D R . M O H A N N E D H U S S A M A L K U M A I T
A S S I S T A N T P R O F E S S O R O F U R O L O G Y
T I K R I T C O L L E G E O F M E D I C I N E
5
T H
Y E A R
Incontinence

Definition
Urinary incontinence (UI) is the complaint of any
involuntary leakage of urine.1 It results from a failure
to store urine during the filling phase of the bladder
due to abnormality of bladder smooth muscle or the
urethral sphincter. Urine loss is either urethral or
extra-urethral (secondary to anatomical abnormalities
including ectopic ureters, rectovesical or vesicovaginal
fistulae).
.
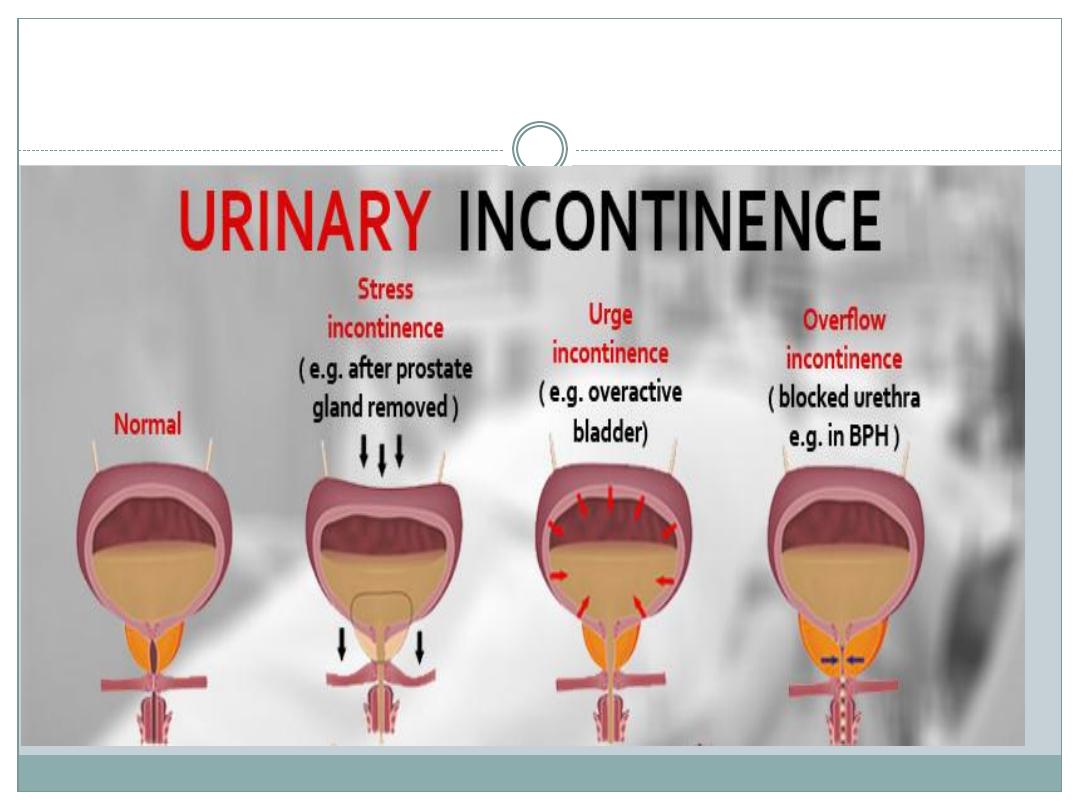
Classification
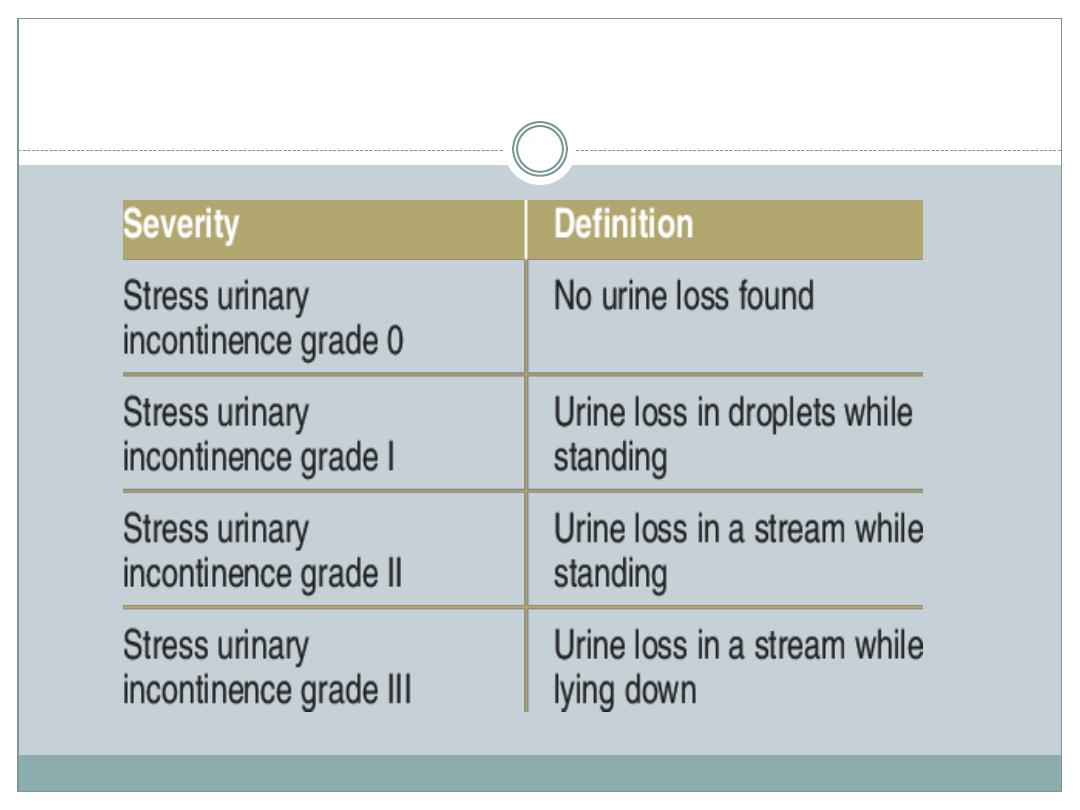
Stress urinary incontinence (SUI) is involuntary urinary
leakage on effort, exertion, sneezing, or coughing, due to
hypermobility of the bladder base, pelvic floor, and/or
intrinsic urethral sphincter deficiencies.
Type 0 €”report of urinary incontinence, but without
clinical signs.
Type I €”leakage that occurs during stress with <2cm
descent of the bladder base below the upper border of the
symphysis pubis.
Type II €”leakage on stress accompanied by marked
bladder base descent (>2cm) that occurs only during
stress (IIa) or is permanently present (IIb).
Type III €”bladder neck and proximal urethra are
already open at rest (with or without descent). Also
known as intrinsic sphincter deficiency (ISD).
Urge urinary incontinence (UUI) is involuntary urine leakage
accompanied by, or immediately preceded by a sudden, strong
desire to void (urgency). It is a component of the overactive bladder
syndrome .
Overflow incontinence is leakage of urine when the bladder is
abnormally distended with large residual volumes. Typically, men
present with chronic urinary retention and dribbling incontinence.
This can lead to back pressure on the kidneys and renal failure in
30% of patients.
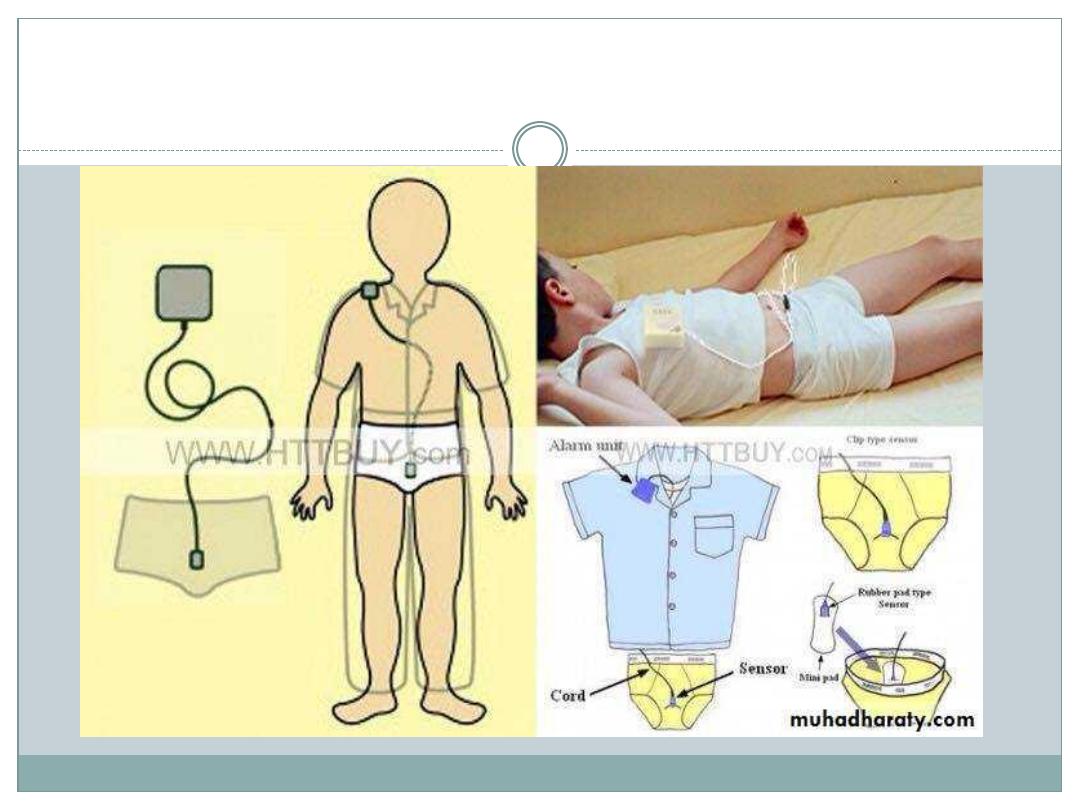
Nocturnal enuresis describes any involuntary loss of urine during
sleep. The prevalence in adults is 0.5%. Approximately 750,000
children over 7 years will regularly wet the bed. Childhood enuresis
can be further classified into primary types (never been dry for
longer than a 6-month period) or secondary (the re-emergence of
bed wetting after a period of being dry for at least 6 months).
Post-micturition dribble is the complaint of a dribbling loss of urine
that occurs after voiding. It predominantly affects males, and is due
to pooling of urine in the bulbous urethra after voiding .

Predisposing factors
gender (female > males)
race (Caucasian > Afro-Caribbean)
genetic predisposition
neurological disorders (spinal cord injury, stroke, MS,
Parkinson's disease)
anatomical disorders (vesicovaginal fistula, ectopic ureter,
urethral diverticulum)
childbirth
anomalies in collagen subtype
pelvic, perineal, and prostate surgery (radical hysterectomy;
radical prostatectomy; TURP) leading to pelvic muscle and
nerve injury
radical pelvic radiotherapy

Promoting factors
smoking (associated with chronic cough and raised
intra-abdominal pressure)
obesity
UTI
increased fluid intake
medications
poor nutrition
ageing
cognitive deficits
poor mobility

Physical examination
Women
Perform a pelvic examination in the supine, standing, and left
lateral position with a Sim's speculum. Ask the patient to cough
or strain, and inspect for vaginal wall prolapse (cystocele,
rectocele, enterocele), uterine or perineal descent, and urinary
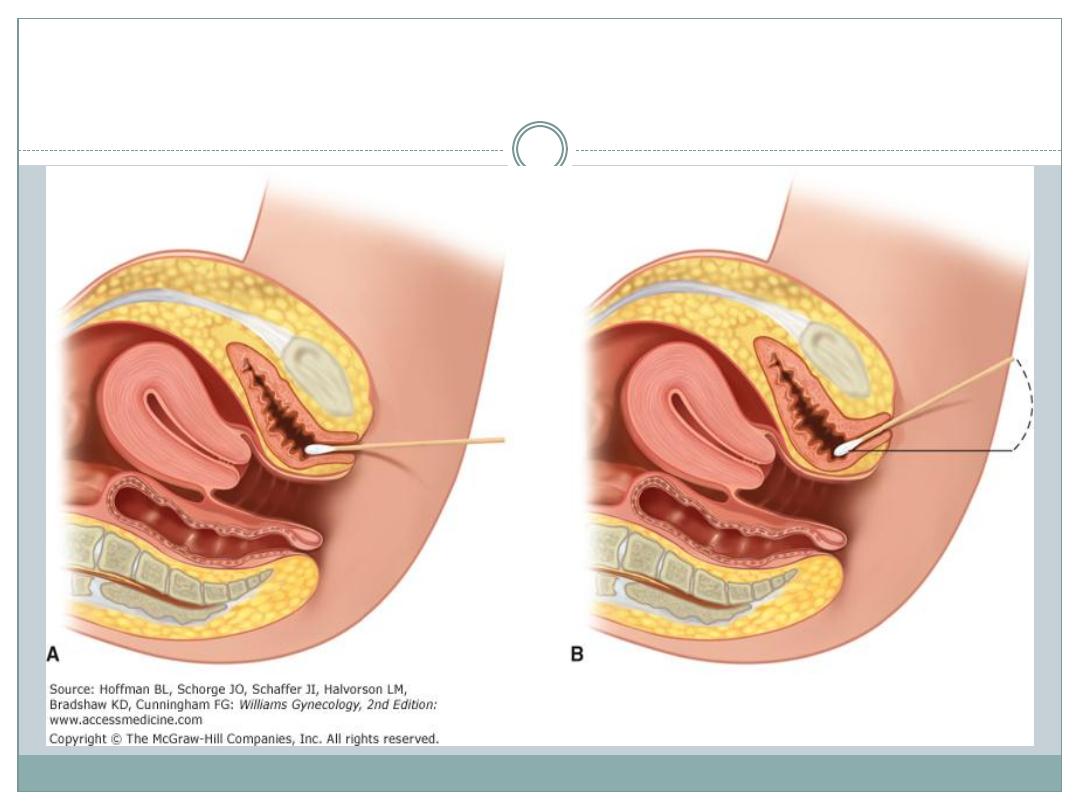
leakage (stress test). Urethral hypermobility is assessed with the
Q-tip test. A lubricated cotton-tipped applicator is introduced
through the urethra to bladder neck level. Hypermobility is
defined as a resting or straining angle of >30 آ
°
from horizontal.
Both sexes
Examine the abdomen for a palpable bladder (indicating urinary
retention). A neurological examination should include
assessment of anal tone and reflex, perineal sensation, and
lower limb function.

Investigation
Bladder diaries
: record the frequency and volume of
urine voided, incontinent episodes, pad usage, fluid intake, and
degree of urgency. Alternatively, pads can be weighed to
estimate urine loss (pad testing).
Urinalysis
: can exclude UTIs.
Blood tests
, X-ray imaging, cystoscopy: indicated for
persistent or severe symptoms, bladder pain, and voiding
difficulties.
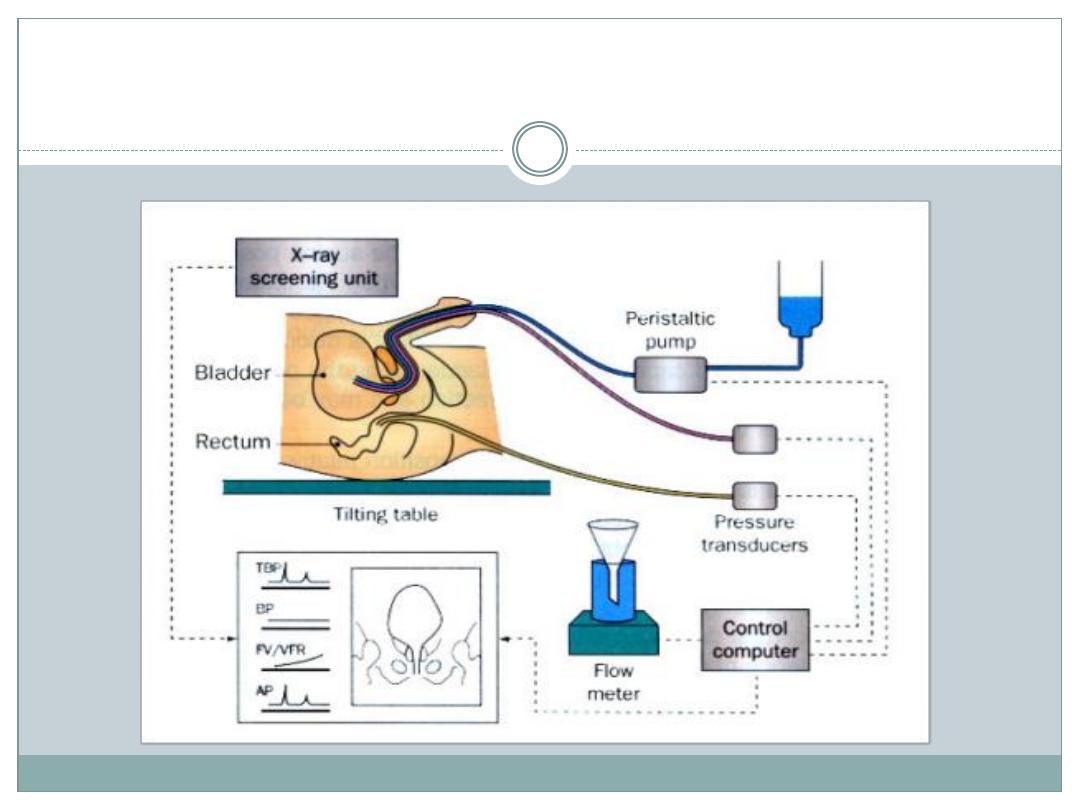
Screening tests
: flowmetry measures the pressure of
urine voided. A low rate indicates bladder outflow obstruction
or reduced bladder contractility. The volume of urine remaining
in the bladder after voiding (post-void residual) is also useful
(<50ml is normal; >200ml is abnormal;

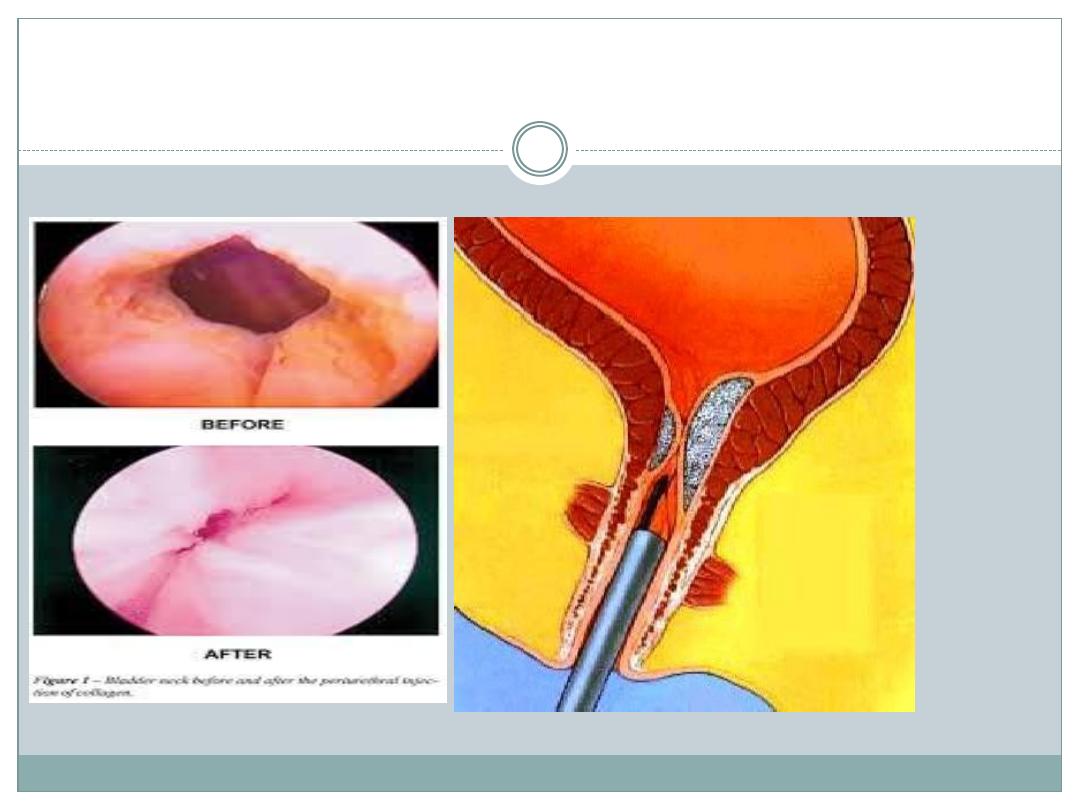
Treatment of sphincter weakness incontinence:
injection therapy
The injection of bulking materials into the bladder
neck and periurethral muscles is used to increase
outlet resistance. Bulking substances include silicone
polymers (Macroplastique); cross-linked bovine
collagen; Teflon; PTFE; and carbon coated zirconium
beads (Durasphere).
Indications
Stress incontinence secondary to demonstrable
intrinsic sphincter deficiency (ISD), with normal
bladder muscle function. Used in adults and children.
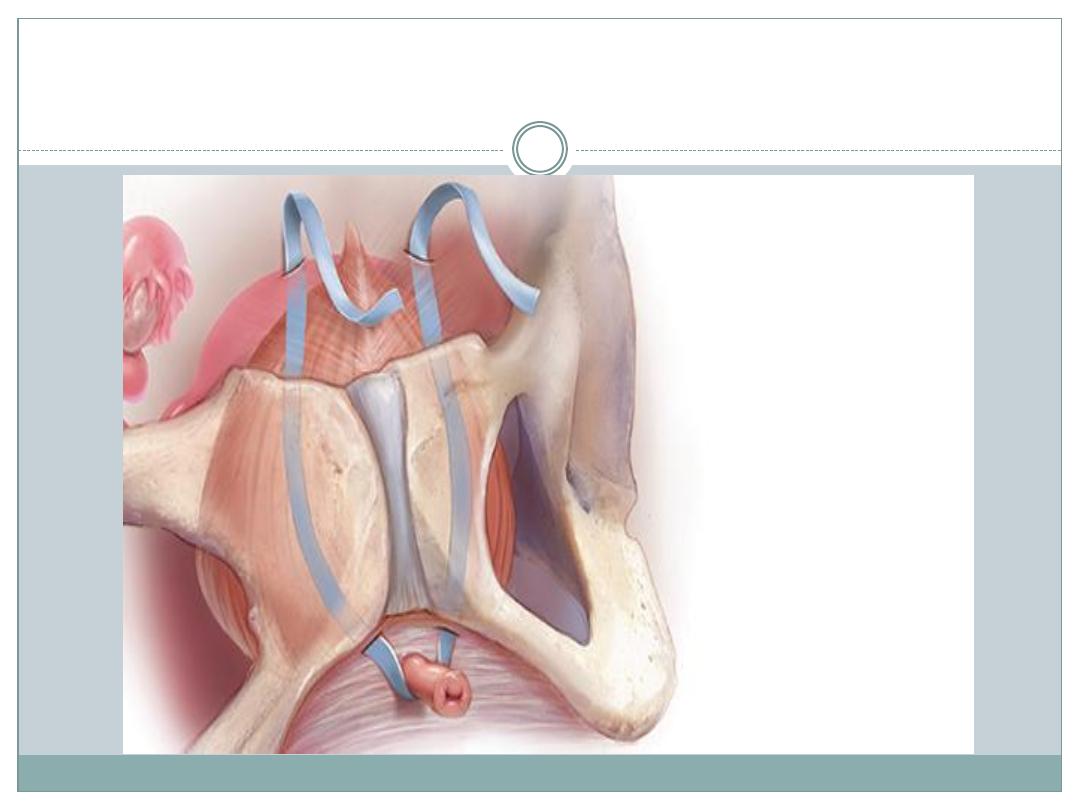
Treatment of sphincter weakness incontinence:
retropubic suspension
Retropubic suspension procedures are used to treat
female stress incontinence caused by urethral
hypermobility. The aim of surgery is to elevate and fix
the bladder neck and proximal urethra in a retropubic
position, to support the bladder neck, and regain
continence. Contraindicated in the presence of
significant intrinsic sphincter deficiency (ISD).

Treatment of sphincter weakness incontinence:
pubovaginal slings
Indications
Sling procedures are mainly used for female stress incontinence
associated with poor urethral function (type III or ISD), or when
previous surgical procedures have failed. Also used for incontinence
due to urethral damage (following radical pelvic surgery or
radiotherapy), and for neurological urethral dysfunction (e.g.
myelodysplasia) in both sexes. It is essential that urethral and bladder
function is evaluated prior to surgical repair.
Types of sling
Autologous ”rectus fascia, fascia lata (from the thigh), vaginal wall
slings.
Non-autologous ”allograft fascia lata from donated cadaveric tissue.
Synthetic ”monofilament polypropylene tape (TVT or tension-free
vaginal tape).

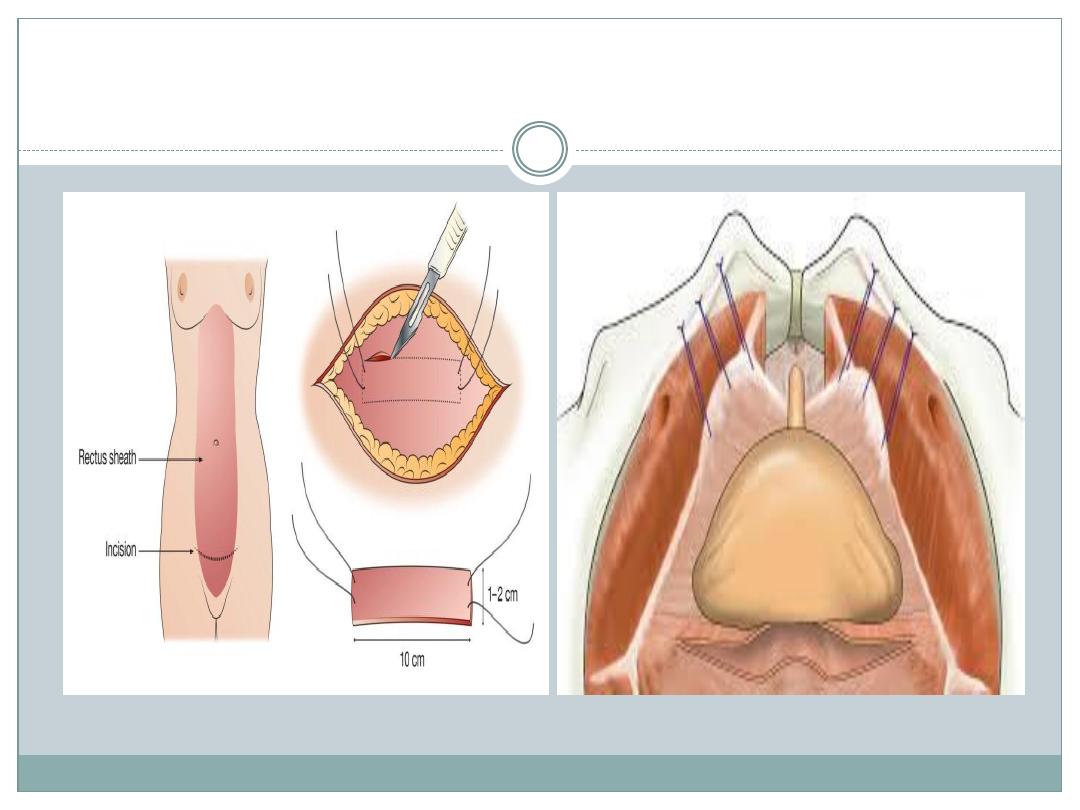
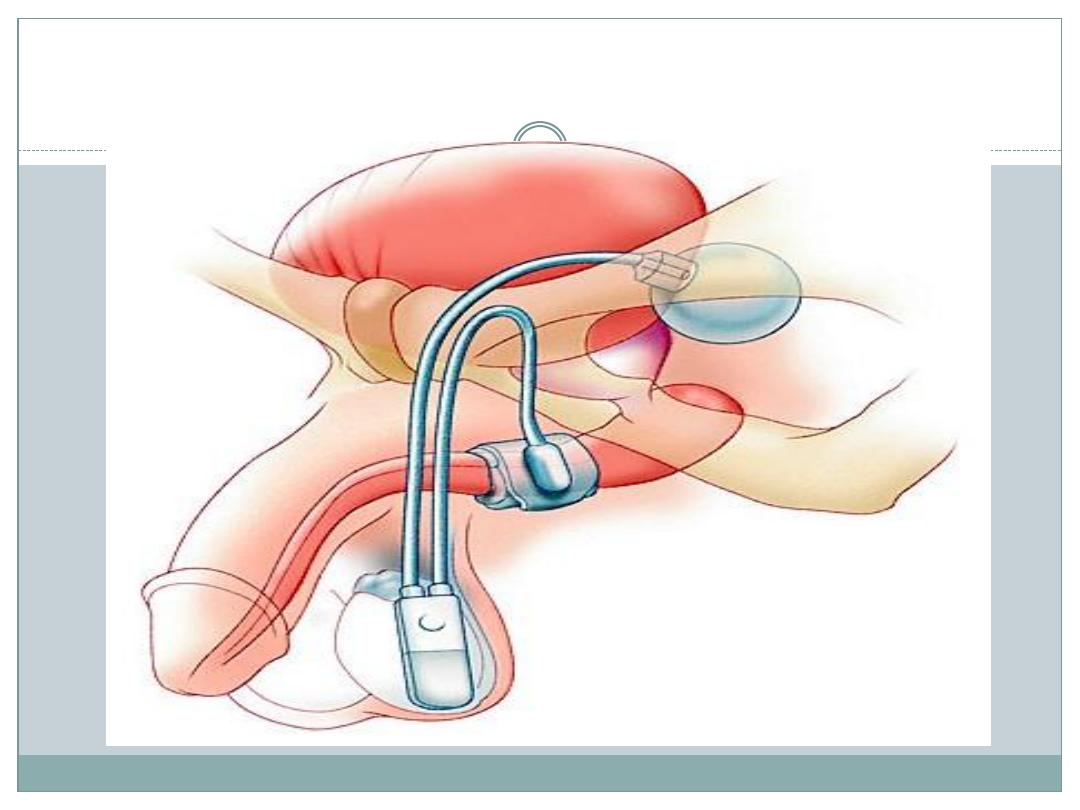
Treatment of sphincter weakness
incontinence: the artificial urinary sphincter
The artificial urinary sphincter consists of an
inflatable cuff placed, via a lower abdominal incision
(midline or Pfannenstiel), around the bladder neck
in both men or women or the bulbar urethra in men,
a pressure-regulating balloon placed
extraperitoneally, and an activating pump placed in
the scrotum or labia majora.

Incontinence secondary to urethral sphincter
deficiency in patients with normal bladder capacity
and compliance. In men, it is used for sphincter
damage due to prostatectomy (radical prostatectomy
for prostate cancer or TURP), pelvic radiotherapy,
pelvic fracture, and following urethral reconstruction.
In women it is used after other treatments for
incontinence have failed. It can be used for
neuropathic sphincter weakness (e.g. spinal cord
injury, spina bifida) if the incontinence is not due to
bladder overactivity.

Overactive bladder: conventional treatment
Definition
Overactive bladder (OAB) is a symptom syndrome
which includes urgency, with or without urge
incontinence, frequency, and nocturia. The symptoms
are usually caused by bladder (detrusor) overactivity,
but can be due to other forms of voiding dysfunction.
17% of the population >40 years old in Europe have
symptoms of OAB.
Conservative
Patient management involves a multidisciplinary team
approach (urologists, gynaecologists, continence nurse
specialists, physiotherapists, and community-based
health care workers). Treat any underlying causes
(urethral obstruction, bladder stones, spinal disease, or
tumour). TURP for bladder outlet obstruction due to
BPH can provide symptomatic relief in >66% of men.
Treatment of SUI component includes pelvic floor
exercises, biofeedback, and high-frequency electrical
stimulation (which strengthens the pelvic floor and
sphincter by increasing tone through sacral neural
feedback systems).

Behavioural modification
This involves modifying fluid intake, avoiding
stimulants (caffeine, alcohol), and bladder training for
urgency (delay micturition for increasing periods of
time by inhibiting the desire to void).

Medication
Anticholinergic drugs
act to inhibit bladder contractions and
increase capacity (oxybutynin, tolterodine; trospium; propiverine).
Oxybutynin also exerts a direct muscle effect and can be administered directly
into the bladder (intravesically) in patients performing intermittent
catheterization (5mg in 30ml normal saline 8 hourly after emptying the
bladder). Contraindications: closed angle glaucoma. Now the use of new m3
receptor blockers like solifenacin (vesicare) and darifenacin.
Tricyclic antidepressants
(imipramine) exert a direct relaxant
effect on bladder muscle as well as producing sympathomimetic and central
effects.
Desmopressin (DDAVP)
is a synthetic vasopressin analogue
which acts as an antidiuretic. It is used intranasally to alleviate nocturia in
adults. Oral DDAVP is effective for nocturnal polyuria.
Baclofen
is a GABA receptor agonist, which is used orally or via
intrathecal pump in patients with bladder dysfunction and limb spasticity.
Overactive bladder: options for failed
conventional therapy
Neuromodulation
Surgery
Auto-augmentation (detrusor myectomy):
Augmentation enterocystoplasty
Conduit diversion

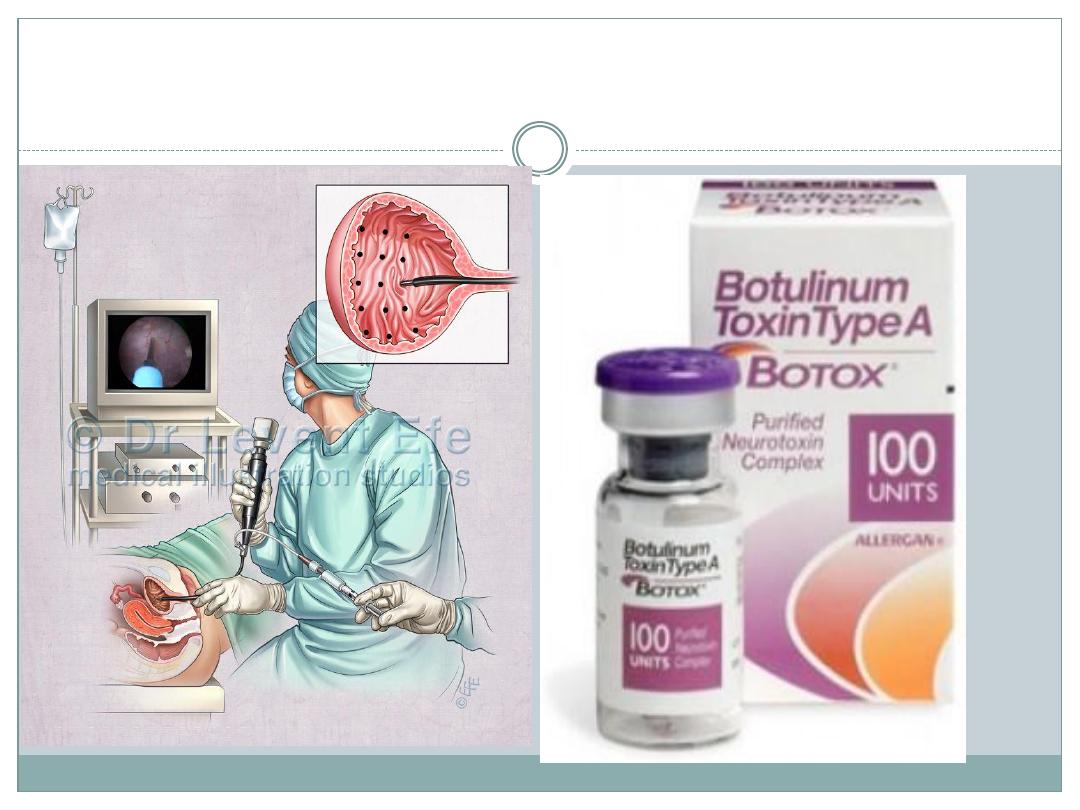
Intravesical pharmacotherapy
Botulinum toxin A (BTX-A) injection therapy acts by
inhibiting calcium-mediated release of ACh at the
neuromuscular junction, reducing muscle contractility.
It is used predominantly for neuropathic bladder
dysfunction, but increasingly is being used for failed
medical therapy of the OAB in non-neuropaths. It is
injected directly into detrusor muscle under
cystoscopic guidance