Pediatric Fever of Unknown Origin
أ:رضاحملا
..د
أحمد هاشم
عبد الغفور
Objectives
:
By the end of this subjects the students should be able to :
1. Define PUO
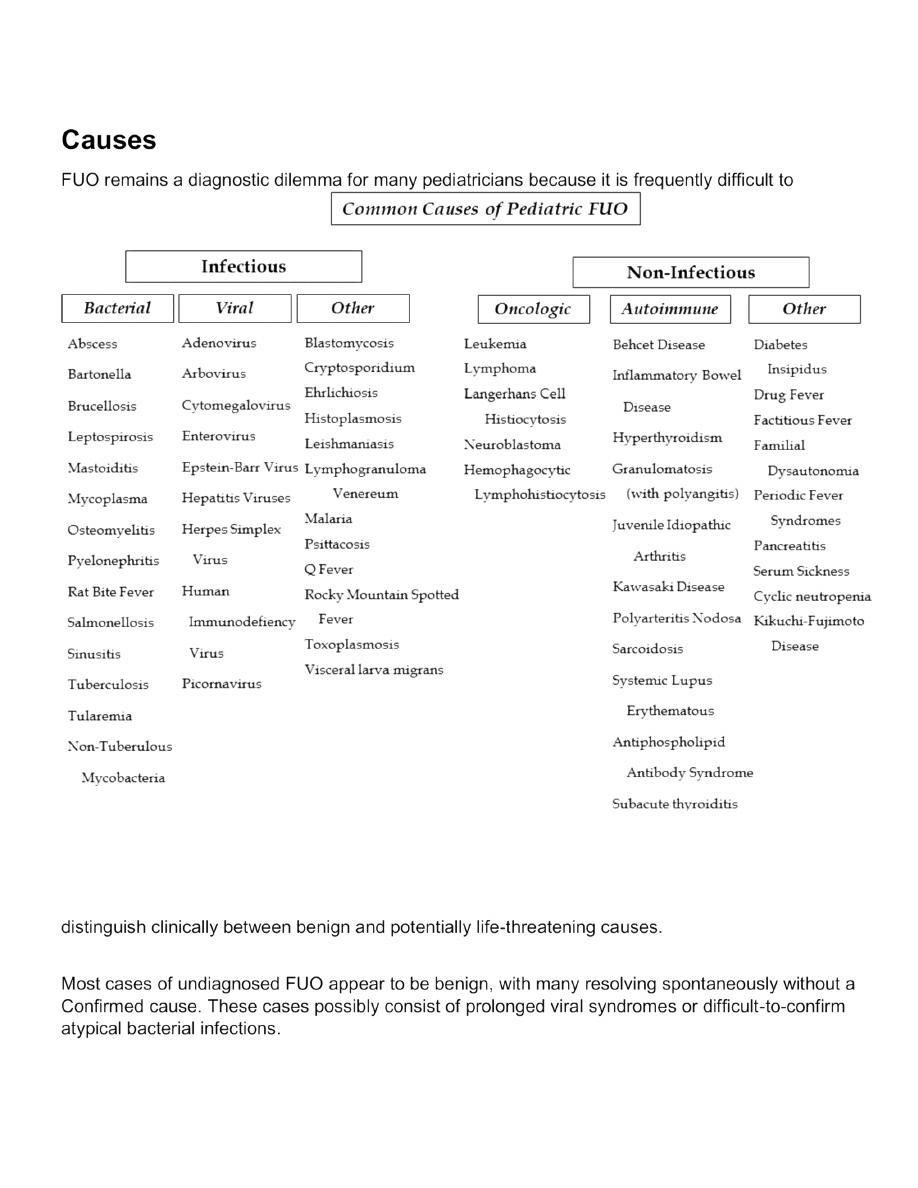
2. Clarify the causes of PUO
3. Diagnose PUO
4. Treat PUO
Fever is a common complaint in children. In most cases, fevers are due to self-limited viral infections
and require no more than symptomatic treatment.
Sometimes fever is due to uncommon infections that are diagnosed by history and physical
examination and require antibiotic treatment without laboratory evaluation.
In a few clinical situations, the cause of fever is not easily identified. Fever without a source (FWS)
may need further evaluation that includes laboratory tests or imaging. Rarely, the fever is more
prolonged, requires more intensive evaluation, and fails in the category of fever of unknown origin
(FUO).
There is often confusion about the terms FUO and FWS.
Distinguishing between FUO and FWS is important and is based on duration of fever. FWS can
progress to FUO if no cause is elicited after 1 week of fever.
Fever Physiology
Body temperature is primarily controlled by the hypothalamus via regulation of pulmonary, skin, and
metabolic systems. Furthermore, infants and young children maintain higher temperatures than older
children and adults, primarily because of increased metabolic rate and body surface-to-weight ratio.
Fever generally is defined as a core temperature of at least 38.0 °C(100.4°F) and is the result of a
complex series of signaling cascades initiated in response to specific biologic stimuli.
Definition of Fever of Unknown Origin
FUO has more recently been defined as a 3S.0°C (100.4°F) that lasts longer than at least 8 days
without a clear source.

Evaluation
History and Physical Examination
1. The first step in evaluating FUO is documentation that fever is actually present. Parental
perception of fever often varies from the medical definition, It is useful to determine what the
parent defines as fever and whether this varies from the medical definition of 38.0 °C
(100.4°F)
. Usually parents frequently report tactile or subjective fevers without actually
measuring the patient’s temperature with an instrument. Parents should be asked if the
temperature was checked using a thermometer.
2. Any associated symptoms and the timing of antipyretic administration is particularly
important.
3. A detailed description of the patient’s fever pattern as intermittent (e.g. tuberculosis),
recurrent (e.g. periodic fever disorders), relapsing (e.g. rat. bite fever), remittent (e.g.
endocarditis, juvenile idiopathic arthritis), or sustained (pyogenic abscess) can sometimes
narrow the differential diagnosis.
4. information on the frequency timing of fevers can be helpful in determining the fever curve
and ability to document the fever in the medical setting.
Periodicity of fever and the presence of other symptoms at the time fever is present can aid in making
certain diagnoses, such as periodic fever, aphthous stomatitis, pharyngitis, and adenopathy (PFAPA)
or other periodic fever disorders, without further expensive evaluation.
A thorough physical examination should be performed that documents vital signs and any reported
weight loss ..
Physical signs commonly provide evidence of the underlying diagnosis Serial physical examinations
should be performed, and observation in a controlled inpatient setting may be beneficial because up
to 25 % of significant physical findings may be (absent at the time of presentation).

Laboratory Studies and Imaging
A number of basic laboratory studies may be used to determine the source of FUO.
1. complete blood cell count (CBC) with differential count and smear can suggest an infectious
or oncologic cause.
2. Blood and urine cultures are recommended, with the understanding that repeat cultures may
be needed.
3. If the patient has neurologic symptoms, cerebrospinal fluid (CSF) studies are also indicated.
Whenever possible! cultures should be obtained before initiating antibiotics to avoid
ambiguity and contamination of results.
4. Abnormalities in serum electrolytes or liver enzymes may indicates viral, atypical bacterial, or
hematologic causes.
5. Specific molecular testing for HIV, tuberculosis, or atypical bacterial pathogens and viral
serologies is expensive and final results can be delayed days to weeks. These tests should be
performed based on specific risk factors or suggestive physical findings.
6. Testing for acute-phase reactants, such as C-Reactive Protein (CRP), Erythrocyte
Sedimentation Rate (ESR), and ferritin, is common in the evaluation of FUO. These tests
results are nonspecific and not diagnostic of any particular disorder. On the other hand,
elevated acute-phase reactants should encourage the Physician to proceed with further
appropriate evaluation. Of note, normal acute-phase reactant results do not exclude serious
causes of FUO.
Note: ESR is an indirect measurement of serum acute-phase protein concentrations, and
physiologic values vary based on age, gender and other factors. Serum ESR may be altered in
cases of abnormal serum protein concentrations, including fibrinogen, albumin, and
immunoglobulin. In addition, ESR is subject to hemoglobin concentration and size, shape, and
number of red blood cells. ESR is useful in determining chronic inflammation or infection, but
for the previously stated reasons, it should be used with caution as a diagnostic tool
particularly in the setting of possible alterations in serum protein concentrations.
7. Radiographs and imaging may play a role in the evaluation of FUO, but research suggests
that empiric imaging has limited utility. Chest radiographs should be performed if pulmonary
symptoms are present or if there is concern for atypical bacterial infection, HIV, tuberculosis,
or oncologic processes. Additional imaging techniques, particularly computed tomography
(CT) scan and magnetic resonance imaging (MRI), are associated with various risks and
should be performed discriminately.

Management and Empiric Treatment
1. The first step in the management of FUO is to discontinue all nonessential pharmacologic
agents, including antipyretic medications.
Drug fever can manifest at any time after starting a
medication, with an overall incidence of up to 5%.
Note: Drug fever is a common source of FUO and can be caused by any agent, including
antibiotics, ibuprofen, and acetaminophen. Once the drug is discontinued, fever usually abates
within 24 hours or two half-life of the drug, typically resolving within 72 to 96 hours. If drug
fever is suspected and the patient is taking multiple medications, eliminating one drug at a
time may be helpful in identifying the offending agent.
In an otherwise healthy, well-appearing child with FUO, it is not recommend routine use of
empiric antibiotics or anti-inflammatory agents.
2. Empiric antibiotics can delay the diagnosis of common infectious causes of FUO, such as
endocarditis, osteomyelitis, central nervous system infection, or abscesses. Pediatricians
commonly prescribe tetracyclines (namely, doxycycline) or macrolides for presumed atypical
bacterial infections in the absence of risk factors or clinical criteria for these diseases
3. Corticosteroids can play a significant role in treating certain causes of FUO, such as
autoimmune disease. There is no urgency for empiric treatment in most autoimmune diseases,
and treatment should be started after the diagnosis is confirmed.
On the other hand, immune suppression should not be a contraindication for specifically
indicated short-term corticosteroids.
Thank you