
Injuries to the Genitourinary
Tract
*About 10% of all injuries seen in the emergency
room involve the genitourinary system to some
extent.
*Initial assessment should include control of
hemorrhage and shock along with resuscitation as
required.
*Resuscitation may require intravenous lines and
a urethral catheter in seriously injured patients.

• In men, before the catheter is inserted, the
urethral meatus should be examined carefully for
the presence of blood.
• The abdomen and genitalia should be examined
for evidence of contusions or subcutaneous
hematomas.
• Fractures of the lower ribs are often associated
with renal injuries, and pelvic fractures often
accompany bladder and urethral injuries.

INJURIES TO THE KIDNEY
• Renal injuries are the most common injuries
of the urinary system.
• The kidney is well protected by heavy lumbar
muscles, vertebral bodies, ribs, and the viscera
anteriorly.
• Most injuries occur from automobile accidents
or sporting mishaps, chiefly in men and boys.

Etiology
• Blunt trauma directly to the abdomen, flank,
or back is the most common mechanism,
accounting for 80–85% of all renal injuries.
• Gunshot and knife wounds cause most
penetrating injuries to the kidney; any such
wound in the flank area should be regarded as
a cause of renal injury until proved otherwise.
• Associated abdominal visceral injuries are
present in 80% of renal penetrating wounds.

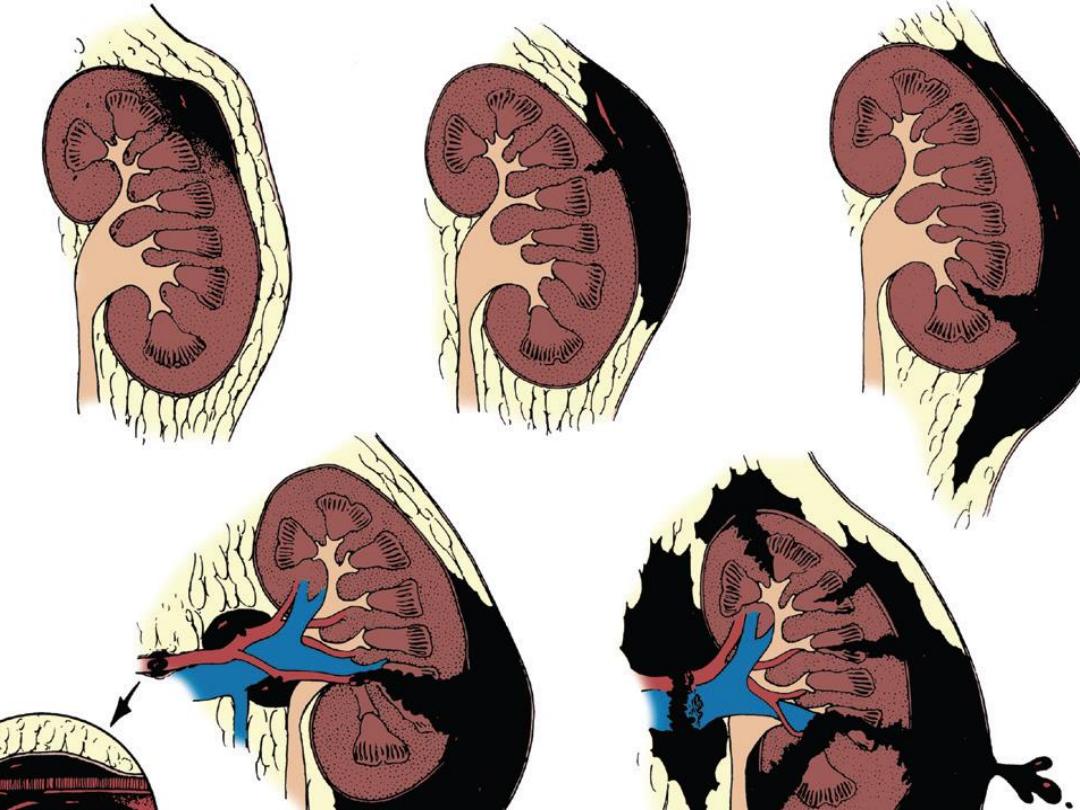
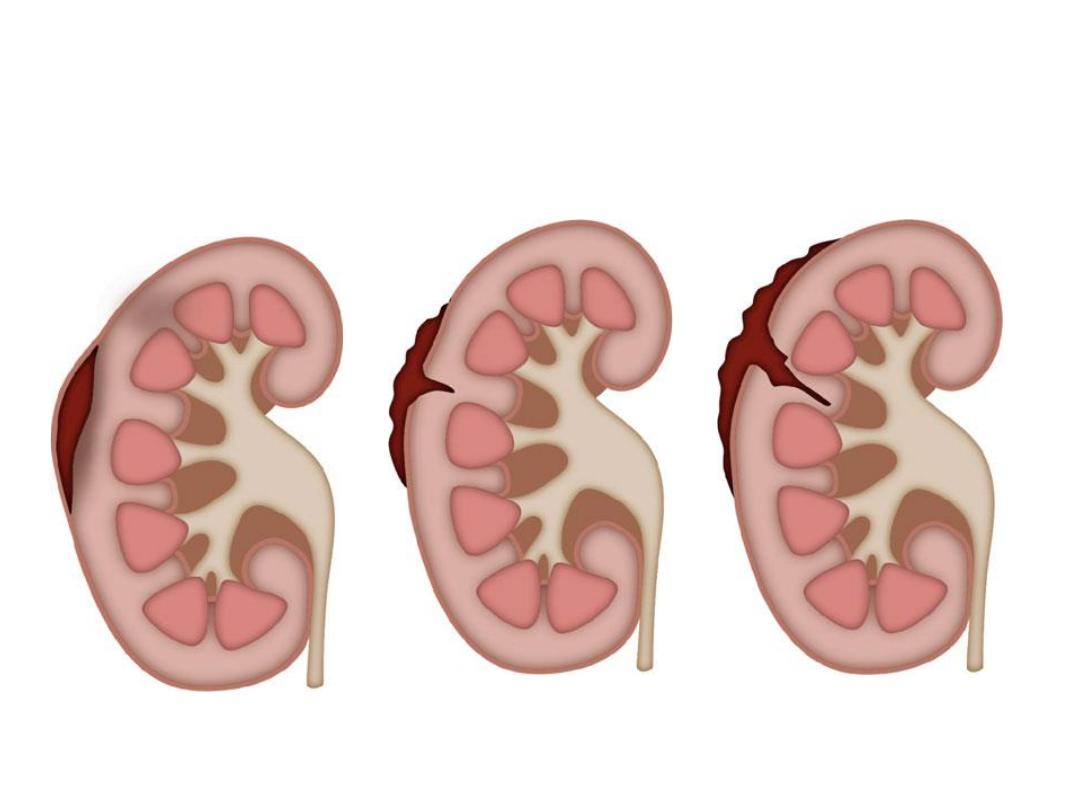
Pathology & Classification
• A.EARLY PATHOLOGIC FINDINGS:
Lacerations from blunt trauma usually occur in the
transverse plane of the kidney. The mechanism of
injury is thought to be force transmitted from the
center of the impact to the renal parenchyma.
• In injuries from rapid deceleration, the kidney
moves upward or downward, causing sudden
stretch on the renal pedicle and sometimes
complete or partial avulsion.

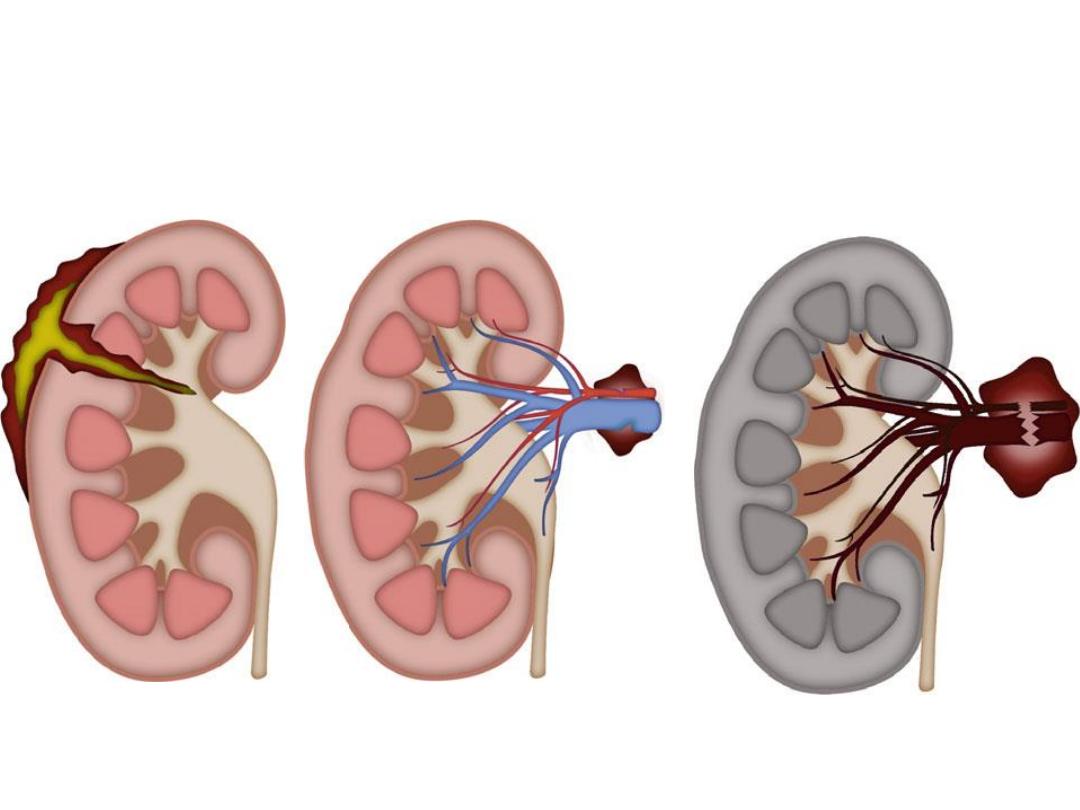
• Pathologic classification of renal injuries is as follows:
Grade I
—microscopic or gross hematuria; normal findings
on radiographic studies; contusion or contained
subcapsular hematoma without parenchymal
laceration.
Grade
II
—nonexpanding, confined perirenal hematoma
or cortical lacerat
ion less than 1 cm deep without
urinary extravasation.
Grade III
—parenchymal laceration extending more than 1
cm into the cortex without urinary extravasation.

Grade IV
—parenchymal laceration extending
through the corticomedullary junction and
into the collecting system.Maine renal artery
or veine injury with contained hemorrhage.
• Grade V
—completely shattered kidney or
avulsion of renal hilum and devascularizing
the kidney.
• B. LATE PATHOLOGIC FINDINGS:
1. Urinoma.
2. Hydronephrosis.
3. Arteriovenous fistula.
4. Renal vascular hypertension.

Clinical Findings & Indications for
Studies
• Microscopic or gross hematuria following trauma
to the abdomen indicates injury to the urinary
tract.
• The degree of renal injury does not correspond to
the degree of hematuria, since gross hematuria
may occur in minor renal trauma and only mild
hematuria in major trauma.
• However, not all adult patients sustaining blunt
trauma require full imaging evaluation of the
kidney.

INDICATIONS FOR RENAL IMAGING
• 1-All blunt trauma patients with groos
hematuria.
• 2-Microscopic hematuria with shock(systolic
BP less than 90mmhg any time during
evaluation &resuscitation).
• 3-Penetrating injuries with any degree of
hematuria.
• 4-Hematuria in pediatric patients(younger
than 18) due to sustaining blunt renal trauma.

• Symptoms:
Pain may be localized to one flank
area or over the abdomen.
• Retroperitoneal bleeding may cause abdominal
distention, ileus, nausea and vomiting.
• Sings:
Initially, shock or signs of a large loss of
blood from heavy retroperitoneal bleeding may
be noted.
• Ecchymosis in the flank or upper quadrants of the
abdomen.

• Diffuse abdominal tenderness may be found
on palpation; an “acute abdomen” usually
indicates free blood in the peritoneal cavity.
• A palpable mass may represent a large
retroperitoneal hematoma or perhaps urinary
extravasation.
• The abdomen may be distended and bowel
sounds absent.

• LABORATORY FINDINGS:
• Microscopic or gross hematuria is usually
present.
• The hematocrit may be normal initially, but a
drop may be found when serial studies are
done.
• This finding represents persistent
retroperitoneal bleeding and development of
a large retroperitoneal hematoma.

STAGING AND X-RAY FINDINGS
• Staging begins with an abdominal CT scan, the
most direct and effective means of staging renal
injuries.
• This noninvasive technique clearly defines
parenchymal lacerations and urinary
extravasation, shows the extent of the
retroperitoneal hematoma, identifies nonviable
tissue, and outlines injuries to surrounding
organs such as the pancreas, spleen, liver, and
bowel.

• If CT is not available, an intravenous
pyelogram can be obtained.
• Arteriography defines major arterial and
parenchymal injuries when previous studies
have not fully done.
• Arterial thrombosis and avulsion of the renal
pedicle are best diagnosed by arteriography
and are likely when the kidney is not
visualized on imaging studies.

• The major causes of nonvisualization on an
excretory urogram are total pedicle avulsion,
arterial thrombosis, severe contusion causing
vascular spasm, and absence of the kidney
(either congenital or from operation).
• Radionuclide renal scans have been used in
staging renal trauma. However, in emergency
management, this technique is less sensitive
than arteriography or CT.

LATE COMPLICATIONS
• 1-Hypertension.
• 2-hydronephrosis.
• 3-arteriovenous fistula.
• 4-calculus formation.
• 5-pyelonephritis.
• Careful monitoring of blood pressure for
several months is necessary to watch for
hypertension.

• At 3–6 months, a follow-up excretory urogram
or CT scan should be obtained to be certain
that perinephric scarring has not caused
hydronephrosis or vascular compromise; renal
atrophy may occur from vascular compromise
and is detected by follow-up urography.
• Heavy late bleeding may occur 1–4 weeks
after injury.

TREATMENT
A.EMERGENCY MEASURES:
• Treatment of shock and hemorrhage,
complete resuscitation, and evaluation of
associated injuries.
B. SURGICAL MEASURES:
• 1. Blunt injuries:injuries
—Minor renal
injuries from blunt trauma account for 85% of
cases and do not usually require operation.

• Bleeding stops spontaneously with bed rest
and hydration.
• Grade IV&V injuries more often require
surgical exploration,but even these high grade
injuries can be managed without renal
operation if carefully staged &selected.
• Aggressive preoperative staging allows
complete definition of injury before operation.
OPERATIVE MANAGEMENT
• Absolute indications for renal exploration include:
1-Evidence of persistent renal bleeding.
2-Expanding perirenal hematoma.
3-Pulsatile perirenal hematoma.
Relative indications include:
1-Urinary extravasation.
2-Nonviable tissue.
3-Delayed diagnosis of arterial injuryor segmental
arterial injury.
4-Incomplete staging.

• 2. Penetrating injuries
:Penetrating injuries
should be surgically explored. A rare exception
to this rule is when staging has been complete
and only minor parenchymal injury, with no
urinary extravasation, is noted.
• In 80% of cases of penetrating injury,
associated organ injury requires operation;
thus, renal exploration is only an extension of
this procedure.

C. TREATMENT OF COMPLICATIONS
• Retroperitoneal urinoma or perinephric abscess
demand prompt surgical drainage. Malignant
hypertension requires vascular repair or
nephrectomy.
• Hydronephrosis may require surgical correction
or nephrectomy.
• Prognosis:
With careful follow-up, most renal
injuries have an excellent prognosis, with
spontaneous healing and return of renal function.

INJURIES TO THE URETER
• Etiology:
1-
Large pelvic masses (benign or malignant) may
displace the ureter laterally and engulf it in
reactive fibrosis.
2-
Inflammatory pelvic disorders may involve the
ureter in a similar way.
3-
Extensive carcinoma of the colon may invade
areas outside the colon wall and directly
involve the ureter.

4-Devascularization may occur with extensive
pelvic lymph node dissections or after
radiation therapy to the pelvis for pelvic
cancer.
5-Endoscopic manipulation of a ureteral calculus
with a stone basket or ureteroscope may
result in ureteral perforation or avulsion.
6-Surgical injury:hysterectomy was responsible
for majority of surgical ureteric injuries(54%).

• Pathogenesis & Pathology:
The ureter may be inadvertently ligated and cut
during difficult pelvic surgery. In such cases,
sepsis and severe renal damage usually occur
postoperatively.
• If a partially divided ureter is unrecognized at
operation, urinary subsequent buildup of a large
urinoma will ensue, which usually leads to
ureterovaginal or ureterocutaneous fistula
formation.
• Intraperitoneal extravasation of urine can also
occur, causing ileus and peritonitis.
• After partial transection of the ureter, some
degree of stenosis and reactive fibrosis
develops, with concomitant mild to moderate
hydronephrosis.

GRADING OF URETERIC INJURY
• Grade I-contusion or hematoma without
devascularizasion.
• Grade II-laceration(less than50%transection).
• Grade III-laceration(more
than50%transection).
• Grade IV-laceration(complete transection with
less than 2cm devascularization.
• Grade V-laceration(avulsion with more than
2cm devascularization.

Clinical Findings
• A. SYMPTOMS:
If the ureter has been completely
or partially ligated during operation, the
postoperative course is usually marked by fever
of 38.3°C–38.8°C (101°F–102°F) as well as flank
and lower quadrant pain.
• Such patients often experience paralytic ileus
with nausea and vomiting.
• Ureterovaginl or cutaneous fistula develops, it
usually does so within the first 10 postoperative
days.

• B. SIGNS:
severe flank pain and abdominal pain
with nausea and vomiting early in the
postoperative course and with associated ileus.
• Signs and symptoms of acute peritonitis may be
present if there is urinary extravasation into the
peritoneal cavity.
• Watery discharge from the wound or vagina may
be identified as urine by determining the
creatinine concentration of a small sample.or by
injection of indogo carmine I.V.

C. LABORATORY FINDINGS:
Ureteral injury from
external violence is manifested by microscopic
hematuria in 90% of cases.
• D. IMAGING FINDINGS:
Diagnosis is by
excretory urography or delayed abdominal
spiral CT scan. A plain film of the abdomen
may demonstrate a large area of increased
density in the pelvis or in an area of
retroperitoneum where injury is suspected.

• In acute injury from external violence, the
excretory urogram usually appears normal.
• Retrograde ureterography demonstrates the
exact site of obstruction or extravasation.
E. ULTRASONOGRAPHY:
Ultrasonography
outlines hydroureter or urinary extravasation
as it develops into a urinoma and is perhaps
the best means of ruling out ureteral injury in
the early postoperative period.

Differential Diagnosis:
*Postoperative bowel obstruction and
peritonitis.
*
Deep wound infection must be considered
postoperatively in patients with fever, ileus,
and localized tenderness.
*
Acute pyelonephritis in the early postoperative
period may also result in findings similar to
those of ureteral injury.

TREATMENT
• The best opportunity for successful repair is in
the operating room.
• If the injury is not recognized until 7–10 days
after the event and no infection, abscess, or
other complications exist, immediate
reexploration and repair are indicated.
• Proximal urinary drainage by percutaneous
nephrostomy or formal nephrostomy should be
considered if the injury is recognized late or if the
patient has significant complications that make
immediate reconstruction unsatisfactory.

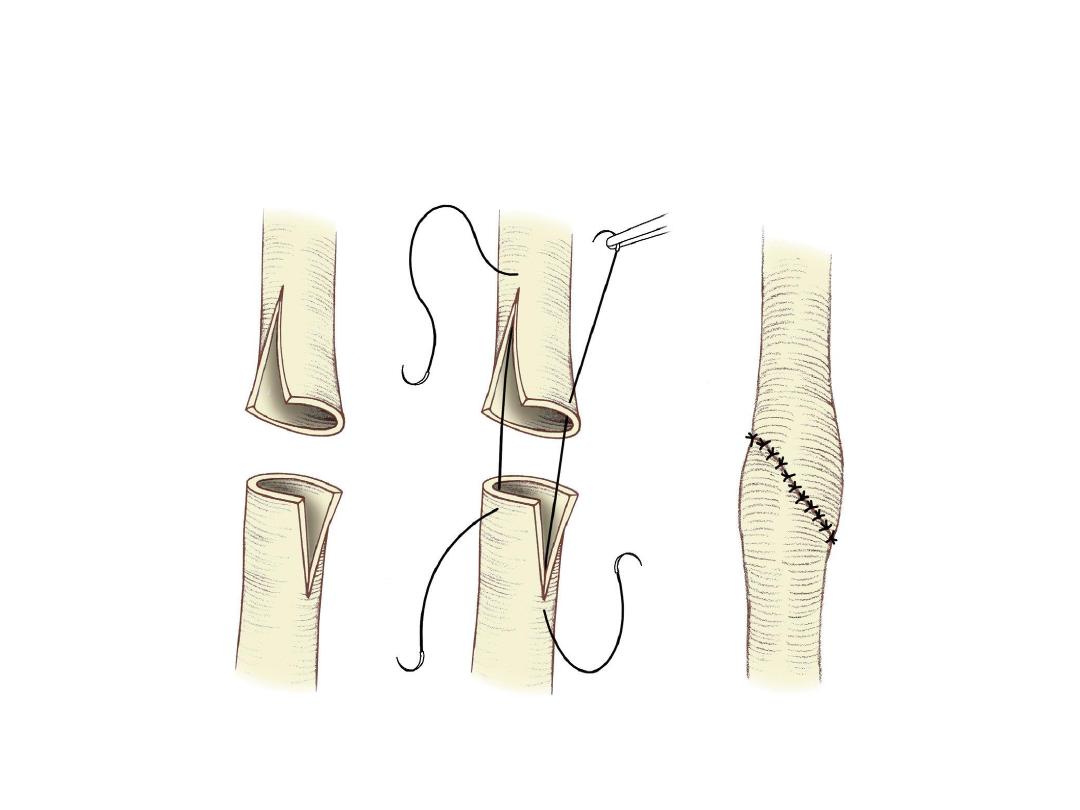
• The goals of ureteral repair are:
1-Achieve complete debridement.
2- Tension-free.
3- Spatulated anastomosis, watertight closure,
ureteral stenting (in selected cases).
4- retroperitoneal drainage.
*Ureteral contusion due to external trauma is
treated by either internal stenting or
ureteroureterostomy.
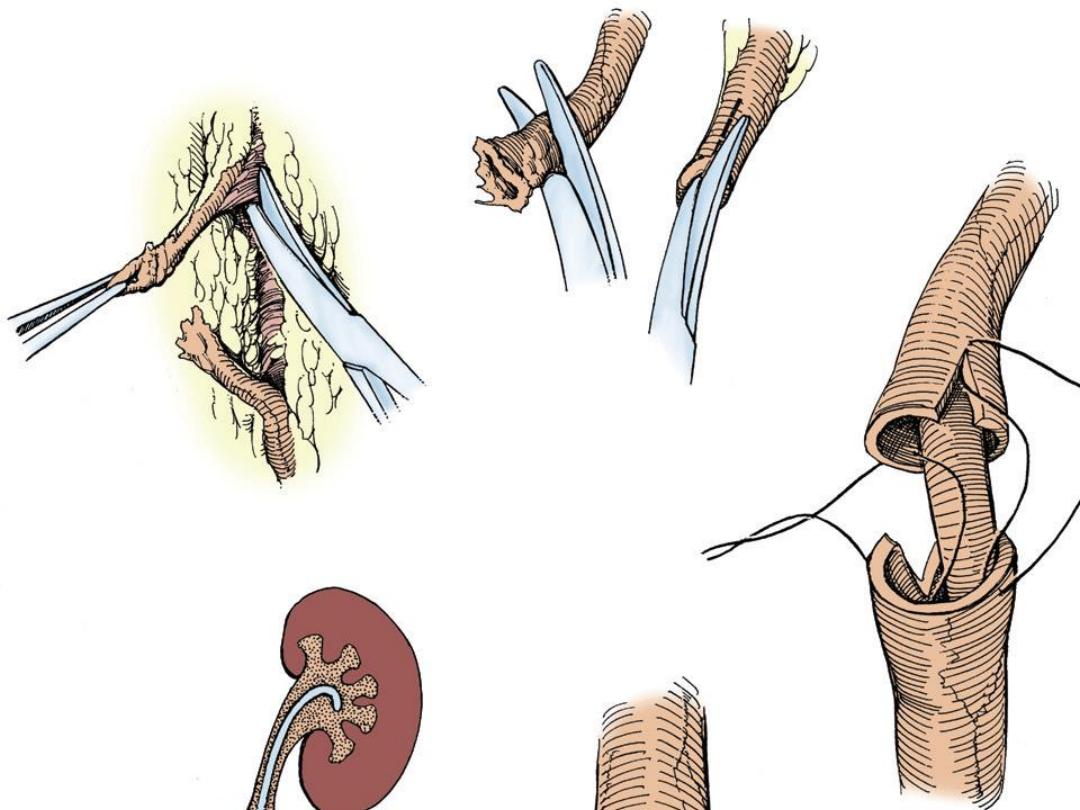
• UPPER URETERAL INJURIES:
• 1-
ureteroureterostomy.
• 2-
bowel replacement of the ureter.
• 3-
autotransplantation of the kidney.
• MIDURETERAL INJURIES:
• 1-
ureteroureterostomy.
• 2-
transureteroureterostomy.

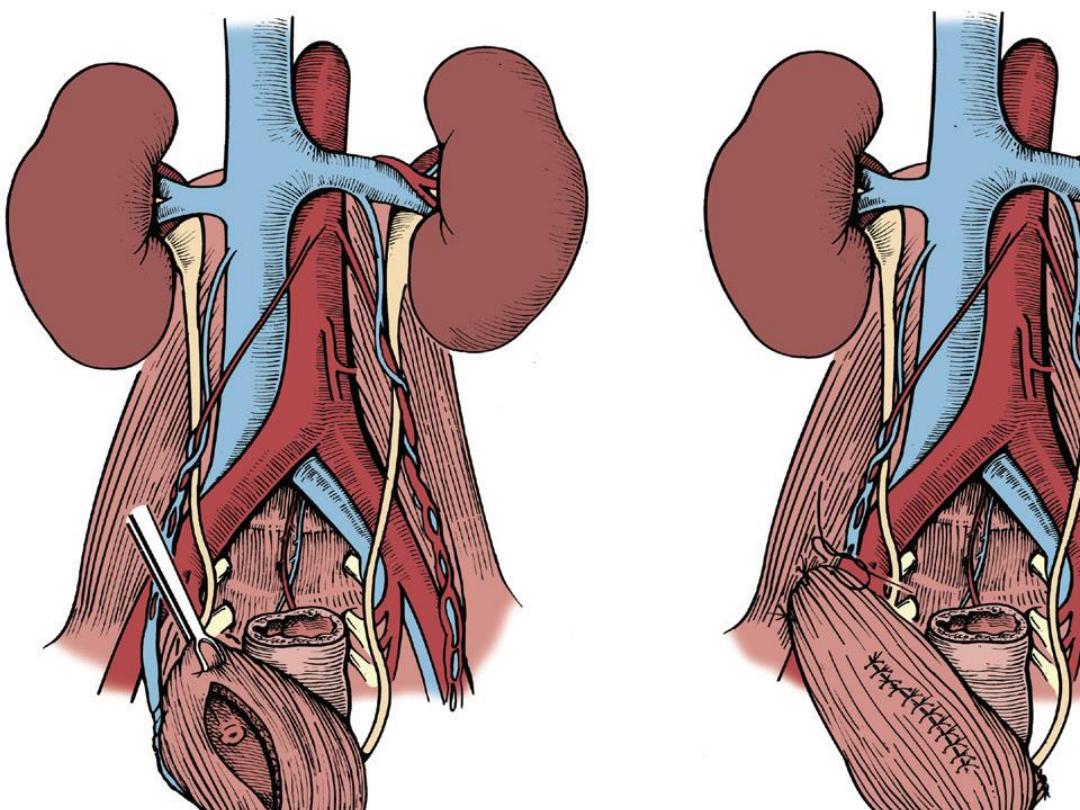
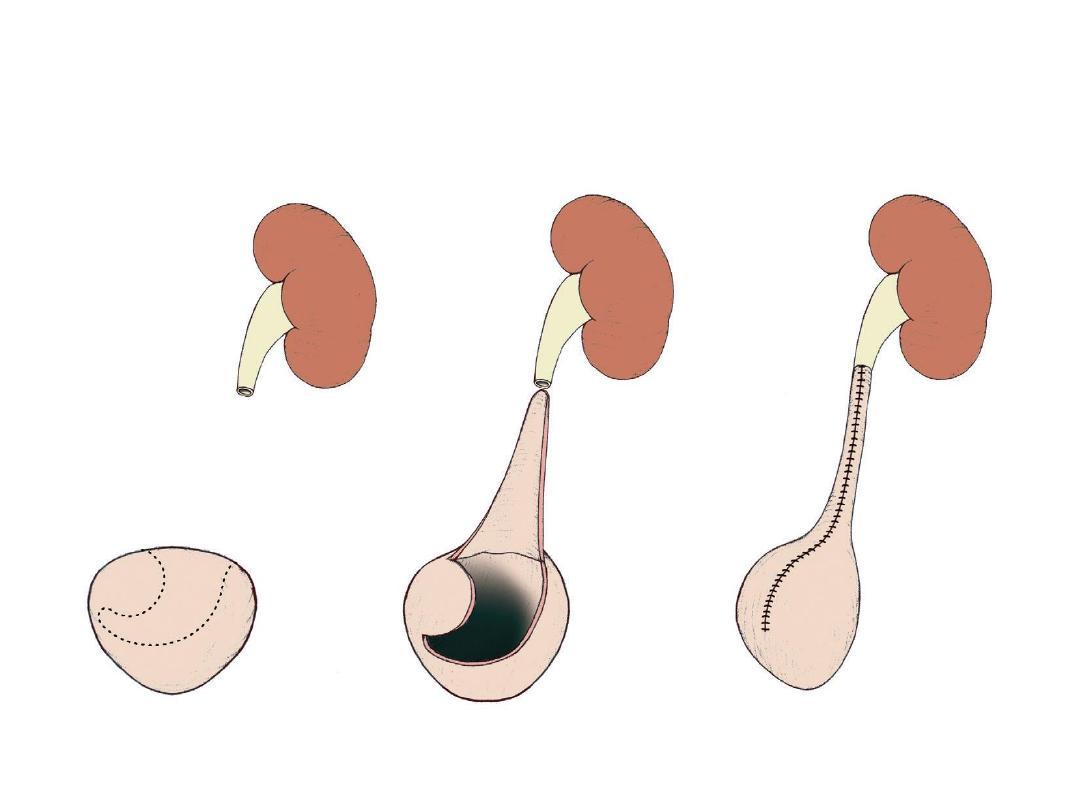
• LOWER URETERAL INJURIES:
• 1-
Ureteroneocystostomy reimplantation into
the bladder.
• 2.
psoas bladder hitch or boari flap.
• 3-
Transureteroureterostomy.
• The prognosis for ureteral injury is excellent if
the diagnosis is made early and prompt
corrective surgery is done.


A B C
D E F