural space.
• Pleural fluid is generated as interstitial fluid
in the parietal pleura, leaking through non-
tight mesothelial junctions into the pleural
space, whence it is removed by bulk flow
through the lymphatics via parietal pleura.
Pleural pathology
• Excess of pleural fluid will accumulates in the
pleural sac when
inflow
and
outflow
from
the pleural space are mismatched.
This occurs when:
1. capillary hydrostatic pressure is increased.
2. blood oncotic pressure is low
(hypoalbunemia)
3. capillary permeability is increased.
4. lymphatic drainage is obstructed.
5. reduction of pleural space pressure.
6. trans-diaphragmatic passage of ascitic fluid.
Types of pleural fluids
• Transudate.
• Exudate (thin or thick).
• Blood
• Chyle.
Trasudate Pleural Effusion
• Usually
bilateral
due
to
systemic
causes.
• Bilateral pleural effusions tend to be transudates
because they develop secondary to generalized
changes that affect both pleural cavities equally
— a rise in capillary pressure or a fall in oncotic
pressure of the blood, (CHR , Hypoalbuminemia,
Cirrhosis ,and Nephrotic syndrome..)
Exudate Pleural Effusion
• Usually unilateral, it could be bilateral
due to local causes.
• Some bilateral effusions are exudates,
however, and this is seen with metastatic
disease, lymphoma, or inflammatory
diseases of the pleura
•
Hemothorax:
• Blood within the pleural cavity ( pleural
fluid hematocrit > 50% blood hematocrit)
Empyema:
• exudative fluid with pus
Chylothorax:
• cholestyrol and or triglyceride increment ..
Remember
Right-sided effusions:
typically associated with:
• Ascites
• heart failure
• liver abscess
• Ovary tumor (due to ascites) .
Left effusions:
seen with
• Pancreatitis
• Pericarditis
• Esophageal rupture
• Aortic dissection.
Radiological signs of a Pleural Effusion
• Subpulmonic effusions.
• Blunted lateral costophrenic angles .
• Meniscus sign.
• Lamellar Effusion.
• Loculated (encysted ,encapsulated )..
• Fissural (Interlobar) Loculation.
• Air – fluid level ..
• Opacified hemithorax .
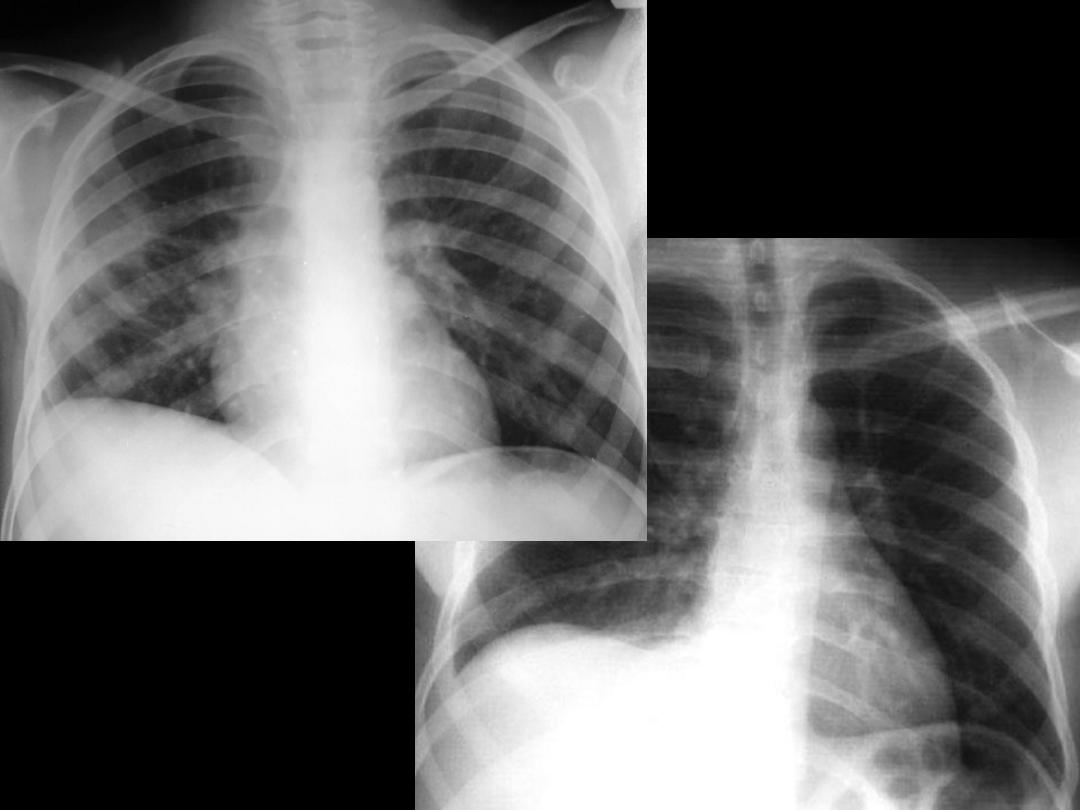
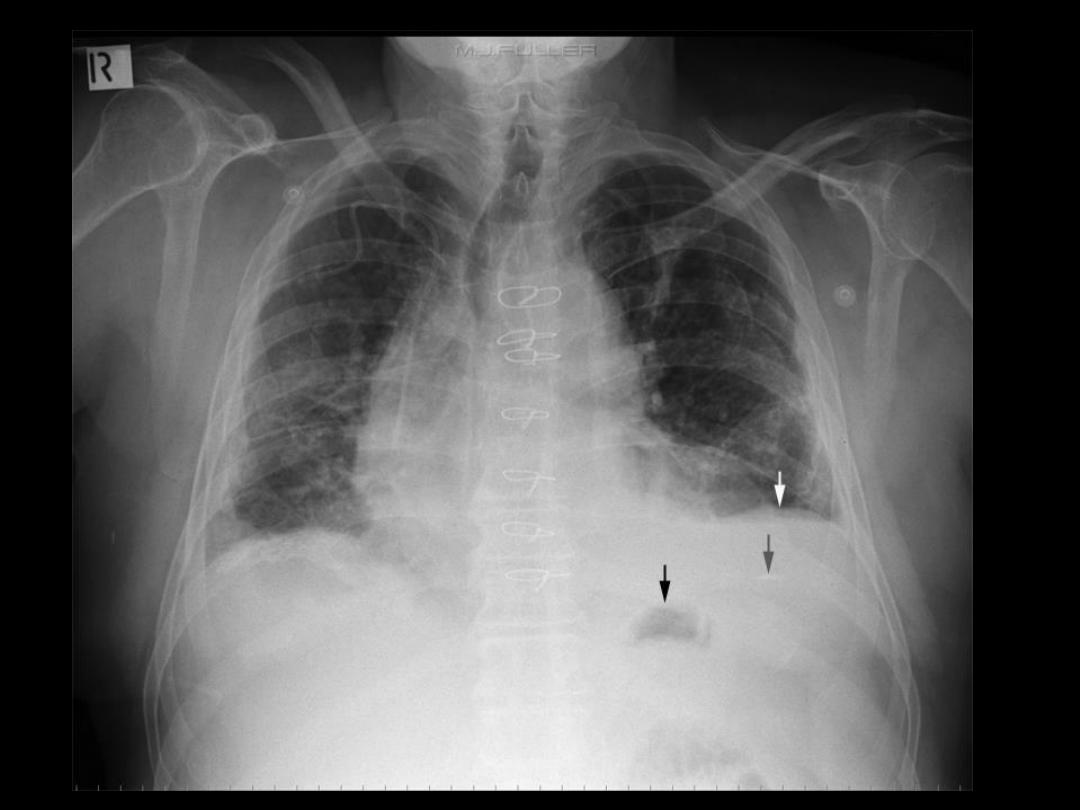
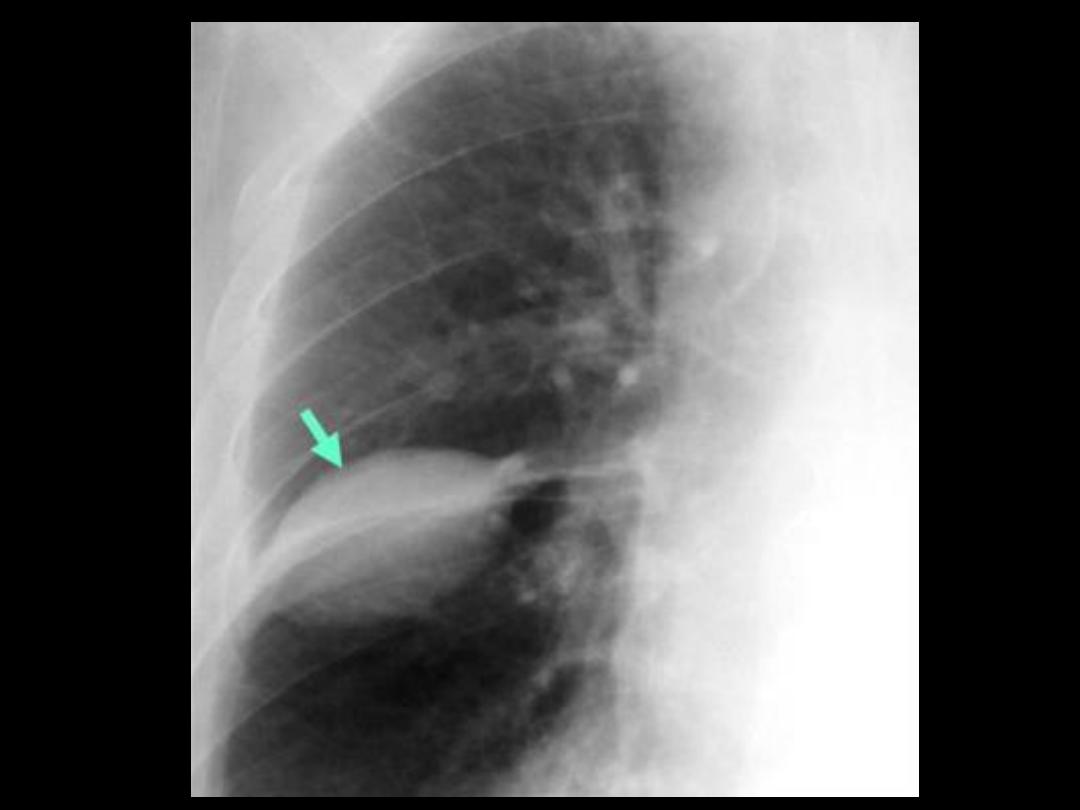
Subpulmonic Effusions
• It is unusual for it to remain localized in this site once its
volume exceeds 200
–300 ml.
• On a Pa film
• The signs are of a 'high hemidiaphragm‘ with an
unusual contour that peaks more laterally than usual
• has a straight medial segment and falls away rapidly to
the costophrenic angle laterally.
• left-sided subpulmonary effusions, there is increased
separation between the stomach gas and the apparent
hemidiaphragm.
Blunting of the CP angle
• Normally there is less than 15 ml pleural
fluid.
• 50 – 100 ml
accumulation is able to blunte
the posterior costophrenic angle seen by
lateral x-ray.
• >
200 ml
needed to blunting the CP angle
seen by frontal film..

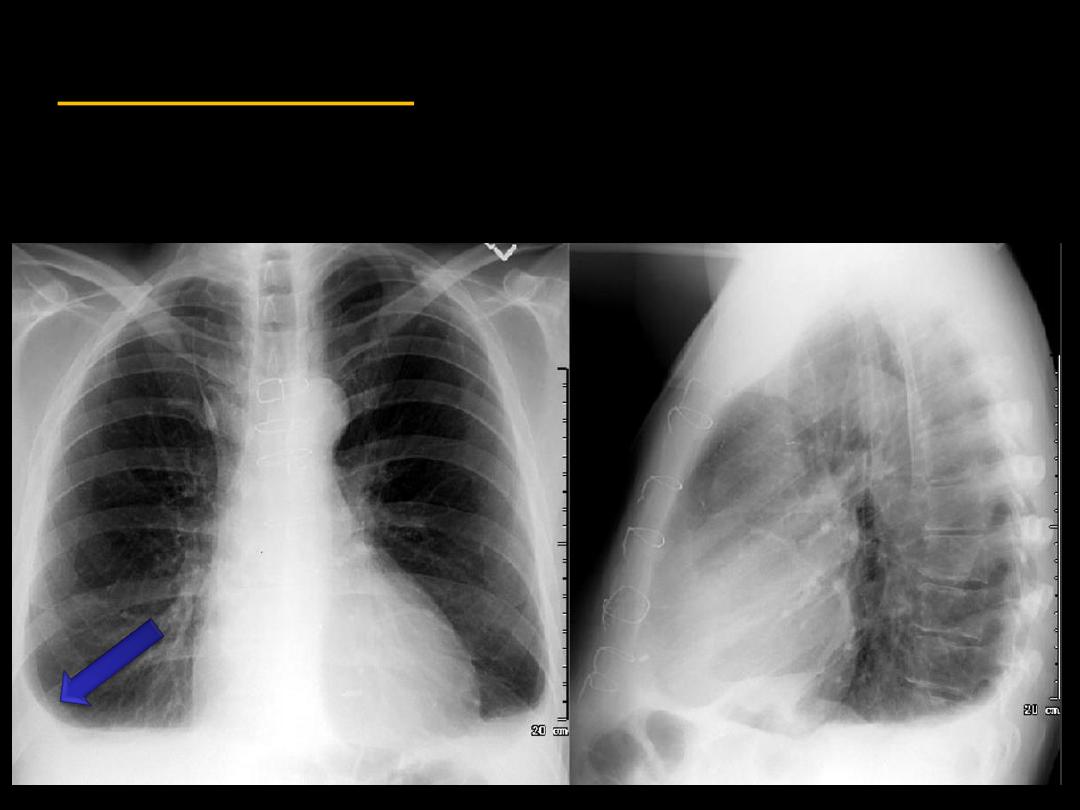
Meniscus sign:
The upper margin of the opacity is concave to the lung
and is higher laterally than medially.
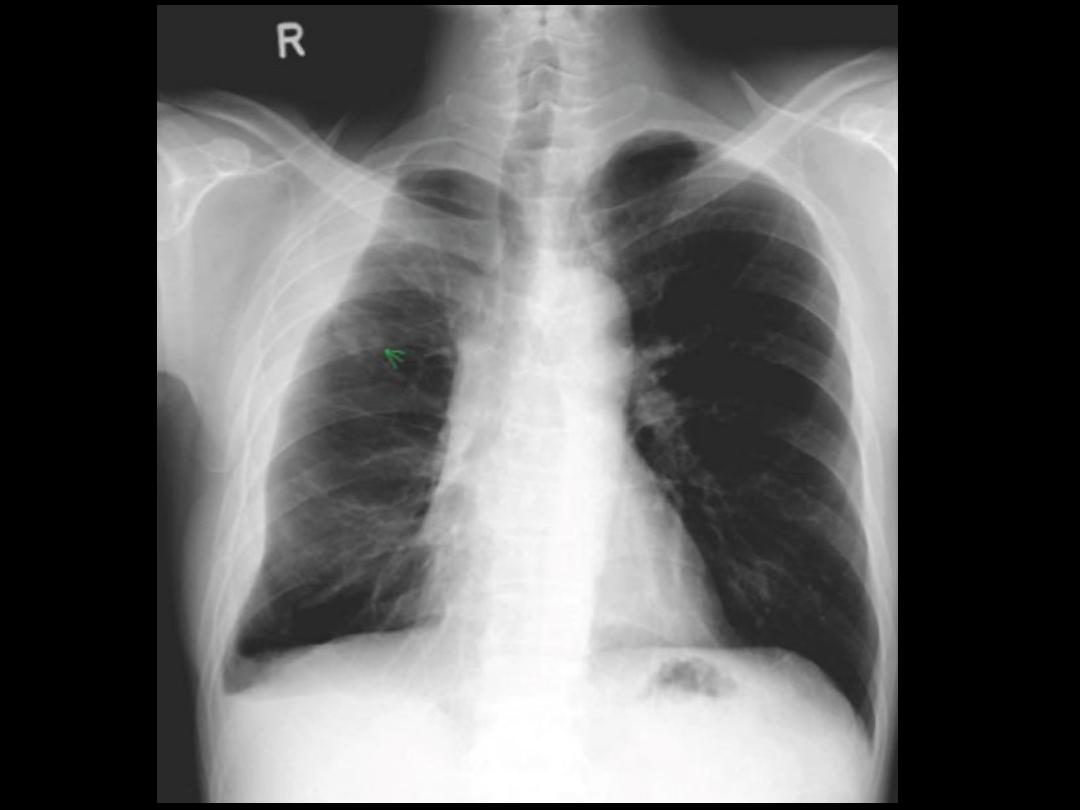
Lamellar Effusion
• A lamellar effusion is caused by fluid
between the lung and visceral pleura and
it is a common finding in
heart failure
.
• It gives a vertical band shadow of soft
tissue density between the lung and the
chest wall above the costophrenic angle,
usually occur with CHF.
Loculated Pleural Effusion
(Encysted, Encapsulated)
•Fluid can loculate between visceral pleural
layers in fissures or between visceral and
parietal layers.
•The shape & position is unusual in thorax.
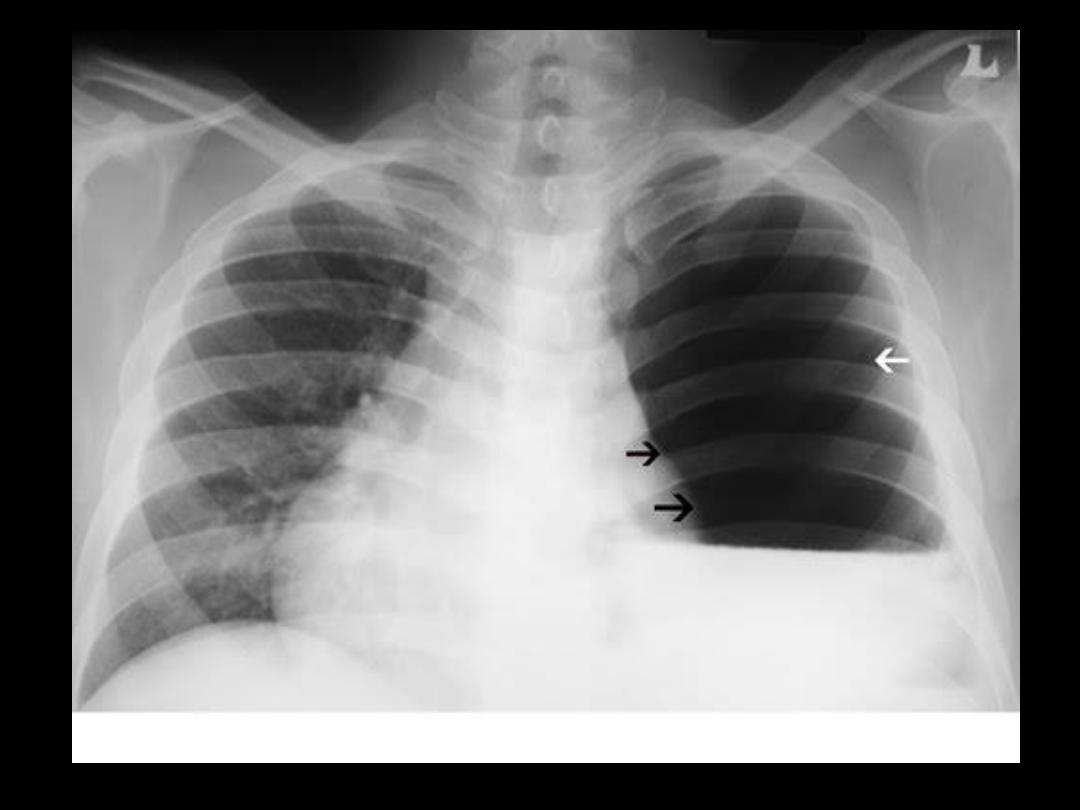
Hydropneumothorax
• air-fluid level occurrence ,when air
(pneumothorax ) present with pleural
effusion
Etiology due to:
– Trauma
– Surgery
– bronchopleural fistula..
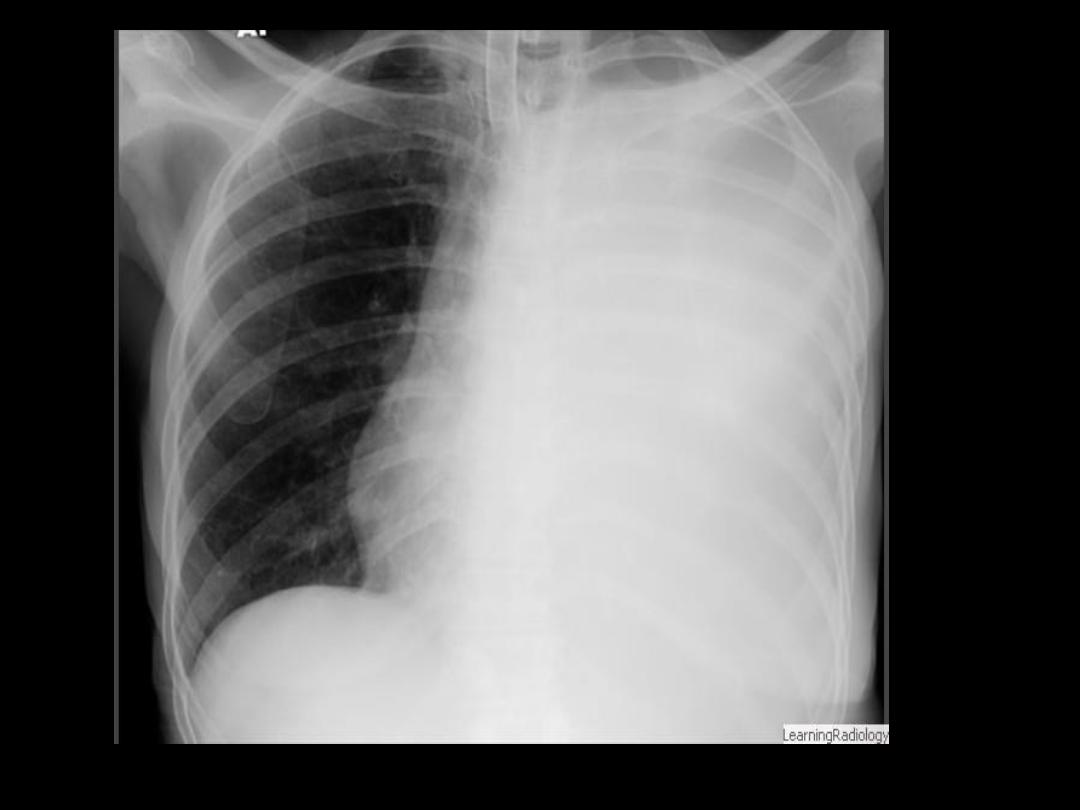
Hemithorax opacification
• The whole hemithorax is opacified
The DDx is broad, and includes
– large pleural effusion
– Empyema
– Hemothorax
– complete lung collapse
– Pneumonectomy
– Community acquired pneumonia
– Bronchogenic carcinoma,
– pleural masses such as