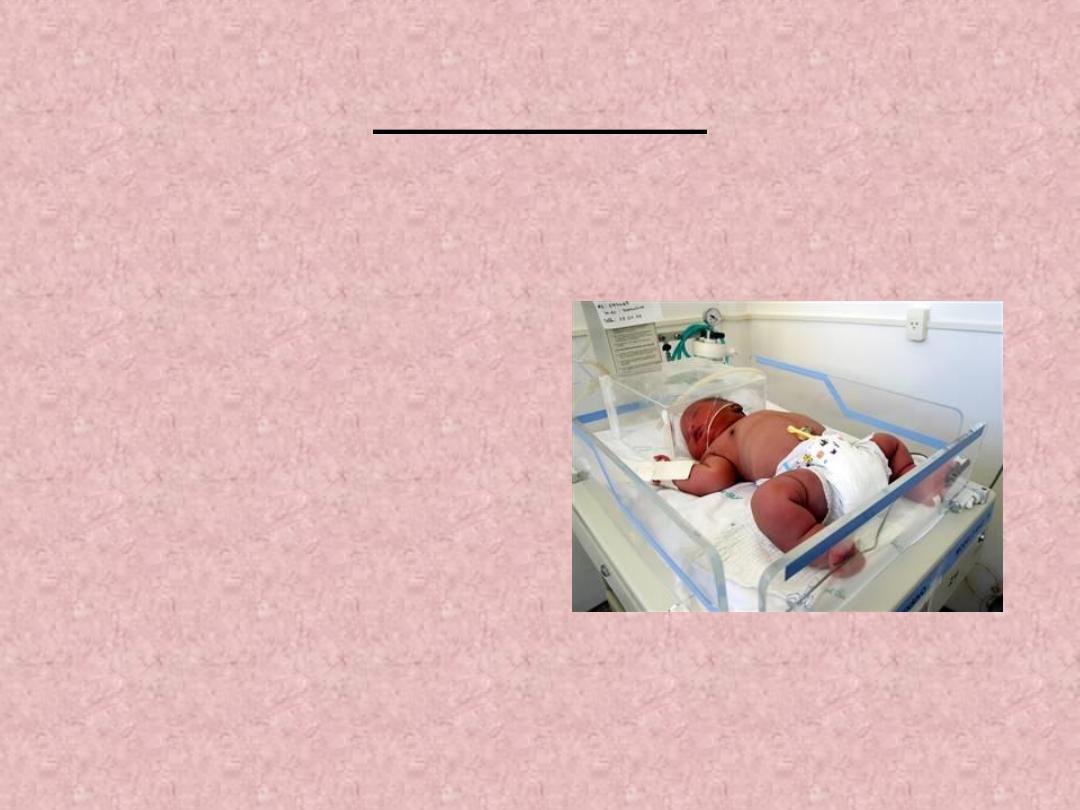
The Infant of a Diabetic
Mother
Dr.Prof. Alaa H.Alwan
TUCOM-2020
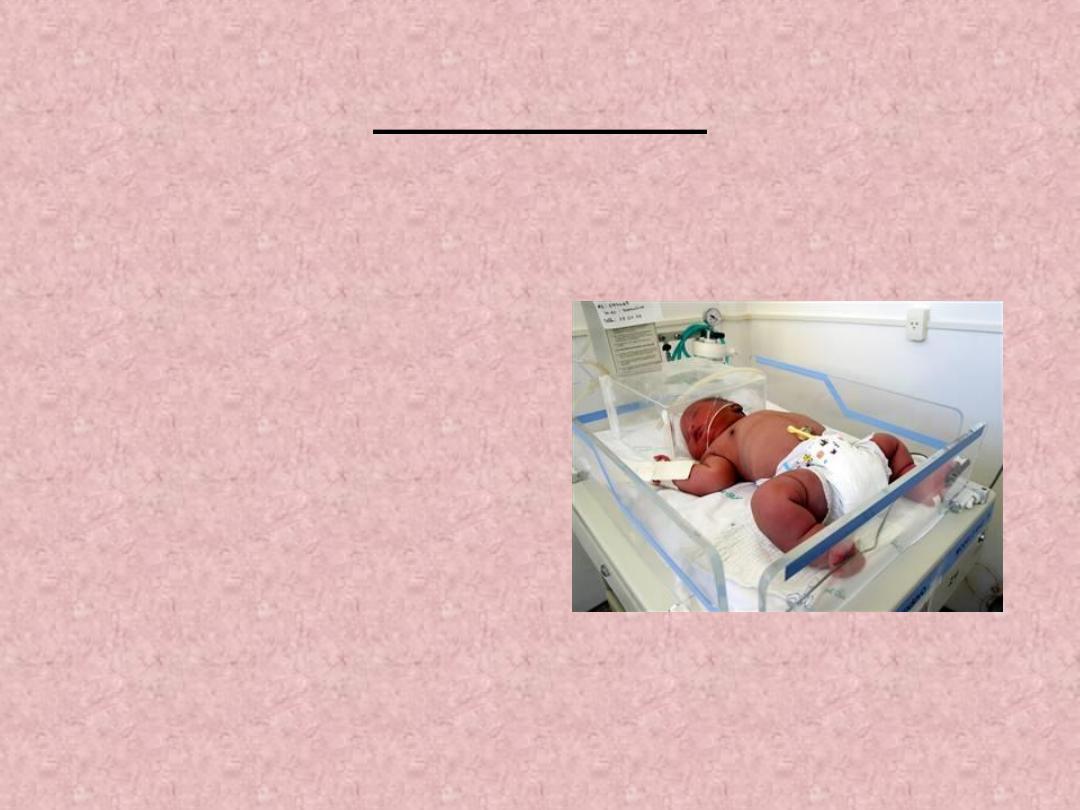
The Infant of a Diabetic Mother
• Is infant born to a mother with diabetes or
gestational diabetes, severity of the problem
depend on the severity of maternal diabetes.
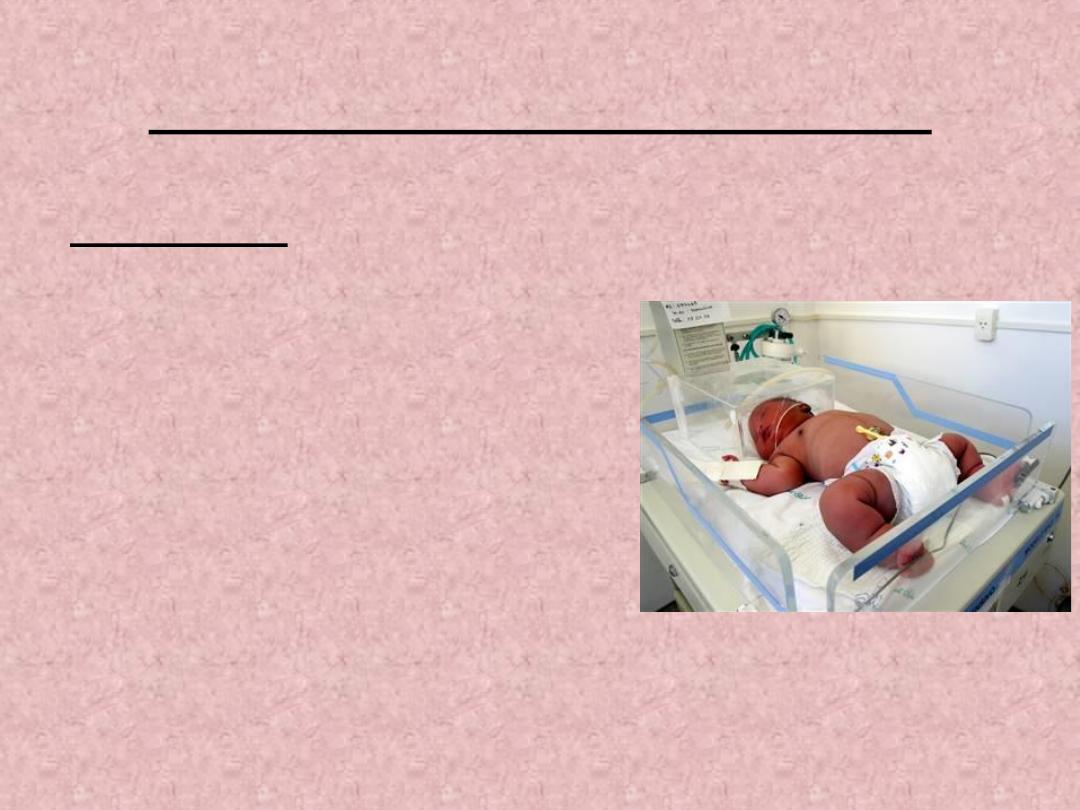
• Altered physiology: hyperinsulinemia in utero
secondary to decreased epinephrine and glucose
response result in the following in the infant:
Altered physiology
• Amount of body fat.
• Hypoglycemia can occur immediately or within
2
-
12
hours post delivery.
• IDM may symptomatic or not with blood glucose
below 20 mg/dl.
• Hypocalcemia: associated with prematurity, difficult
labor and or asphyxia at birth, can occur during first
24
-
48
h after birth.
• Birth trauma such as cephallhematom due to large
size of infant .
Altered physiology
cont…
• Hyperbilirubinemia: occur 48-72 h due to immature liver
and inability to conjugate bilirubin.
• Prematurity or SGA associated with placental
insufficiency.
• Respiratory problems may occur.
• Polycythemia: HCT more than 65% or Hb% 22gm/dl,
which the risk of thrombosis
, RDS,
hypoglycemia &
hypocalcemia.
• Congenital anomalies: (cardiac & skeletal).
• Infection
.
Diabetes Mellitus
A chronic metabolic disorder involving
complete or decreased insulin secretion
or other insulin dysfunction resulting in
increased serum glucose concentration.
Diagnostic criteria
• Family or mother history of DM.
• Determine gestational age.
• Blood studies:
• Blood glucose, HCT, Hb%, blood gases, bilirubin,
electrolytes.
• Clinical manifestations:
• Marcosomia, cardiomegaly, hepatomegaly,
abundent fatty, hair, vernix caseosa
• May SGA
Diabetes- ADA Classification
• Type 1: IDDM (Juvenile diabetes)- early onset, lack of insulin,
presence of antibodies against B-cells; insulin needed, ketoacidosis
seen.
• Type 2: NIDDM (Adult diabetes, Maturity onset)- older patients,
insulin resistance common, decreased insulin sensitivity, overweight
patients, significant genetic component.
• Gestational Diabetes : Carbohydrate intolerance with onset or
first recognition during pregnancy
Morbidities in Infants of Diabetic
Mothers
• Macrosomia
• Hypoglycemia
• RDS
• IUGR
• Hypocalcemia
• Hyperbilirubinemia
• Congenital Anomalies
• Polycythemia
• Hyper viscosity
• Cardiomyopathy
• Increased fetal death
• Postnatal problems
Macrosomia
• Common Definition: Infant
with Bwt >4000 grams and/or
Head Circumference & Length >
90
th
percentile .
• IDMs have increased fat cells and
fat cell hypertrophy.
• Excess non-fatty tissue in
shoulders and scapular areas.
Macrosomia
• ¼ th of insulin dependent mothers
have Macrosomic infants.
• Excess growth happens in 3
rd
trimester.
• GDM mothers have same
incidence of Macrosomic infants as
other diabetics.
Macrosomia- Complications
• Birth Injuries- Brachial Plexus injury,
Fracture Clavicle or Humerus, Facial
nerve injury, Cephalhematoma.
• Shoulder Dystocia (2-4 fold more)
• Hypoglycemia
• Increased risk for asphyxia
• Increased recurrence risk in mother.
Morbidities- Congenital
Anomalies
• Upto 4-fold increase in infants of IDDMs
• Malformations shown to occur before 8
th
week
of gestation.
• Etiology: not clear, ? Hyperglycemia. ? Glucose
as a teratogen.
Congenital Anomalies
• Many reported.
• Most common are CV, Musculo-Skeletal &
CNS.
• Incidence decreased with tight glucose control
in mothers.
Respiratory Distress Syndrome
• Increased risk of RDS in IDMs <37 weeks GA
• Possible insulin interference with surfactant composition
and delayed maturation of surfactant system
• Metabolic Complications
• Hypoglycemia
• Hypocalcemia
• Hypomagnesemia
Hypoglycemia
• Occurs in up to 25 % of IDMs.
• Half of hypoglycemia occurs in first 24 hours.
• Less likely when mother’s glucose tightly
controlled.
• May be asymptomatic.
Hypocalcemia &
Hypomagnesemia
• Occur in 50% or more of IDMS born to mothers who
are IDDM
• Decreased parathormone or parathyrin hormon
(
PTH) secretion in IDMs
• IDMs may have decreased calcium transfer
• Decreased Mg++ levels in mothers
• ? Decreased Mg++-→Decreased PTH
Polycythemia/
Hyperbilirubinemia
• Fetal hypoxia→Polycythemia→
hyperbilirubinemia
• ? Ineffective RBC Production
• Polycythemia may lower glucose levels
Management of IDMs
• Delivery:
✓Consider as high risk. (mother & infant)
✓Follow basic steps of resuscitation for infant.
Management
• Post-delivery Observe / Evaluate for:
Asphyxia.
Birth injury.
Malformations.
Macrosomia.
Hypoglycemia.
Respiratory Distress.
Management of Hypoglycemia
• May be asymptomatic
• Can occur within 30 minutes.
• May last up to 48 hrs or more.
• Check Blood Glucose as soon as possible
after birth and at regular intervals for 48 hrs.
• Early feeds.
• Blood Glucose < 30 mg/dl IV dextrose
recommended.
Prognosis
• IDMs 10 x more likely to be obese (1960)
• Macrosomic infants 6 X likely to be obese at
age 7 (Vohr 1980)
• Increased risk for teenage obesity
• Increased risk for glucose intolerance as young
adults (19%)
• No developmental problems noted in
asymptomatic hypoglycemic infants.
Follow up for the IDM
• Developmental risk:
• CP , seizures 3-5 X common. SGA IDM infants
have increased risk for cognitive delay at 3-5
years.
• Metabolic Risk:
• IDMs with 1 parent Type 2DM have 1-6 % risk
of DM themselves
