Psychogenic seizures
- These seizures also referred to (pseudo seizure) it is non- Epileptic seizure, and not
caused by abnormal neuronal discharge like real seizure.
- It could be a manifestation of a psychiatric disturbance such as conversion disorder,
somatization disorder, or factitious disorder.
- They are frequently mistaken for epileptic seizures and treated with anticonvulsant drugs
to which they are characteristically not response.
- They are most common in female than male.
- Some patients have both psychogenic and real seizures and the distinguish between
them is difficult.
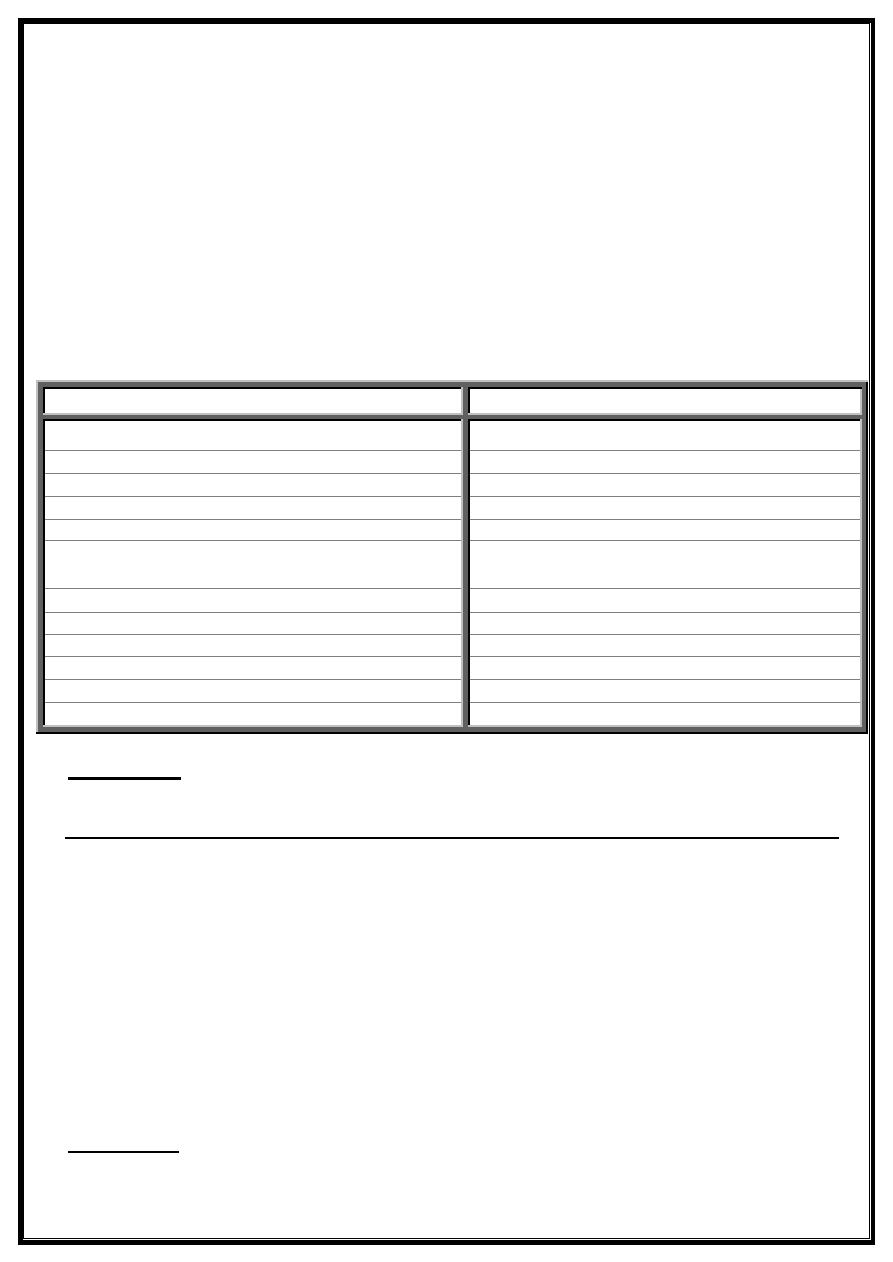
- This table will show the different between pseudo seizures and real one :
Treatments
It is depend on the under lying psychiatric disorder which is mostly conversional disorders
which had a good response to benzodiazepine group or mild dose of antidepressant drugs.
((Psychogenic loss of consciousness))
In this condition the patient, who was mostly a female fall to the ground like asleep state
without contraction of upper and lower limbs, and the condition mostly preceded by
psychological stress. Clinical examinations all were normal and when try to open the
eyes of patient he is resist opening and there is no reflex movement in response to any
painful stimuli.
This condition must be differentiated from other medical, neurological, endocrinological,
cardiovascular and all other organic problems which cause similar condition by history,
examination and laboratory investigations.
-So vital signs all were normal (pulse, pressure, temperature and breathing)
Cardiac, neurologic and all other examination is normal.
-Also all investigations were normal.
Treatments:
Is according to the underlying psychiatric disorder, mostly conversion.
Psychogenic
Epileptic
1- Always P.T.T by psychogenic stress.
1- Could occur without stress.
2- Always occur in awaked patient.
2- Usually occur at night during sleep.
3- There could be continuo's shouting.
3- Shouting only at the start of the fit.
4- There is a bizarred limbs movement.
4- Symmetrical limbs movements.
5- Continuo for minutes to hours.
5- Not more than 15 minutes.
6- No self-injury occurs.
6- tongue bite, fracture teeth, bruises, shoulder
dislocation could occurs.
wasshposhoulder
7- No urinary passing at all.
7- Urine pass could occur.
8- Patient can hearing the sound during the attack.
8- Patient can not hearing the sound.
9- Patient not amnestic for the attack.
9- Patient amnestic for the attack.
10- No post-ictaJ confusion or headache.
10- Headache and confusion could occur.
11- Planter post-ictally is down-going.
11- Planter reflex is up-going post -ictal.
12- EEG is normal during the attack and post-ictal.
12- EEG abnormal during and post-ictal.
Dr.Hassan M. Al jumaily
Neurologist