
1
Ca larynx
Dr.Safaa Hussain Alturaihy

3
Tumours of the larynx
Benign tumour
Papillomas
1. Single papilloma: seen in adult arise usually from the vocal cord as a
sessile or pedunculated mass, May have recurrence after removal and have
risk of change to malignancy.
2. Multiple papillomas are the usual type in children may be due to human
papilloma virus; no risk of malignancy but recurrence is common,
regression occur at puberty.
There is no histological difference between two types.

4
Clinical features:
Either silent or present with hoarseness of voice or stridor.
Malignant tumour
Mostly squamous cell carcinoma others may include
adenocarcinoma,or connective tissue tumour.
Squamous cell carcinoma:
Grading; well differentiated ,moderately differentiated and poorly
differentiated
Clinical types, ulcerative or proliferative

5
Types:
◙Supraglottic carcinoma
Area of supraglottis comprises the larynx superior to the apex of
ventricle .It includes the ventricle, vestibular
folds.arytenoids,aryepiglottic folds and the epiglottis (laryngeal
surface, tip and lingual surface).
It has rich lymphatic drainage and the tumour spread either locally
to base of tongue, glottis and pharynx or to the upper deep
cervical lymph nodes.

6
◙ Glottic carcinoma
This comprises the vocal cords and the posterior and anterior commissures.
Spread either locally to subglottis or supraglottis and rarely to lymph nodes
(4%) because no lymph drainage in this area.
◙Subglottic carcinoma
This extends from the inferior border of the glottis to the lower border of the
cricoid cartilage.
Spread locally to vocal cords, trachea, and circumferential spread, or to the
lower deep cervical LN.paratracheal and mediasinal LN.
Risk factors:
Male, smoker, alcoholic, 5th-6th decade of life and chronic laryngitis.

7
Clinical features:
●Hoarseness of voice
●●Stridor
●●●Neck mass due to LN or the tumour mass
●●●●Pain locally in the neck or referred otalgia
●●●●●Dysphagia
●●●●●●Cough
●●●●●●●General symptom like cachexia and anorexia
Investigations
●Radiological plain x-ray ,CT, MRI
●●Haematological
●●●Biochemical
●●●●Laryngoscopic examination and biopsy

8
Staging
TNM classification of sq.cell carcinoma
T primary tumour
N lymph nodes
M distant metastasis
Primary tumour
Supraglottic
T1 Tumour limited to one subsite of supraglottis like aryepiglottic fold or
arytenoids
T2 Invasion of more than one subsite of supraglottis or glottis or adjacent
region outside the supraglottis like mucosa of tongue base
T3 Limited to the larynx with fixed vocal cord or invades the postcricoid
area, pre-epiglottic tissue, base of tongue
T4 Extends beyond the larynx

9
Glottis
T1a tumor limited to one VC
T1b Involves both VC
T2 Extend to supraglottis and /or subglottis, or impaired VC
mobility
T3 Limited to the larynx with fixed VC
T4 Extends beyond the larynx
Subglottis
T1 Limited to subglottis
T2 Extend to VC with normal or impaired mobility
T3 VC fixation
T4 Extend beyond the larynx

10
Lymph nodes
N0 No LN
N1 Ipselateral single LN equal yo or less than 3cm
N2 LN 3-6cm unilateral or bilateral
N3 many LN more than 6cm
Metastases
M0 No distant metastasis
M1 Distant metastasis
Treatment
Palliative
→to decrease the patient suffering but no cure like pain relief and tracheostomy
Curative
→the aim is to cure the patient
◙Radiotherapy
It preserves the function of the larynx
Or given when the patient refuse surgery
Can be given pre or post operative in advance cases
◙Surgery
External approach as total and partial larygectomy
Endoscopic approach as microlaryngoscopy and laser surgery
◙No Ca larynx has been cured by chemotherapy


12
Tracheostomy
Creation of surgical opening in the trachea and converting this opening to astoma on the
skin surface.
Indications:
1-releife of upper airway obstruction
◙Congenital
●Bilateral choanal atrasia
●●Laryngomalacia
●●●Laryngeal web
●●●●Subglottic stenosis
◙Traumatic
●Either external trauma as in gun shot or stab wound (cut throat), or internal
trauma as inhalation of irritating fumes, swallowing of corrosives, foriegn body.
◙ Infections
●Acute epiglottitis
●●Acute laryngotracheobronchitis
●●●Diphtheria
●●●●Ludwig's angina

13
◙ Tumours
Of the tongue,larynx,pharynx,thyroid:
●In advance stage
●●If oedema from radiotherapy embarrasses respiration
●●●As adjuvant to surgery
◙ Bilateral recurrent nerve palsy
●After thyroidectomy
●●Bulbar palsies
2, Protection of tracheobronchial tree, this achieved by:
● Provide good aspiration
●● Protect from inhalation of saliva, food or blood
●●● Clear the airway from stagnation of bronchial secretion
These conditions include:
●Coma due to head injury, poisoning, cardiac arrest
●●Burn of the face, neck
●●●Multiple fractures of the mandible
●●●●Neurological diseases as myasthenia gravis, tetanus, cervical cord lesions or
injury

14
3. Tretment of cases lead to respiratory insufficiency as in
● All above conditions
●● Pulmonary diseases as
►Chronic bronchitis and emphysema
►Post operative pneumonia
●●●Severe chest injury (flail chest)
●●●●Neuromuscular in coordination
●●●●●Need for intermittent positive pressure respiration IPPR
Aims of tracheostomy
◙Relief upper airway obstruction(By-passing)
◙◙Reduce the dead space (30-50%)
◙◙◙Allowing easy toilet of bronchi
◙◙◙◙Using of mechanically assisted ventilation PPV
15
Criteria for emergency tracheostomy:
●Recession of suprasternal notch and intercostals
space
●●Anxious, pale, sweating faces
●●●Cyanosis, indicate a late and grave stage
Types of tracheostomy
Elective or emergency,Temperary or permanent
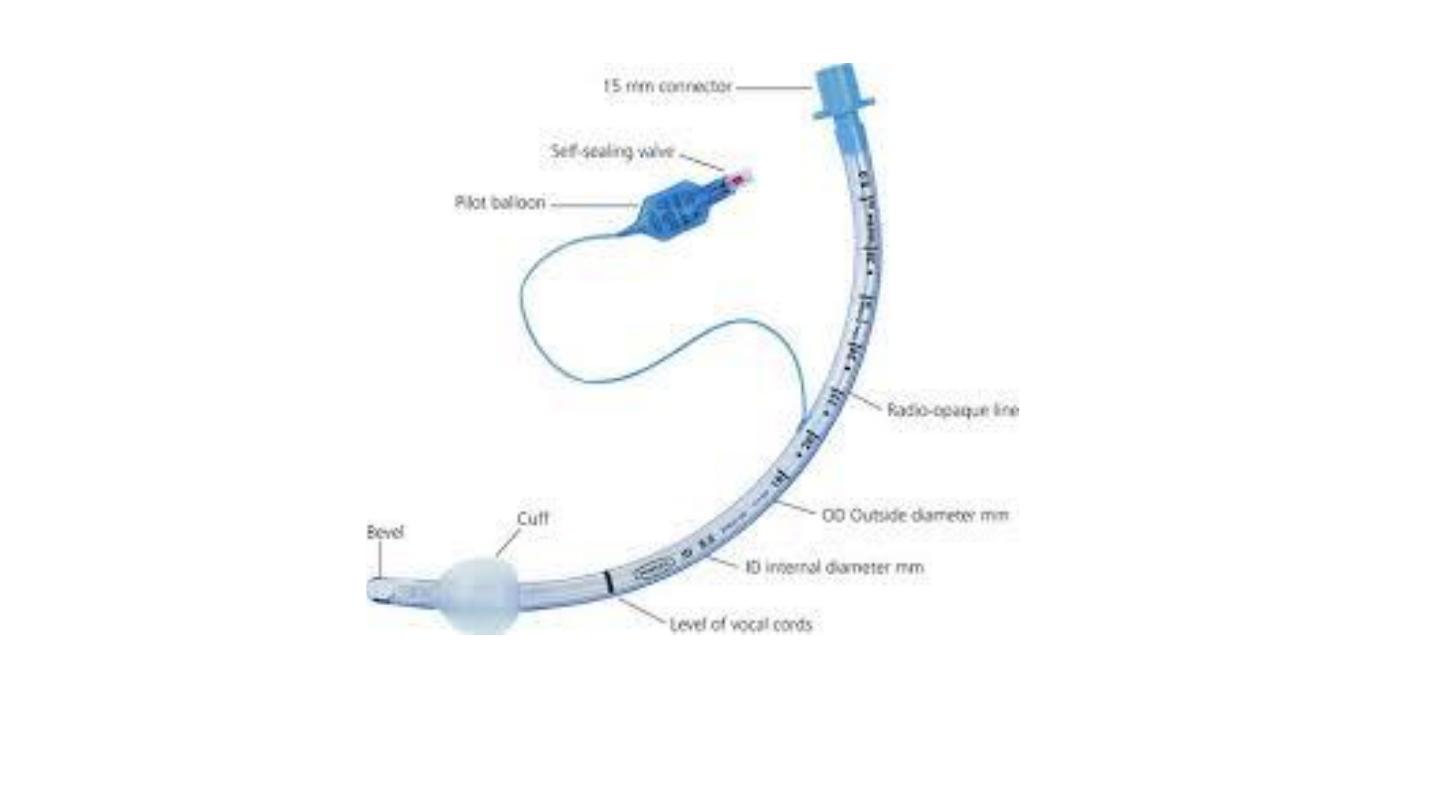
Types of tracheostomy tube
●Metalic
●●Non metallic


18
Technique of tracheostomy
◙Anaesthesia either local or general
◙Position extension of the head
◙Incision either vertical or horizontal ,vertical always used in emergency
midline from the level of cricoid cartilage to the suprasternal notch
,horizontal incision about 2 fingers breadth above the suprasternal notch
◙ Midline separation of strap muscle using blunt dissection scissor
vertically with haemostasis of all bleeding points
◙ Thyroid isthmus either divided or separated
◙ Trachea exposed and opened ,tracheal incision is at 2nd,3rd and fourth
tracheal rings
◙ Insertion of the tube
◙ Closure of the wound loosely and dressing

19
Post-operative care
●Nursing, constant attention for first 24 hours
●●Position upright position in bed
●●●Humidification of inspired air
●●●●Suction applied regularly
●●●●●Fixation of the tube by silk suture to the skin and tape tied around
the neck
●●●●●●Care of the wound by dressing and antibiotic
●●●●●●●Change the tube at least after 36-48 hours and in children it
should be done at least one week after surgery

20
Complication of Tracheostomy
◙Immediate
●Haemorrhage from anterior jugular vein ,thyroid gland
vessels
●●Air embolism due to air sucked into large neck veins that
may be opened
●●●Apnea due to sudden CO2 wash out
●●●●Cardiac arrest either due adrenaline production of
anxious patient,hyperkalaemia due to respiratory alkalosis or
rapid rise in PH as aresult of rapid CO2 wash
21
◙Intermediate complications
●Displacement or dislodgment of tube
●●surgical emphysema
●●●Pneumothorax and pneumomediastinum
●●●●Obstruction of tube by crusts
●●●●●Infections of the wound
●●●●●●Tracheal necrosis due to over size of tube,improper curve of
tube or pressure of the cuff on the trachea
●●●●●●●Tracheoarterial fistula and tracheo-oesophageal fistula
●●●●●●●●Dysphagiadue to tethering of the larynx,pressure of inflated
cuff on the oesophagusor due to original cause of tracheostomy

22
◙
Late complications
●Tracheal stenosis due to inflatable cuff, improper placed
insicion, repetitive incision, tracheal resection or trauma, or
tracheal infections
●●Difficulty with decanulation especially in long standing
tube due to suprastomal granulation and fibrous mass
●●●●Tracheocutanous fistula and scars especially in long
standing tracheostomy

23
Neurological affection of the larynx
Sensory dysfunction
The sensory nerve supply to the supraglottis is from yhe vagus via internal
laryngeal nerve.Stimulation produces a cough reflex which prevents food
and saliva from entering the airway,thus being very important protective
reflex.
Loss of this reflex predispose to aspiration.
Uncontroled aspiration lead to sever pneumonia which is life threatening.
Sensory paralysis is caused by lesions affecting the vagus nerve in the skull
base or in the upper neck
Laryngeal spasm
It is most commonly seen postoperatively in the patient with with sensitive
larynx that has been irritated by secretion or blood.
The cords become adducted and the patient cannot breath
Laryngeal spasm may present in the clinic with repeated chocking episodes
and loss of voice gastroesophageal reflex or postural drip may be the cause

24
Functional dysphonia
Is form of laryngeal spasm which is often induced by anxiety and panic
attach It is most commenly present in young female,who present with
aphonia. The vocal cords will de seen lying equidistant from the midline and
move normally with deep inspiration but on phonation will not meet in the
midline.Patient able to cough and when cough ,the cord will meet in the
midline.
Treatment is by reassurance with good speech therapy.
Vocal cords paralysis
It can be unilateral or bilateral and can be adductor or abductor paralysis
Abductor paralysis means loss of power of abduction i.e V.C are in
adduction
Adductor paralysis means loss of power of adduction i.e V.C are in
abduction

25
Causes
1.malignancy 25%
2.surgical trauma
3.idiopathic
4.inflammatory T.B of the lung
5.non surgical trauma pressure by atrium enlargement or by aneurysm
6.neurological as DM,CVA
7.other as rheumatoid arthritis
The left nerve affected more because it has longer course

&