
1
Dermatology Dr. Hussein A. Al-Sultany
2019-2020
Fungal Skin Infections
Fungi exist in three forms:
1- Molds (consist of long filaments of cells called hyphae) as Dermatophyte, the molds
grow and fragment into spores.
2- Yeasts (single cell) as Candida, which is reproduced by budding.
3- Dimorphic fungi (can exist as yeast and/or mold depending on the temperature) as
Pityrosporum.
Dermatophyte Infections (Tinea)
●
Dermatophytes, have the ability to infect and survive on keratin only (skin, hair, and nail).
●
They caused by three genera: Microsporum, Trichophyton, and Epidermophyton.
●
Dermatopyte classified according to their origin into: Anthropophilic (human source),
Zoophilic (animal source) which usually elicit a brisk inflammatory response, and
Geophilic (soil source).
Clinical presentation:
Infections with dermatophytes (also called ringworms) are usually called Tinea (worm); for
further description, the anatomical site is added, including:
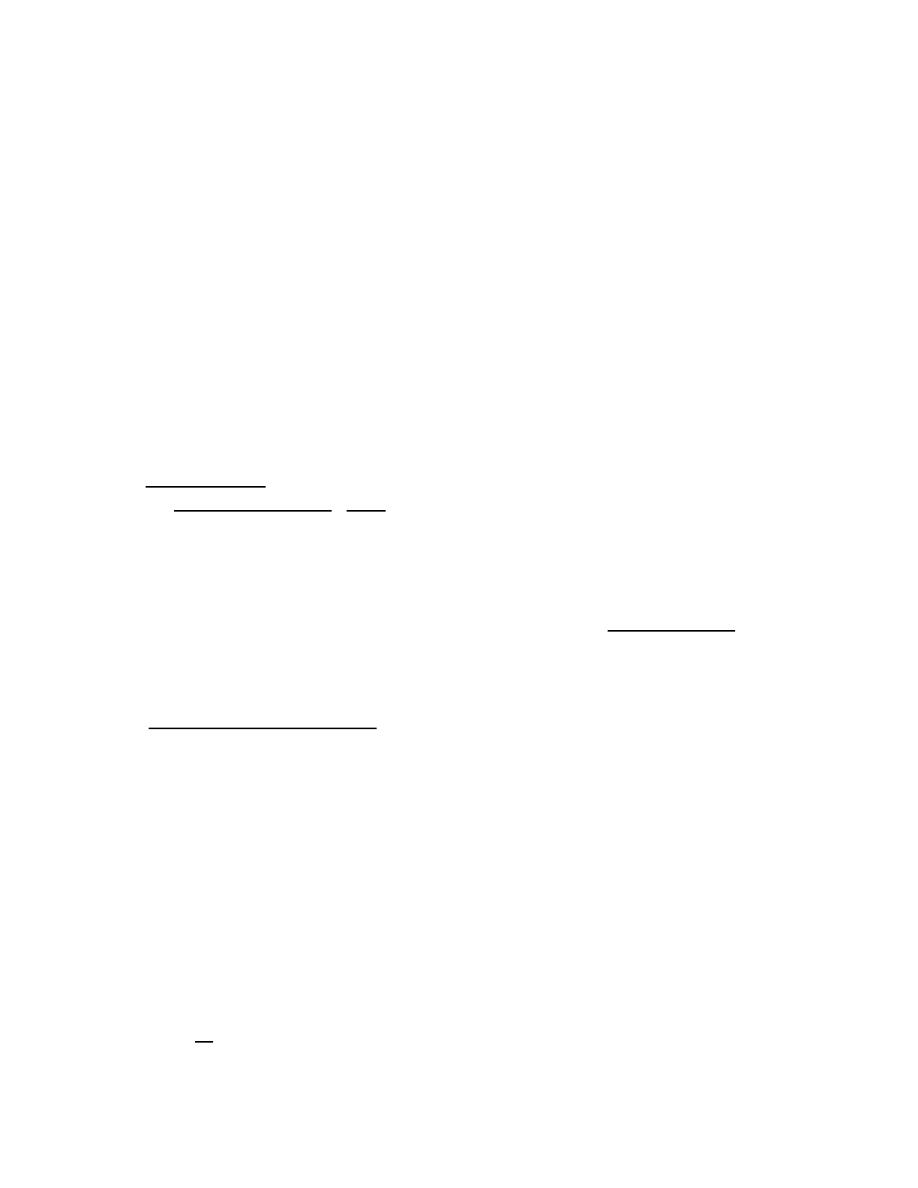
1- Tinea corporis or T. circinata: (Tinea of the trunk and limbs)
It can occur at any age.
The clinical infection usually starts from an inoculation site and
spreads peripherally, where the lesion becomes more pronounced (active border).
The active border: is a very characteristic pattern of dermatophyte infection, typically the
active border is scaly, red, and slightly elevated, a few small vesicles and pustules may be
seen within them. The lesions expand slowly and healing in the center leaves a typical
ring-like pattern, t
his characteristic annular appearance results from the immunological
elimination of the fungus from the center of the lesion, and the subsequent resolution of the
inflammatory host response at that site.
2- Tinea cruris: (Tinea of the groin)
This is common and affects men more often than women. The children are rarely affected.
The upper inner thigh is involved and lesions expand slowly to form sharply demarcated
plaques with active border. The scrotum is usually spared.
3- Tinea barbae: (Tinea of the beard)
It is limited to the beard areas of the face and neck and occurs almost exclusively in adult
males. Like tinea capitis, the hairs are infected and easily removed (easily epilated).
4- Tinea faciei: (Tinea of the face)
It is limited to the glabrous skin of the face in adult males. In pediatric and female patients,
the infection may appear on any surface of the face, including the upper lip and chin.
The lesions have annular shape with active border
2
5- Tinea pedis or Athlete’s foot: (Tinea of the foot)
It is a common type of dermatophyte infection. The forth web space is most commonly
involved. A warm moist environment of the of the toe webs predispose for this infection.
The involved area is usually white, macerated, and soggy, with itching.
6- Tinea manum: (Tinea of the hand)
It appears dry diffuse and keratotic, at the palmar surface.
7- Tinea ungium or onychomycosis: (Tinea of the nails)
The initial changes occur at the free edge of the nail, which becomes yellow and crumbly.
Subungual hyperkeratosis, onycholysis, and thickening may then follow. Usually only few
nails are infected but rarely all are.
8- Tinea incognito: (steroid modified tinea):
Fungal infections treated with topical steroids, appear as diffuse erythema and scales with
scattered papules and pustules, and usually lose their characteristic features (annular shape
with active border).
9- Tinea capitis:
●
Tinea capitis is a dermatophytosis of the scalp and associated hair (which lost and
become easily epilated).
●
It occurs mainly in children (boys more than girls),and it is very
rare in adults (because
fatty acids from sebaceous glands inhibit dermatophyte growth).
●
Tinea capitis trasmited usually by direct contact (with infected human or infected animal)
or from contaminated fomites. Transmission is higher with: decreased personal hygiene,
overcrowding, and low socioeconomic status.
●
The most important differential diagnosis of tinea capitis is alopecia areata in which the
skin is smooth without any signs of inflammation or scaling.
Types and clinical presentation:
A- Noninflammatory Type (Gray Patch):
It is the most common type in Iraq. Hairs in the affected area turn gray and lusterless and
break off above the level of the scalp with minimal Inflammation. It is usually result from
anthropophilic dermatophyte
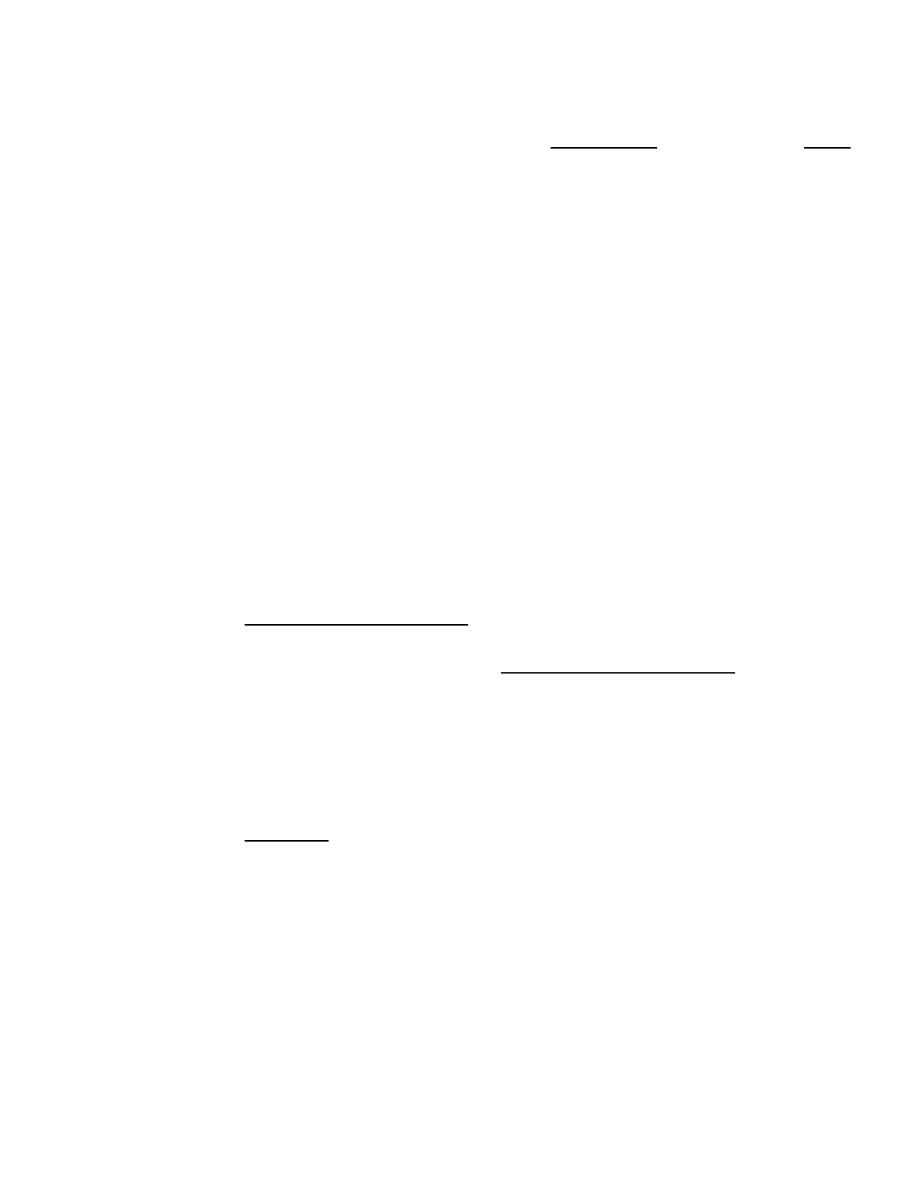
B- Inflammatory Type (Kerion):
A sever inflammatory reaction with a boggy tumor like mass that exudes pus. It is usually
result from zoophilic dermatophyte (cats, dogs and cattles). Inflammatory type are usually
pruritic, and may be associated with pain, posterior cervical lymphadenopathy, and fever.
If not treated properly; it is often results in scarring alopecia.
C- “Black Dot” Tinea capitis:
Hairs broken at the level of the scalp leave behind black dots in the areas of alopecia .
D- Favus (honeycomb):
Characterized by thick yellow crusts (scutula), which may lead to scarring alopecia.
Dermatophytid “id” Reaction:
A non infective cutaneous eruption (usually papulovesicular) representing an allergic
response to a distinct focus of a dermatophyte infection. The condition disappears
spontaneously when the primary infection is improved.
3
Diagnosis of Dermatophyte Infections (Tinea):
1- Wood’s light:
It is a UV light of 365 nm wave length, obtained by passing the UV light through a special
filter (Wood’s filter). It is used in the diagnosis of tinea capitis only, giving a green
flourecent color.
2- Potassium Hydroxide (KOH):
The scale is scraped on a glass slide with a surgical blade. The highest number of hyphae
are located in the active border and so is the best area to obtain a sample. Other samples can
include nail clippings (in onychomycosis), or hair plucking (in tinea capitis).
A drop or two of the KOH solution (10-20%) is added on a glass slide then examined under
a microscope. Dermatophytes appear as translucent branching filaments (hyphae).
In tinea capitis the spores may seen inside the hair shaft (endothrix) or on its surface
(ectothrix).
3- Culture:
The common media used is "Sabouraud's Dextrose Agar".
Treatment:
A- Topical:
For limited skin infections.
1- Imidazole group (miconazole, clotrimazole & ketoconazole) cream or lotion or shampoo.
2- Terbinafine cream.
3- Tolnaftate cream.
B- Systemic:
1- Griseofulvin: act against dermatophyte only. It is relatively safe, and it is the treatment of
choice of tinae capitis in children (10-20 mg /kg for 1-2 months).
2-
Azole groups (imidazole and triazole) are broad spectrum antifungal (act against
dermatophyte, yeast, and
Pityrosporum
infections).
Imidazole group: (ketoconazole, 100 mg tab) can cause hepatic toxicity.
Triazole group: these newer drugs are more effective and less likely to cause hepatic
toxicity than ketoconazole, includes:
Itraconazole (100 mg cap) used twice daily.
Fluconazole (150 mg cap) usually used once weekly.
3- Terbinafine: It is fungicidal,
and has produced rapid and long lasting remission.
●
All systemic antifungal should not be given for pregnant patients.
Indication of systemic antifungal in dermatophyte infections:
1- Tinea capitis.
2- Onychomycosis.
3- Tinea incognito.
4- Widespread infection.
5- Immunocompromised patient.
6- Recurrent or persistent infection.
4
Candidiasis
Cause:
Candida albicans ; is an apportunistic organisim acting as a pathogen in the presence of
certain prediposing factors
Predisposing factors:
1- Mechanical factors: local occlusion, moisturization, dentures, and obesity.
2- Nutritional factors: iron deficiency, and malnutrition.
3- Physiologic alterations: extremes of age, and pregnancy.
4- Systemic illnesses: endocrine disease ( as DM), malignancy, and immunodeficiency.
5- Iatrogenic: catheters and medications (steroid, broad spectrum AB, and OCP).
Presentation:
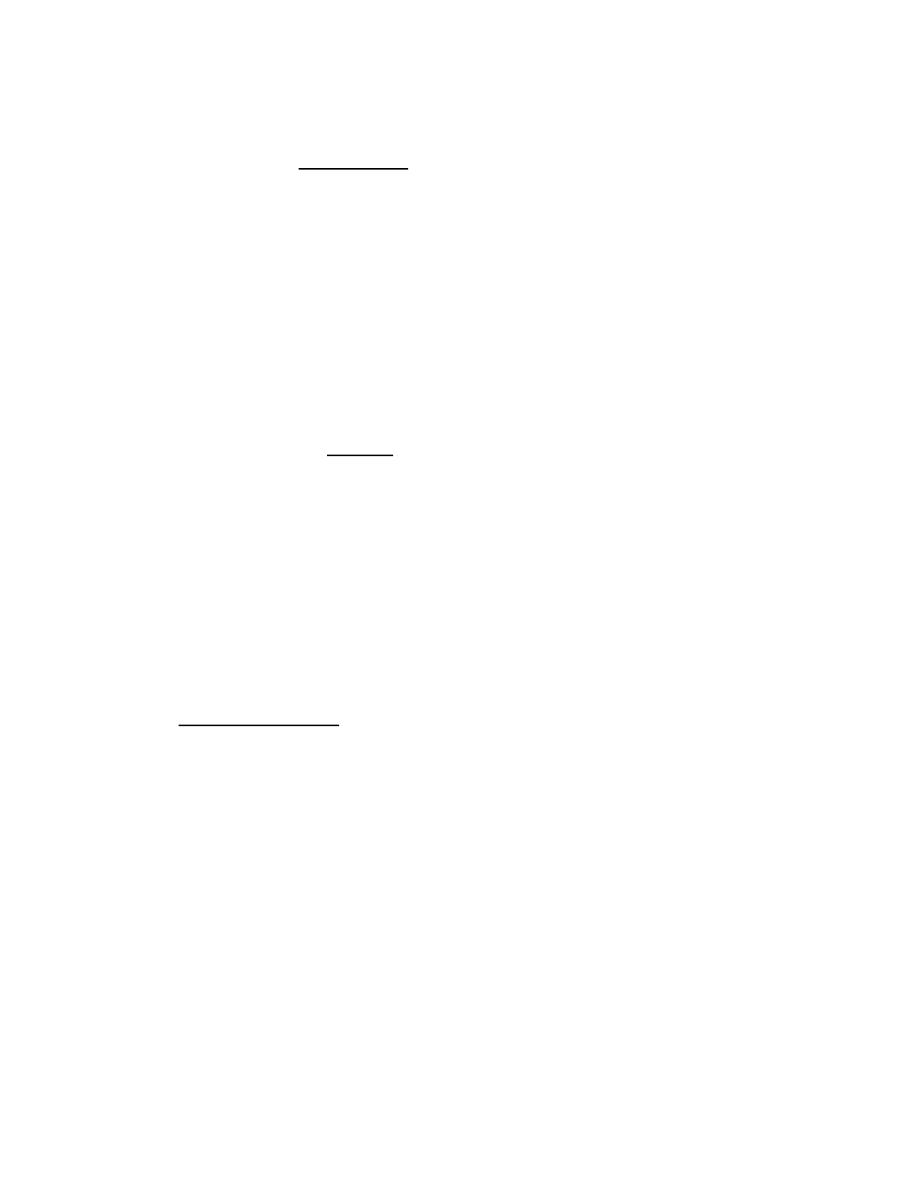
1- Flexural candidiasis:
A moist glazed area of erythema and maceration appears in a body fold; the edge shows
soggy scaling, with outlying satellite papulopustules. These changes are most common in
the groin, axillae, or under the breasts.
2- Erosive interdigital candidiasis:
Mostly seen in diabetic patients, or in persons with frequent water exposure of their hands.
3- Oral candidiasis (Thrush): one or more whitish adherent plaques appear on the mucous
membranes. If wiped off they leave an erythematous base.
4- Angular cheilitis (Perlèche): is characterized by erythema, fissuring, maceration, and
soreness at the angles of the mouth.
5- Chronic Paronychia:
The proximal and sometimes the lateral nail folds of one or more fingers become bolstered
and red and the cuticles are lost. Mostly seen in house wife (water and detergent exposure).
6- Candidal nail infection: generally results from chronic candidal paronychia and starts
near the nail fold. The nail plate becomes ridged and yellow.
7- Genital candidiasis:
Vulvovaginitis and Balanitis.
8- Chronic mucocutaneous candidiasis:
It is a chronic, treatment-resistant, candidal infections of the skin, nails, and mucous
membranes. There are specific inherited abnormalities in cell-mediated immunity,
several different forms have been described including those with autosomal recessive and
dominant inheritance patterns.
9- Systemic candidiasis:
This is seen against a background of severe illness, leucopenia or immunosuppression. The
skin lesions are begin as erythymatous macules that may become papular, nodular, pustular,
or ulcerative.

5
Investigations:
1- KOH examination:
candida appears as oval cells (yeast), and sometimes as elongated
cells (pseudohyphae).
2- Culture: Sabouraud's Dextrose Agar.
3- Investigations for the suspected predisposing factors.
●
Wood's light is not useful (negative) in all types of candidal skin infection.
Treatment:
General measures:
Predisposing factors should be sought and eliminated.
A- Topical:
Imidazole cream (miconazole, clotrimazole, and ketoconazole), amphotericin, nystatin, and
gention violet, all are effective topically.
B- Systemic:
Oral triazole as itraconazole (100 mg cap twice daily) or fluconazole (150 mg once weekly)
can be used, they are indicated for:
1- Candidal paronychia
2- Candidal nail infections.
3- Chronic mucocutaneous candidiasis.
4- Systemic candidiasis.
5- Recurrent candidiasis in immunocompromised.
6- Sever or recurrent genital infection.
6
Pityriasis Versicolor
It is a common fungal skin infection. The old name, tinea versicolor, should be dropped, as
the disorder is caused by commensal yeasts (Pityrosporum) and not by dermatophyte.
Cause:
Pityriasis versicolor is caused by the lipophilic, dimorphic organism (Pityrosporum
(orbiculare and ovale)) which is a commensal yeast. the pathogenic form of it called
Malassezia, recent researches has shown that, the genus Malassezia includes 12 species,
and the majority of pityriasis versicolor is caused by Malassezia globosa, while the classical
old species is Malassezia furfur.
Predisposing factors:
Heat, and humidity, corticosteroid therapy, Cushing syndrome, pregnancy, OCP, and
malnutrition; Predispose the Pityrosporum to convert to its pathogenic form (Malassezia).
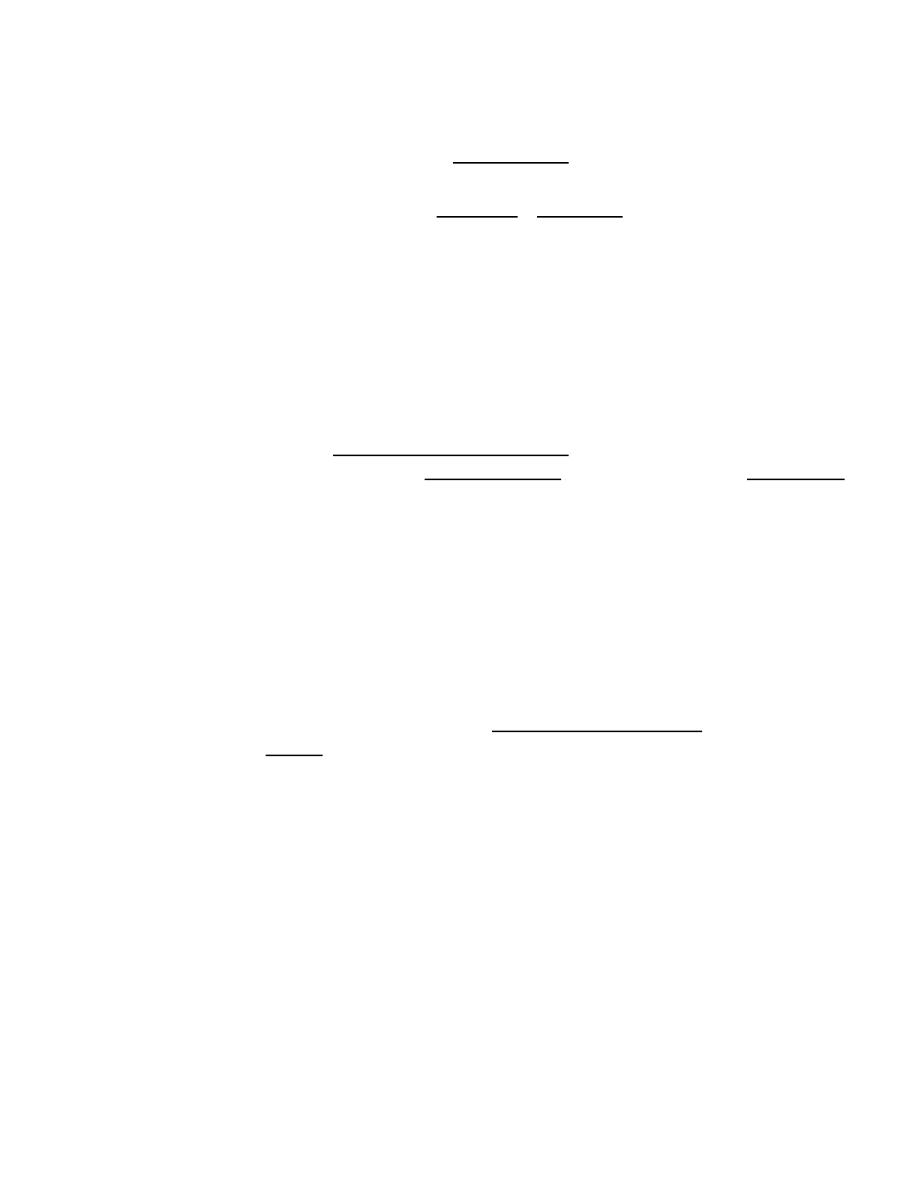
Presentation and course:
●
The disease mostly seen in adolescent and young adult (age of high sebaceous activity)
and rare in children, and mostly occur in summer months. Typical sites are the upper trunk;
neck, chest, upper back, & shoulders (areas with high sebaceous activity).
●
It presents as asymptomatic or slightly itchy, scaly, hypopigmented (in dark skin) or
hyperpigmented (in white skin) macules (so termed versicolor). The scales are accentuated
by stretching.
●
Mechanisms of pigmentary change are unclear; darkening may result from hyperkeratosis,
but lightening result from either reduced tanning or direct inhibitory effect on melanocytes
by the carboxylic acids which is released by the organisms.
●
The infectivity of the disease is very low and can be regarded as non-infectious.
Investigations:
1- KOH: show a mixture of hyphae and yeasts (a ‘spaghetti and meatballs’ appearance).
2- Wood's light: show yellow fluorescence.
3- Culture.
Treatment:
A- Topical: it is indicated for limited disease, topical treatment options include:
1- Creams: as imidazole (miconazole,clotrimazole & ketoconazole),twice daily for 2 weeks.
2- Shampoos: (ketoconazole, selenium sulphide, or zinc pyrithione) 10 minutes daily for
one week.
B- Systemic: indicated for (1) extensive or resistant infection. (2) frequent recurrences,
include: itraconazole (200 mg daily for one week), fluconazole (300 mg once weekly for 2-
4 weeks or 400 mg single dose).
C- Prevention: recurrence is common after any treatment, so it may be prevented by:
once weekly application of ketoconazole shampoo, or once monthly oral itraconazole or
fluconazole.
"Best Regards"