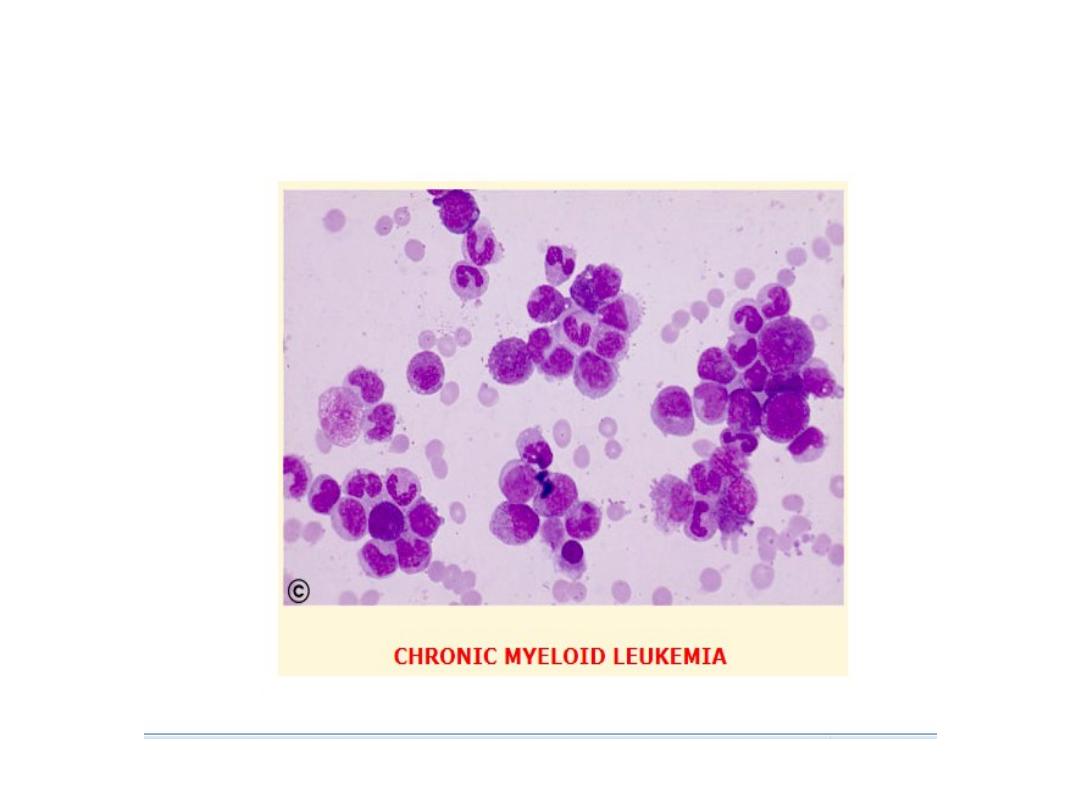
Chronic myeloid leukaemia( CML)
;

Learning objectives
•
1
-
Definition and etiology
•
2
-
Natural history and presentations
•
3
-
Investigations
•
4
-
Management

CML is an excessive proliferation with fairly normal maturation.
The disease occurs mainly between 30 and 80 years with a peak
incidence at 55 years. It is higher in men than in women (1.7:1).
Etiology:
The etiology is unknown however large doses of radiation can
induce CML.
Cytogenetic and molecular aspects:
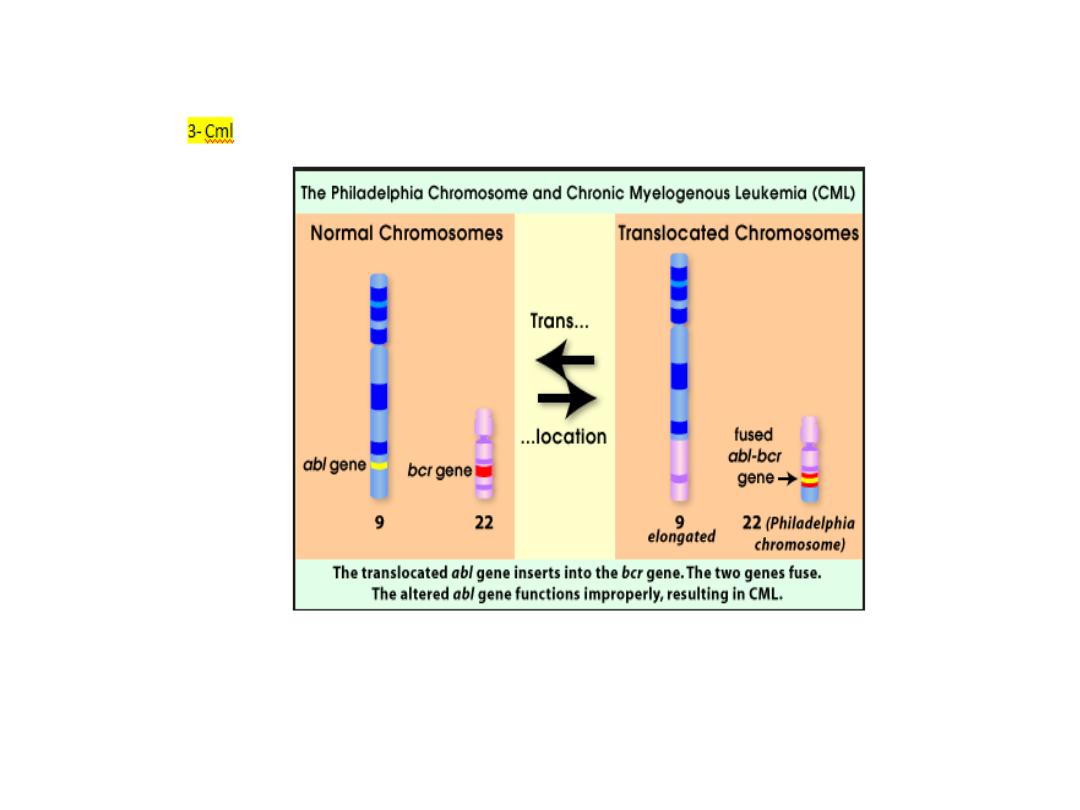

90% of patients with CML have a chromosome abnormality
known as the Philadelphia (Ph) chromosome which is due to
translocation between chromosome 22 and 9.
The break on chromosome 22 occurs in the breakpoint cluster
region (BCR) which form with the fragment from chromosome 9 the
Abelson (abl) oncogene, which forms a chimeric gene. This chimeric
gene codes for protein with tyrosine kinase activity, which plays a
causative role in the disease. Some patients with ph-negative also
have evidence of the same molecular abnormality.

Natural history:
1- chronic phase: in which the disease is responsive to treatment.
2- Accelerated phase: in which disease control becomes more
difficult.
3- Blast crises: in which disease transform into an acute leukaemia
(either myeloid 70% or lymphoblastic 30%).

Disease acceleration is defined by the development of increasing
degree of anaemia, cytogenetic clonal evolution, or blood or
marrow blast between 10-20%, blood or marrow basophils ≥ 20%,
or platlets count < 100.000/ML.
Blast crises is defined as acute leukaemia with a blood or
marrow blast ≥ 20%.

Clinical features:
1- Generally the presentation is insidious, some patients are
diagnosed accidently during routine test.
2- Other patients present with fatigue, weight loss, breathlesness,
abdominal discomfort from splenic enlargement, sweating with
vague ill health.
3- Less commonly feature related to granulocyte or platlets
dysfunction (infection, thrombosis or bleeding) or with leukostatic
manifestation due to severe leukocytosis or thrombosis.
Physical finding
:
mild to moderate splenomegally, occasionally mild hepatomegally,
lymphadenopathy, and extra-medullary tumor are unusual except
late in the disease
.

Investigation:
1- Normocytic normochronic anaemia.
2- Elevated W.B.C count with various degrees of immaturity of the
granulocytic series.
3- The mean platlets count is 445 x 10
9
/L.
4- Blast cells in the peripheral circulation usually less than 10%.
5- Leukocyte alkaline phosphatase is characteristically low in CML
cells.

6- Serum level of vitamin B
12
and B
12
binding proteins are generally
elevated.
7- Basophilia increased in later stages causing pruritis due to
histamine production.
* Blood film shows full range of granulocyte precursor with peaks
at the myelocyte and mature granulocyte stage of maturation.
Bone marrow cellularity is increased in patients with CML with
blast cell is generally normal or slightly elevated. Bone marrow
material should be obtained for chromosome analysis.

Management
:
No specific therapy is required if the patient is asymptomatic and
the leukocyte count not greatly elevated.
1- Chemotherapy: hydroxyurea is the most widely used oral agents.
2-4 gm/day is used initially, reduced to maintain the white count in
the normal range. However, it does not affect the Philadelphia
chromosome frequency.

2- Alpha-interferon given I.M or subcutaneous at 3-9mega-unit
daily. Interferon prolong survival in those with significant reduction
in ph- positive cells.
Severe bone pain and severe weight loss are reasons for
discontinuation.
3- Initab mesylate(Imatinib): this agent is an inhibitor of the BCR-
abl.- Tyrosine kinase. Over 76% achieving ph-chromosome
negatively. It is also very active in interferon resistant cases, in
accelerated phase and blast crises.
4- Allogenic or syngeneic bone marrow transplant: this provide the
only means of obtaining long term remission in this disease. It is
available to those under 55 years of age.
Treatment of the accelerated phase is more difficult. Hydroxyurea
(hydroxyl carbamide) can be an effective single agent. Low dose
cytarabine can also be tried.
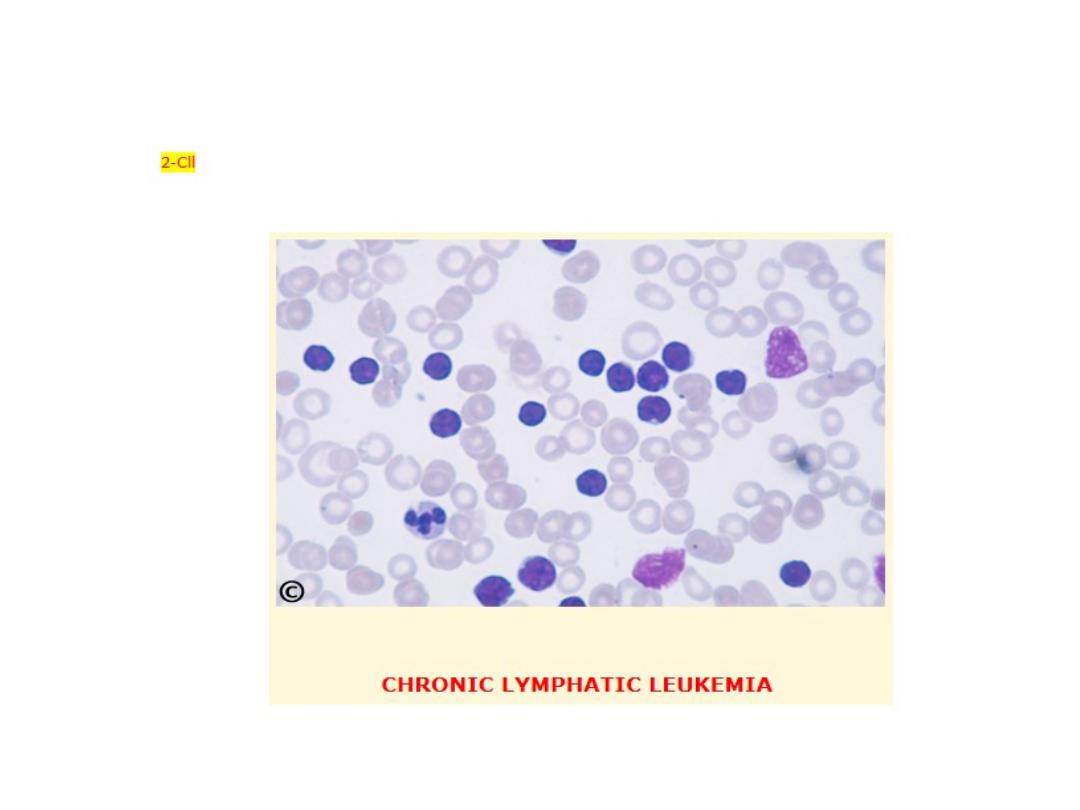
Chronic lymhocytic leukaemia( CLL)
:
Learning objectives
•
1
-
Definition and presentations
•
2
-
Staging of the disease
•
3
-
Investigations
•
4
-
Management

This is the most variely of leukaemia (30% of cases). Male to
female ratio is 2:1 with a peak at 65. In this disease B-lymphocyte
failed to transform into antibody forming cells in response to
antigen. This lead to increasing of immuno-incompetent cells and
impaired immune function. The B-cells(CD19,CD23) of chronic
lymphocytic leukaemia characteristically express a T-cell antigen,
CD5
.

Clinical features:
1- The onset is very insidious (around 25% of patients are diagnosed
incidentally).
2- Patients may present with anaemia, painless lymphodenopathy
or splenomegally.
3-Infections often occur later in the disease.

Staging of CLL:
1-Clinical stage A (60%): no anaemia or thrombocytopenia and less
than three areas of lymphoid enlargement.
2-Clinical stage B ( 30%): no anaemia or thrombocytopenia with
three or more involved areas of enlargement.
3- Clinical stage C (10%): anaemia and/ or thrombocytopenia,
regardless the number of areas of lymphoid enlargement.

Investigations:
1- Mild anaemia. Haemolytic anaemia may occur (warm auto
immune type).
2- In the majority of patients the leukocyte count is between 50-200
x10
9
/L although it may occasionally be greatly increased. About
95% or more of these cells are mature lymphocytes.
3-Bone marrow examination may be helpful in the diagnosis of
cases with a low white count and for prognosis.

4- Chromosome analysis can be helpful (cases with trisomy 12 or
13q abnormalities are associated with a poor prognosis).
5- Estimation of total protein and immunoglobulin level should be
undertaken to establish the degree of immune suppression.
In some patients there may be a monoclonal band.

M
anagement:
Treatment depends upon the stage of the disease:
1- Clinical stage A: no specific treatment is required.
2- Clinical stage B: chemotherapy with chlorambucil may be
initiated (5 mg orally daily over long periods with dose adjustment
according to blood counts) or intermittent high dose (0.4 mg/kg)
every 2 weeks increased by 0.1 mg/kg until the maximum tolerated
dose is reached. Local radiotherapy to lymph node may be given if
causing discomfort.

3- Clinical stage C: correction of anaemia with red cell concentrate.
Treatment of bone marrow failure with prednisolon 40 mg daily for
2-4 weeks. More aggressive combination chemotherapy may be
beneficial. Fludarabine, a synthetic nucleoside appears to be the
most active drug.
Total body irradiation using very small doses spread over 5 weeks in
10 fraction is effective and well tolerated especially by the elderly.
Splenoctomy may be required to treat autoimmune haemolytic
anaemia or gross splenic enlargement.