
Renal parenchymal neo Plasm:
LEARNING OBJECTIVES
At the end of this clerkship, the learner will be able to:
1. Classify Renal tumors.
2. Describe the proper technique for Diagnosis of renal masses.
3. Identify four risk factors that increase the likelihood of finding malignancy during evaluation c Renal
tumors.
4. Explain the significance of findings o frenal cell carcinoma during evaluation of renal mass.
5. Contrast the evaluation and management of renal masses.
6. Identify the causes of secondary renal masses .
About Kidney Cancer
According to the American Cancer Society, an estimated 58.240 people in the United States will be
diagnosed with kidney cancer about 13.0-40 people will die from this disease. As with all cancers, early
diagnosis of kidney cancer dramatically improves the chance for survival.
Although the prognosis is relatively poor for kidney cancer that is advanced (metastasized), promising
new treatments for kidney cancer are improving the outlook for patients.
ADENOCARCINOMA OF THE KIDNEY (RCC):
RCC accounts for roughly 2.8°o of adult cancers and constitutes approximately 85% of all primary'
malignant renal tumors. RCC occurs most commonly in the fifth to sixth decade and has a male-female
ratio of 2:1 . (Table 1).
Table 1 ; Etiology and environmental risk factors for renal tumors:
Established
• Tobacco exposure
• Obesity
• Hypertension
Putative
• Lead compounds
• Various chemicals (e.g., aromatic hydrocarbons) Trichloroethylene exposure
• Occupational exposure (metal, chemical, rubber, and printing industries)
• Asbestos or cadmium exposure Radiation therapy
• Dietary (high fat/protein and low fruits/vegetables)
Other Risk Factors:
von hippel-lindau disease ;
(cerebellar hemangioblastoma . retinal angiomata, and bilateral clear cell RCC.)
Hereditary papillary renal carcinoma; multiple (bilateral renal tumors with a papillary histologic
appearance)
Acquired cystic decease of the kidneys; is a well-recognized entity of multiple (bilateral cysts in the
native kidneys of uremic patients (>30 times higher).
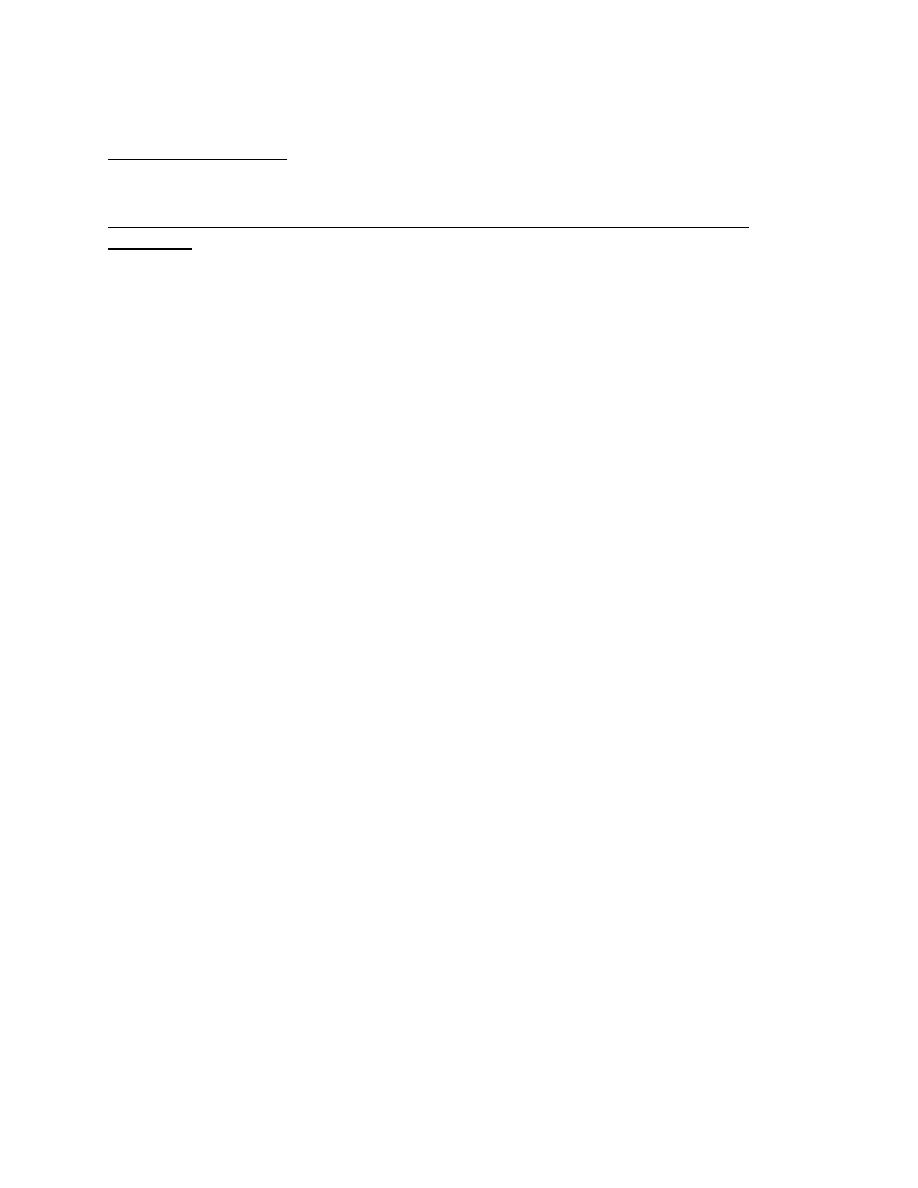
Pathology:
A. Clear cell renal cell carcinoma (RCC) with typical golden ye How color.
B. Low-power view of typical microscopic appearance of a low-grade clear cell RCC demonstrating a
delicate vascular network interspersed within homogeneous nests of cells with clear cytoplasm-Figure 1.
Clinical presentation of renal cell carcinoma
Incidental
( local tumor growth)
1. Hematuria
2. Flank pain
3. Abdominal mass
4. Perirenal hematoma
Metastasis
1. Persistent cough
2. Bone pain
3. Cervical lymphadenopathy
4. Constitutional symptoms (weight loss/fever/malaise)
5. Obstruction of Inferior Vena Cava
6. Bilateral lower extremity edema
7. Nonreducing or right sided varicocele
Paraneoplastic syndrome
1. Hypercalcemia
2. Hypertension
3. Polycythemia
4. Stauffer’s syndrome
Pathogenesis:
RCCs arc vascular tumors that tend to spread either by; direct invasion through the renal capsule into
perinephric fat and adjacent visceral structures or by direct extension into the renal vein. Approximately
25—30% of" patients have evidence of metastatic disease ill presentation. The most common site of
distant metastases is the lung.

STAGING OF RENAL CELL CARCINOMA:
• Stage I
Tumor within capsule
• Stage II
Tumor invasion of perinephric fat (confined to Gerota fascia)
• Stage III
Tumor involvement of regional lymph nodes and/or renal vein and cava.
Laboratory findings
In addition to the laboratory abnormalities associated with the various RCC paraneoplastic
syndrome, Anemia, hematuria, and elevated sedimentation rate are frequently observed.
Gross microscopic hematuria can be seen in up to 60% of patients presenting with RCC.
An elevated erythrocyte sedimentation rate is also commonly seen, with a reported incidence as
high as 75%.
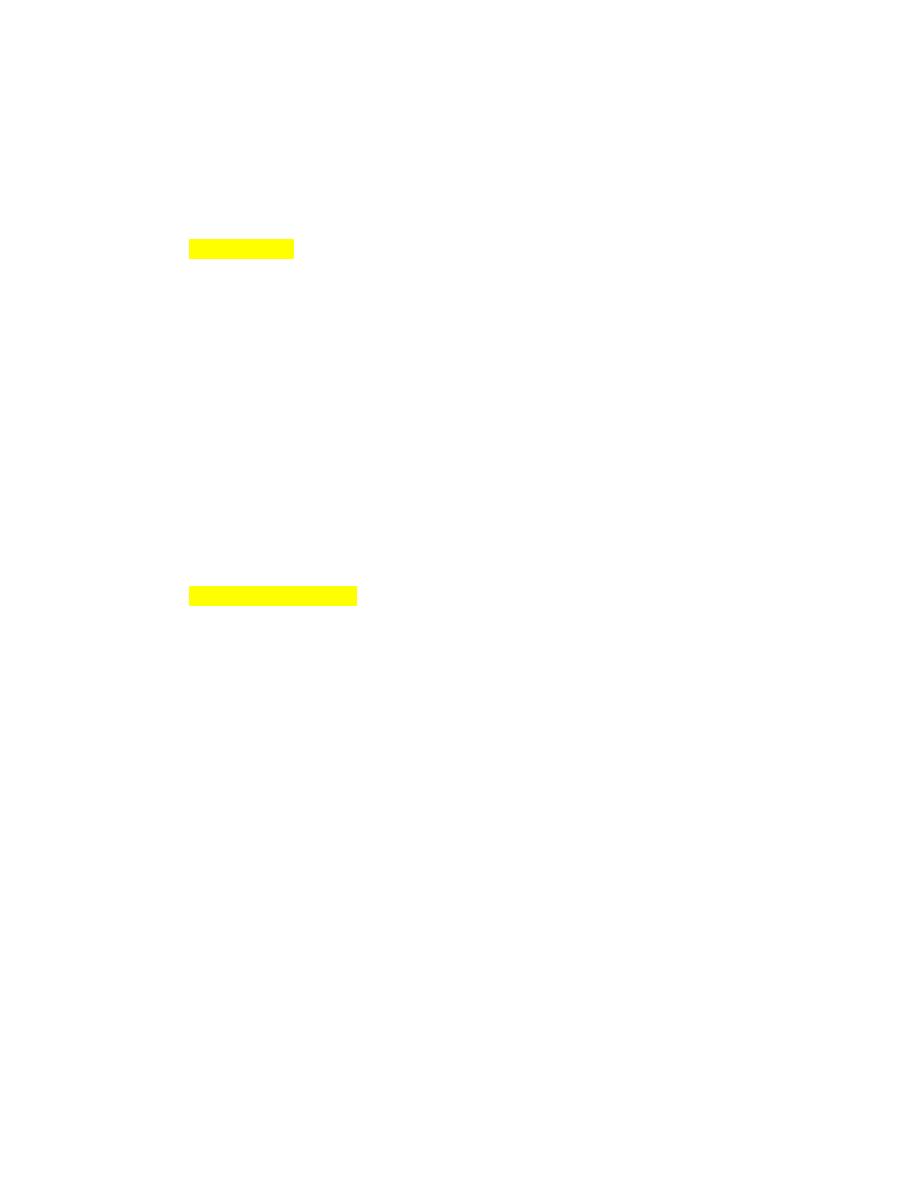
Radiological findings
• CT scanning remains the primary technique with which others must be compared. A typical
finding of RCC on CT is a mass that becomes enhanced with the use of intravenous contrast
media . (Figure 3).
• Ultrasonography ; It is approximately 98% accurate in distinguishing simple cysts from
solid lesions.
• Fine- needle aspiration ;
Primary indications for needle aspiration or biopsy o f a renal mass are when a renal abscess
or infected cyst is suspected. when RCC must be differentiated from metastatic malignant
disease or renal lymphoma.
Differential Diagnosis
the great majority of renal mas are simple cysts.
A renal abscess may be strongly suspected in a patient presenting with fever, flank pain, pyuria,
and leukocytosis, and an early needle aspiration and culture should be performed.
Other benign renal masses include granulomas and arteriovenous malformations, renal
lymphoma ,transitional cell carcinoma of the renal pelvis. Adrenal cancer, and metastatic
diseases (most commonly from lung or breast cancer primary).
1. Localized disease:
Surgically removal of the early-stage lesion remains the only potentially curative therapy
available for RCC patients.
Radical nephrectomy is the primary treatment for localized RCC.
Radical nephrectomy entails en bloc removal of the kidney and it’s enveloping fascia
(gerota’s) including the ipsilateral adrenal, proximal one-half of the ureter, and lymph nodes
up to the area of transection of renal vessels.

laparoscopic surgery
The recovery from a laparoscopic nephrectomy is remarkably swift with many patients back
to full activities within 3 weeks. They also suffer a lot less from the smaller sears than the
conventional surgical sear.
Nephron-sparing surgery
Considered for patient with:
1- A localized tumor less than 4 cm in diameter.
2- A anatomical or functional solitary kidney and patients with a contralateral kidney
affected by condition that might impair renal function in future.
it involves partial nephrectomy with preservation of as much functioning kidney tissue as
possible.
Minimal invasive surgery:
Used in patient who are not candidates for surgery.
A. Ablation
Kidney tumors he removed (ablated) with intense heat or cold, in which special inserted
needles as inserted through the skin, guided by imaging from a CT scan and ultrasound.
B. Angio-embolization : embolization of the renal artery resulting in reduction of tumor size.
2. Disseminated disease
Approximately 30% of patients with RCC will present with advanced disease. Metastatic RCC
has a natural history that is typically aggressive and rapidly progressive with 5 years survival
rates typically less than 10%.
A. Surgery:
For managing patients with severe hemorrhage or unremitting pain.
Patients presenting with a solitary metastatic site! particularly in the lung that is amenable
to surgical resection may be candidates tor combined nephrectomy and removal of the
metastatic foci.
Nephrectomy in the- presence of metastatic disease (cytoreductive nephrectomy) before
immunotherapy.
B. Radiation therapy :
Effective palliation of metastatic disease to the brain, bone, and lungs is reported in up to
two thirds of patients.
C. Biologic response modifiers:
More recently, recombinant interferon alpha (IFN-α). Various doses and schedules of
interferon alpha (IFN-α) have demonstrated reproducible overall response rates of 10-15%
in advanced renal cancer.
TARGETED MOLECULAR AGENTS:
Antagonists of the Vascular Endothelial Growth Factor Pathway inhibition of
Mammalian Target of Rapamycin.
Prognosis:
5-year survival rates tor patients with stage T1 -T2 disease in the 80-100% range. with stage
T3 in the 50—60% range. Patients presenting with metastatic disease have a poorer
prognosis with only 10-32% 5-year survival rate.
Benign tumors:
Renal adenoma:
The adenoma is the most common benign renal parenchymal lesion. These are small,
well-differentiated glandular tumors of the renal cortex. They are typically asymptomatic
and usually identified incidentally.
Renal oncocytoma:
Renal oncocytoma has a spectrum of behavior ranging from benign to malignant. An
estimated 3-5% of renal tumors are oncocytomas. The diagnosis of oncocytomas
predominantly pathologic because there are no reliable distinguishing clinical
characteristics.
Angiomyolipoma ( Renal Hamartoma):
Angiomyolipoma is a rarer benign tumor of the kideny Angiomyolipomas are found in
approximately 45-80% of patients with tuberous sclerosis an are typically bilateral and
asymptomatic. Patients with lesions >4 cm with moderate or severe symptoms (bleeding or
pain) should undergo renal-sparing surgery or renal arterial embolization.
Secondary renal tumors:
The kidney is a frequent site for metastatic spread of both solid and hematologic tumors.
The most frequent primary site of cancer was lung (20% followed by breast 12% → stomach
11% → and renal 9%). invasion by lymphoma to be 0.5-7% with the rates of Hodgkin’s and
non-Hodgkin’s lymphoma distributed equally.