
Dr.Safaa Hussain Alturaihy
1

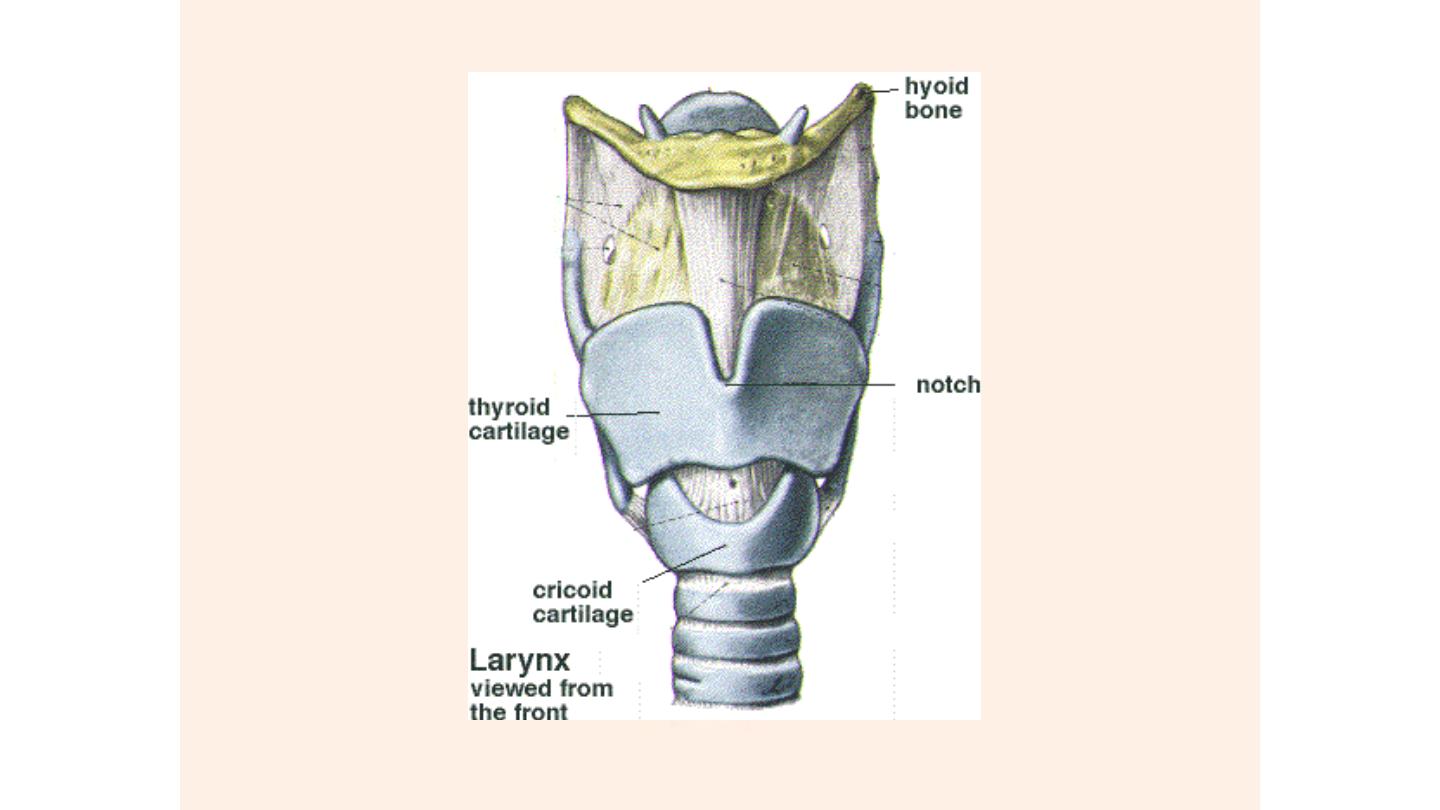
The larynx is an integral part of the respiratory system and is the
organ of voice production .The larynx consists of a cartilaginous
framework bound together by ligaments and covered muscle and
mucous membrane. The cartilage of the larynx is either unpaired
or paired cartilage.
Unpaired cartilages:
1.Thyroid cartilage
2.Cricoid cartilage
Paired cartilages:
1.Arytenoid car.
2.Corniculate car.
3.Cuniform car.
The Larynx
Dr.Safaa Hussain Al-Turaihy
Dr.Safaa H. Alturaihy

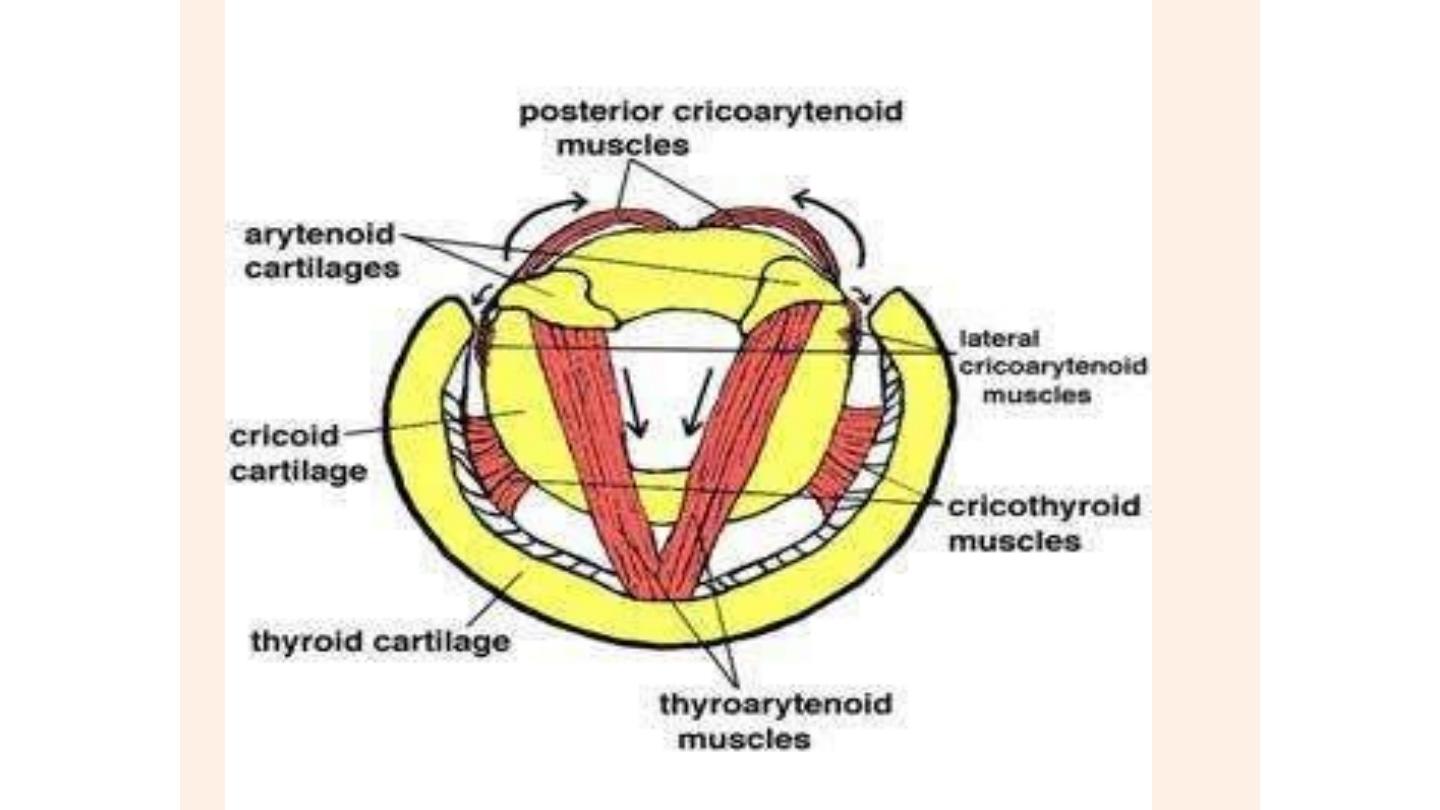
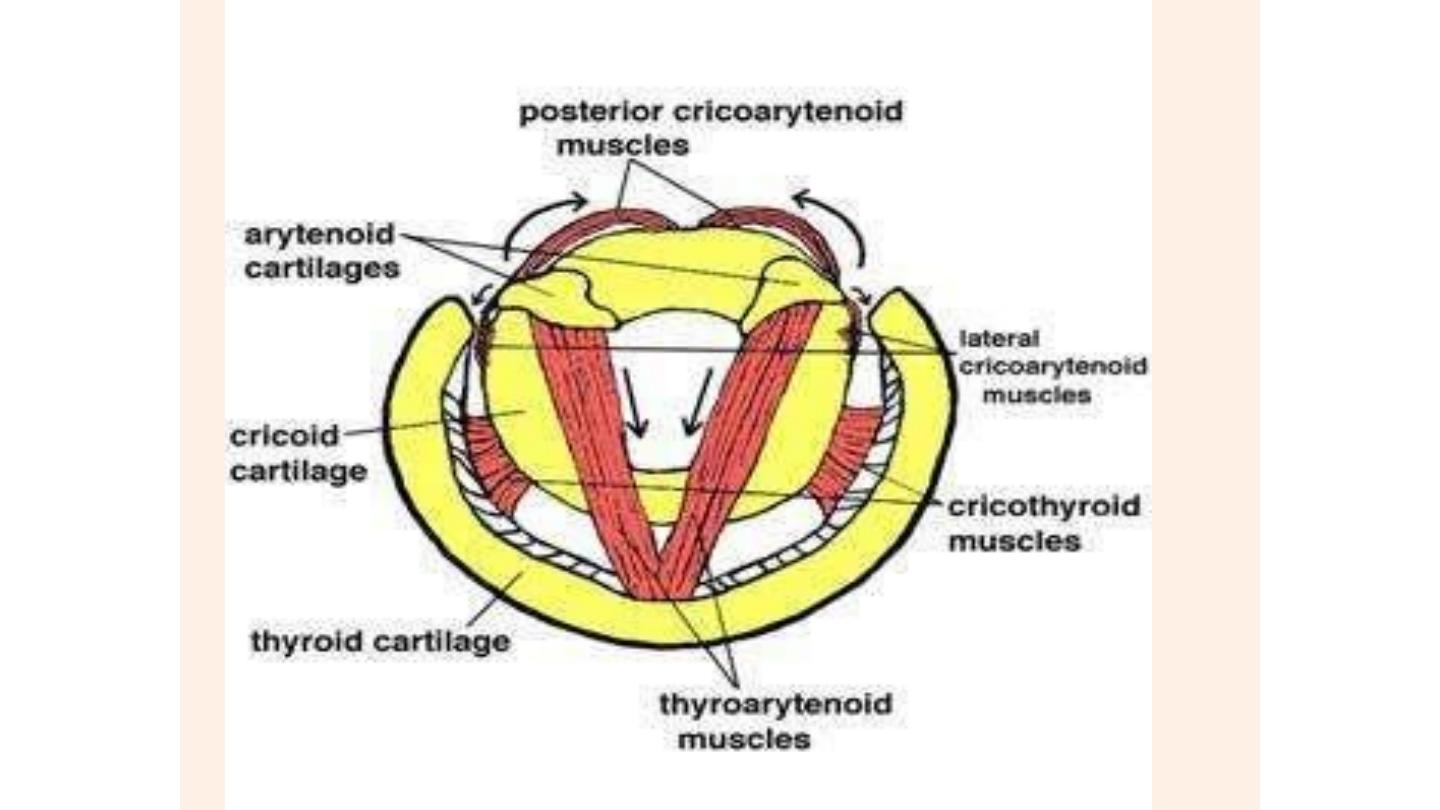
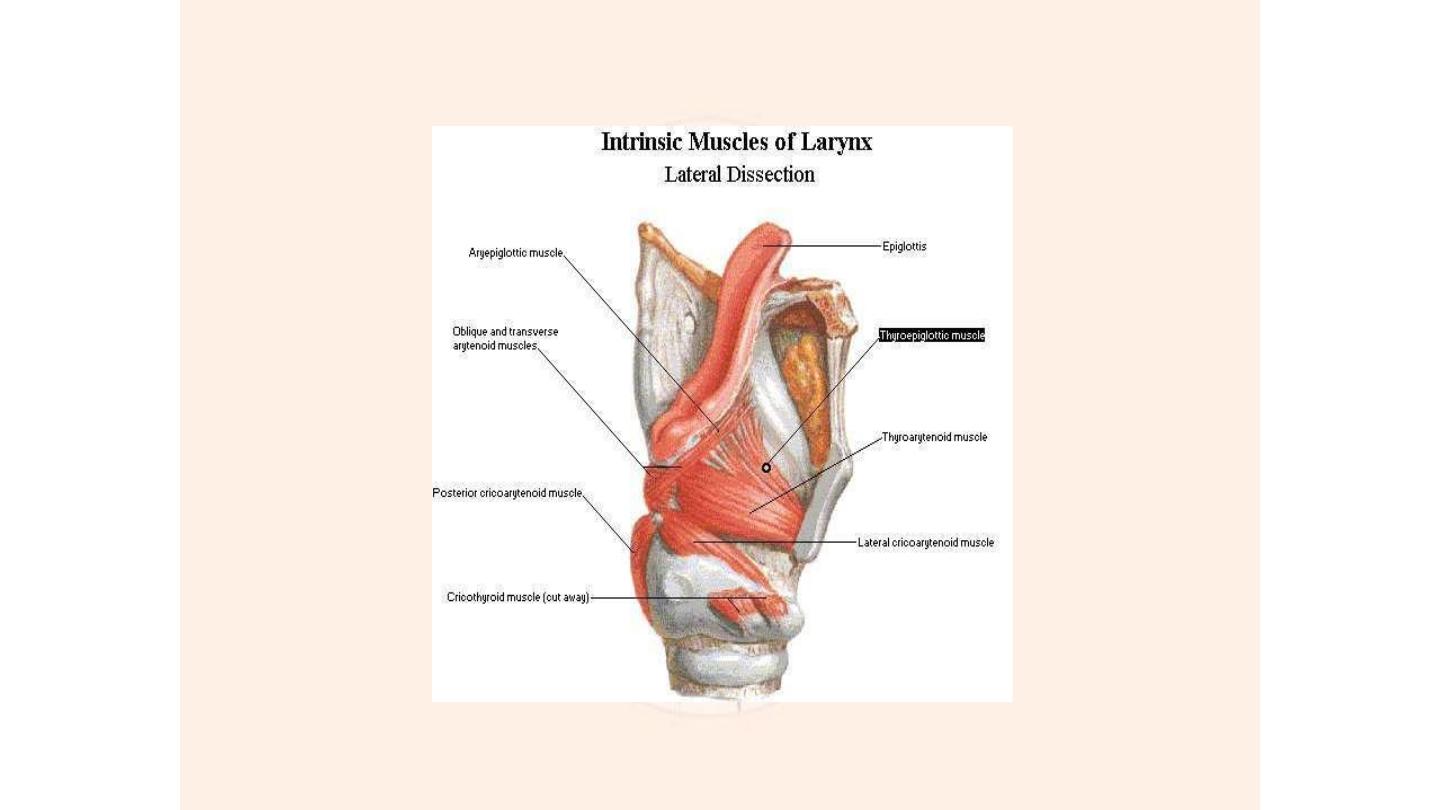
Laryngeal Muscles:
Are of 2 types:
Intrinsic muscle of larynx
:
۞
◙Abducors(opens):
It is one muscle (posterior cricoarytenoid muscle)paired muscle
◙ Adductors(closes)
●Lateral cricoarytenoid muscle,paired also.
●● interarytenoid muscle which is unpaired
◙Muscle adjust the tension of vocal cord
● Thyroarytenoid muscle with its specialized free edge
portion,vocalis muscle
◙ Muscle adjust the length of vocal cord
● Cricothyroid muscle (the only intrinsic muscle which lies on the
out side

Extrinsic muscle of larynx:
۞
◙Strap muscle of the neck
●Sternothyroid muscle
●●Sternohyoid muscle
●●●Thyrohyoid muscle

Nerve supply:
All above muscle are supplied by recurrent laryngeal nerve except
cricothyroid
muscle which is supplied by external laryngeal nerve which
is branch of superior laryngeal nerve.
Recurrent laryngeal nerve is branch of vagus that has different courses
on each side.
In the
left
side it passes under the aortic arch and ascend in the tacheo-
oesophageal groove, entering the larynx underneath the inferior
constrictor muscle.
Right
recurrent laryngeal nerve is shorter than the left looping around
the subclavian artery , because of its long intrathoracic course,the left
recurrent laryngeal is more likely to be involved in cases of
bronchogenic carcinoma
The recurrent laryngeal nerve is sensory to the mucosa below the vocal
cord .while the internal laryngeal nerve is sensory to the mucosa of the
larynx above the vocal cords

Blood supply:
The larynx above the vocal cords is supplied and drained by
the superior laryngeal artery and vein which enter the
larynx through the thyrohyoid membrane the region below
the cords is supplied and drained by the inferior laryngeal
artery and vein branches of inferior thyroid artery.
Lymphatic drainage:
The vocal cords have no lymph drainage, the supraglottis
drains upwards via the superior laryngeal lymphatic pedicle
which ends in the upper deep cervical chain.
The subglottics drain to both the prelaryngeal and
paratracheal nodes and also directly to the lower deep
cervical chain and the mediastinum.

Histology:
The larynx is lined by two different types of epithelium:
squamous over the true vocal cords and the upper
quarter of posterior surface of epiglottis and columnar
ciliated over the rest of the larynx which commonly
undergoes squamous metaplasia in response to air
pollution and smoking.
Functions of the larynx
:
◙
Phonation
Vocal cords act as vibrator
◙
Protection of respiratory tract by:
●
Laryngeal elevation
●●
Epiglottis
●●●
Sensory nerve supply(cough)
●●●●
Vocal cords
Characterized by flaccidity of supraglottic structures, it is the commonest
laryngeal stridor (60%-70%).
Pathology:
●
Softness or flabbiness and lack of consistency of the larynx.
●●
Thinning and hypocellularity of the laryngeal cartilage.
●●●
Wrinkled loose mucosa especially over the arytenoids cartilage.
Clinical features:
●
Stridor is high pitch inspiratory stridor which is present at birth and
become obvious when the child become active or have URTI.The stridor
start to increase at the first 8 months and become maximum at 9-12
months,it is intermittent, during feeding or crying and more obvious during
sleep especially when the child lies on his back, on hyperextension of the
neck the stridor will decrease.
Laryngomalacia
:

●●
Long and narrow epiglottis prolapsed backwards with omega
shape (
Ω
)
●●●
Small,lax laryngeal inlet lead to sucked together by each
inspiration.
●●●●
The suprsglottis is deepened and narrow and the vocal cords
are difficult to see
●●●●
Elongated arytenoids car.covered by loose redundant mucosa
and on inspiration. Crossing one over the other.

Treatment:
Most cases disappear spontaneously between 18 months to 2
years, if the child is with feeding difficulty. Failure to thrive or
respiratory distress this needs active treatment which is:
▪ Tracheostomy
▪▪ Excision of the redundant mucosa
▪▪▪ Division of aryepiglotic fold
Other congenital abnormality of the larynx:
●
Subglottic stenosis
●●
Subglottic haemangioma
●●●
Laryngeal web
●●●●
Laryngeal cyst

Intubation granuloma
This injury mostly occur in patient mostly have a traumatic
intubation due to rough intubation,prolong intubation,or use of
large size tube.
Clinical features:
Patient presented with hoarseness of voice few days or weeks
after an operation, and rarely presented with stridor.
On examination by indirect laryngoscope or by endoscope, large
fleshy granuloma arising from one arytenoids if not treated may
lead to fibrosis.
Treatment:
●Voice rest
●●Endoscopic removal of granuloma

16
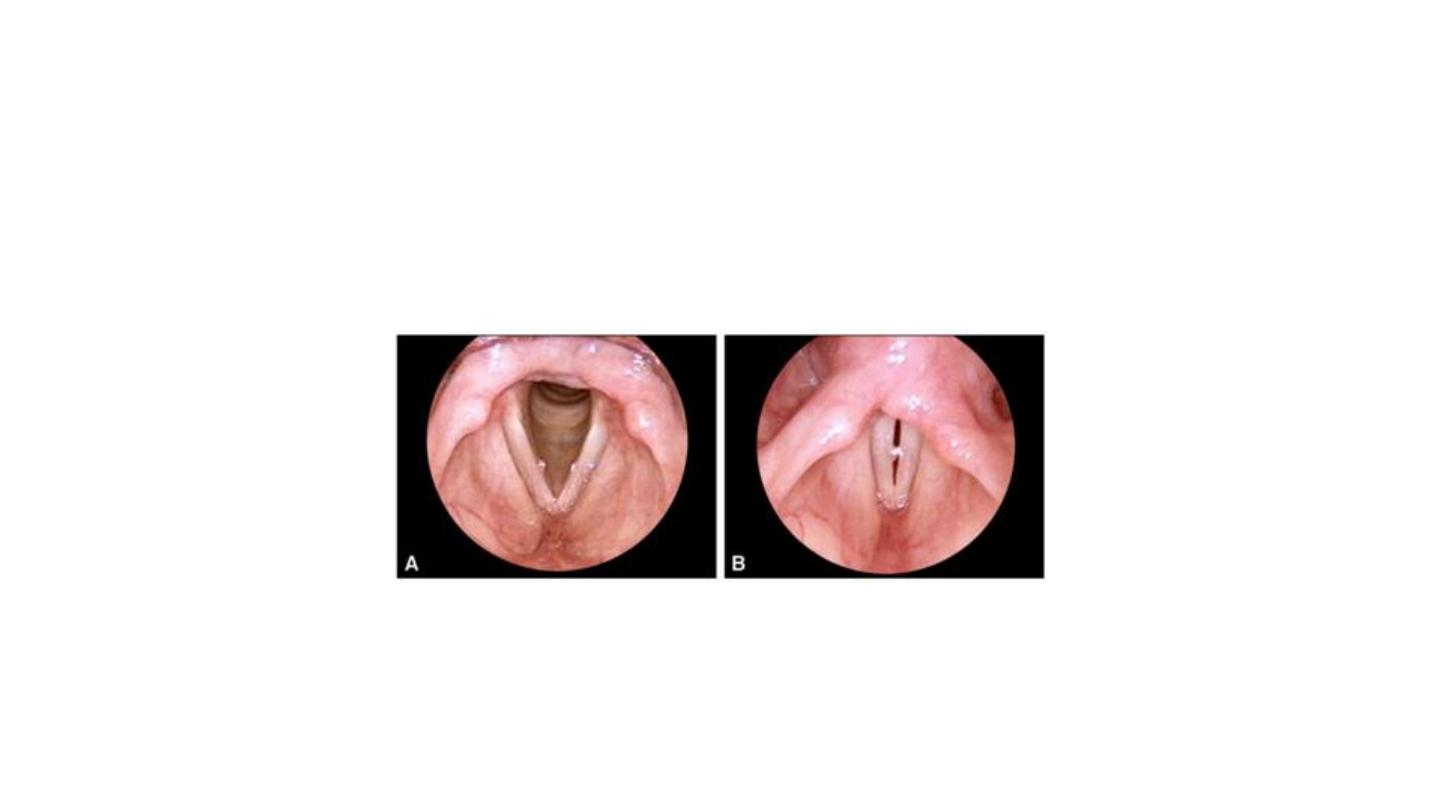
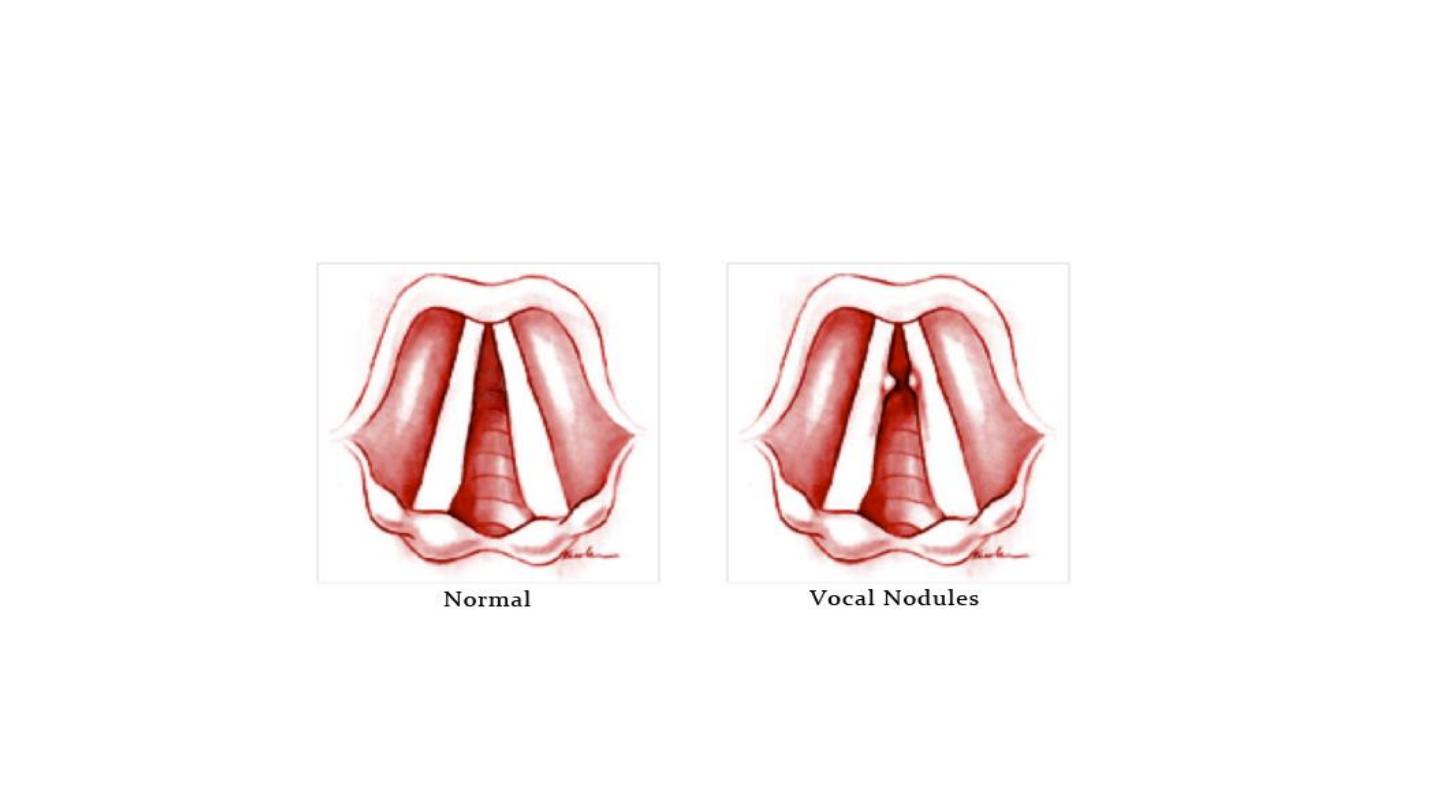
Vocal cord nodule (Singer's nodule):
It is due to misuse of voice and bad voice production common in school
children.teacher, singers and actors, often in the presence of
inflammation.
Pathology:
Localised hard thickening on the edge of each vocal cord at the junction of
anterior thirds and posterior two third of vocal cord,it is usually bilateral.
Clinical features
Hoarseness of voice, with voice fatigue
Dr.Safaa H. Alturaihy

Treatment
●
voice rest
●●
Removal of any inflammatory focus
●●●
Speech therapy often lead to resorption of
the nodules
●●●●
Finally, precise localised removal is
curative

The larynx is in a unique position in being a major component of the upper
respiratory tract and
also lying just anterior to the upper end of the digestive tract. It is therefore vulnerable
to various
causes of inflammation, not all of which are
infective.
Gastro-oesophageal reflux disease
(
GORD/GERD)
is now a well-defined clinical entity that is associated particularly with
posterior glottic and arytenoid inflammation. Inflammation affecting the vocal cords
can be induced by vocal
misuse/abuse, exposure to irritants and allergies. The larynx may also be affected by
chronic inflamatory noninfective conditions, such as sarcoidosis and Wegener's
granulomatosis.
Laryngeal infection can also occur as a rare complication of a neck space infection,
Such as parapharyngeal or retropharyngeal abscess and Ludwig's angina
Laryngitis

CLINICAL FEATURES OF ACUTE LARYNGEAL
INFECTION
The general clinical features that should be
sought from a patient with acute laryngeal
infection
include the following:
• change or loss of voice;
• difficulty in breathing/stridor;
• sore throat and otalgia;
• difficult or painful swallow;
• tender larynx with/without cervical
lymphadenopathy

ACUTE LARYNGITIS
Acute laryngitis is a common inflammatory
condition that affects the vocal folds and
supraglottis.
The usual cause is a virus associated with an
upper respiratory tract infection, but laryngitis may
also be secondary to infection of the tonsils or the
chest. Inhalation of dusts and fumes or
underlying allergy can induce laryngeal
inflammation and may facilitate the development of
acute
laryngeal infection.

Clinical features
Acute viral laryngitis is normally a self-limiting infection that resolves after a few
days.
Patients will have a rough, deep voice of variable pitch that often disappears in
mid-sentence and they may, on occasins become aphonic.
Voice changes are usually preceded by the symptoms of a common
cold and a sore throat.
Examination will show erythema and oedema of the vocal cords and there may be
excess secretion.
Changes can, however, be subtle and not nearly as bad as the symptoms may
suggest.
Bacterial superinfection will induce a more severe degree of laryngitis that may
persist and become chronic

Management
Acute laryngitis usually resolves completely over one to two weeks and
investigation is unnecessary.
Basic therapy includes vocal rest, avoidance of irritants and steam.
Antibiotic should be reserved for more sever forms of bacterial laryngitis,
persistent laryngeal inflammation,
or in specific patients who rely on their voice professionally.
Penicillin has no effect but erythromycin, which is active against Moraxella
catarrhalis, is associated with less vocal
disturbance and reduced coughing at one to two weeks but no other significant
effects. Residual
problems such as aphonia, hoarseness or throat discomfort sometimes occur but
the larynx may look sureprisingly normal.
The likely explanation is that the residual dysfunction is due to
persistent inflammation within the internal laryngeal
muscles.
Speech therapy is indicated if the problem persist

26
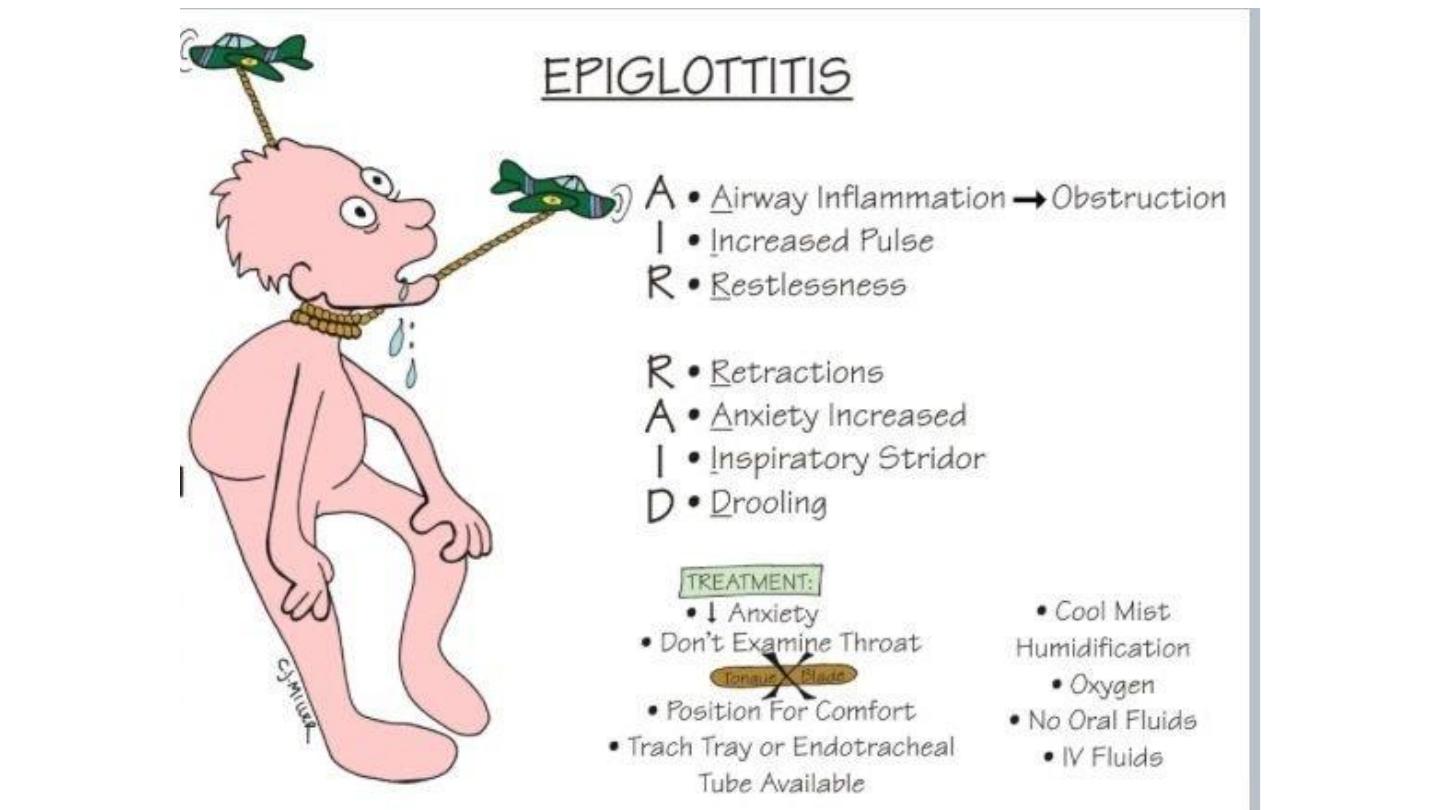
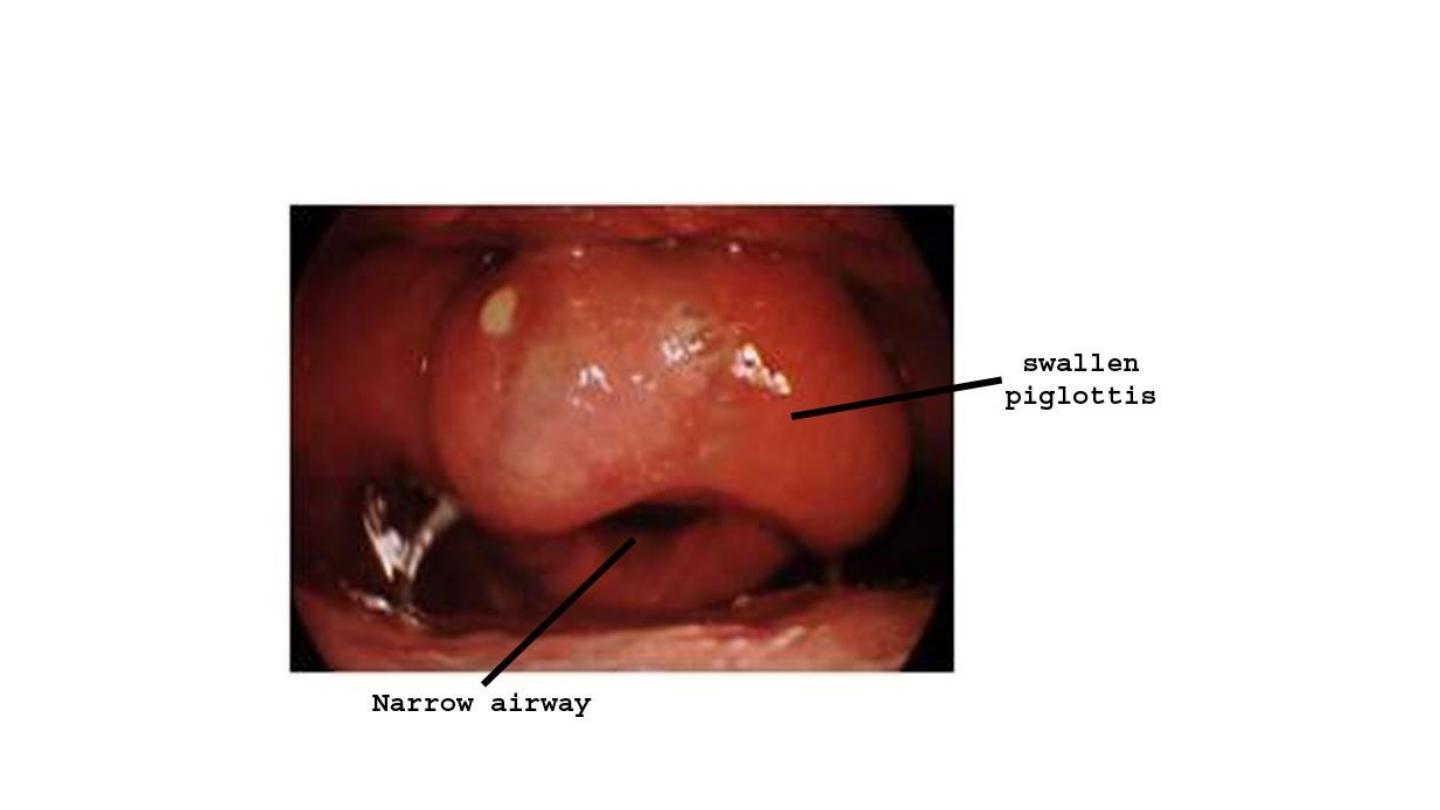
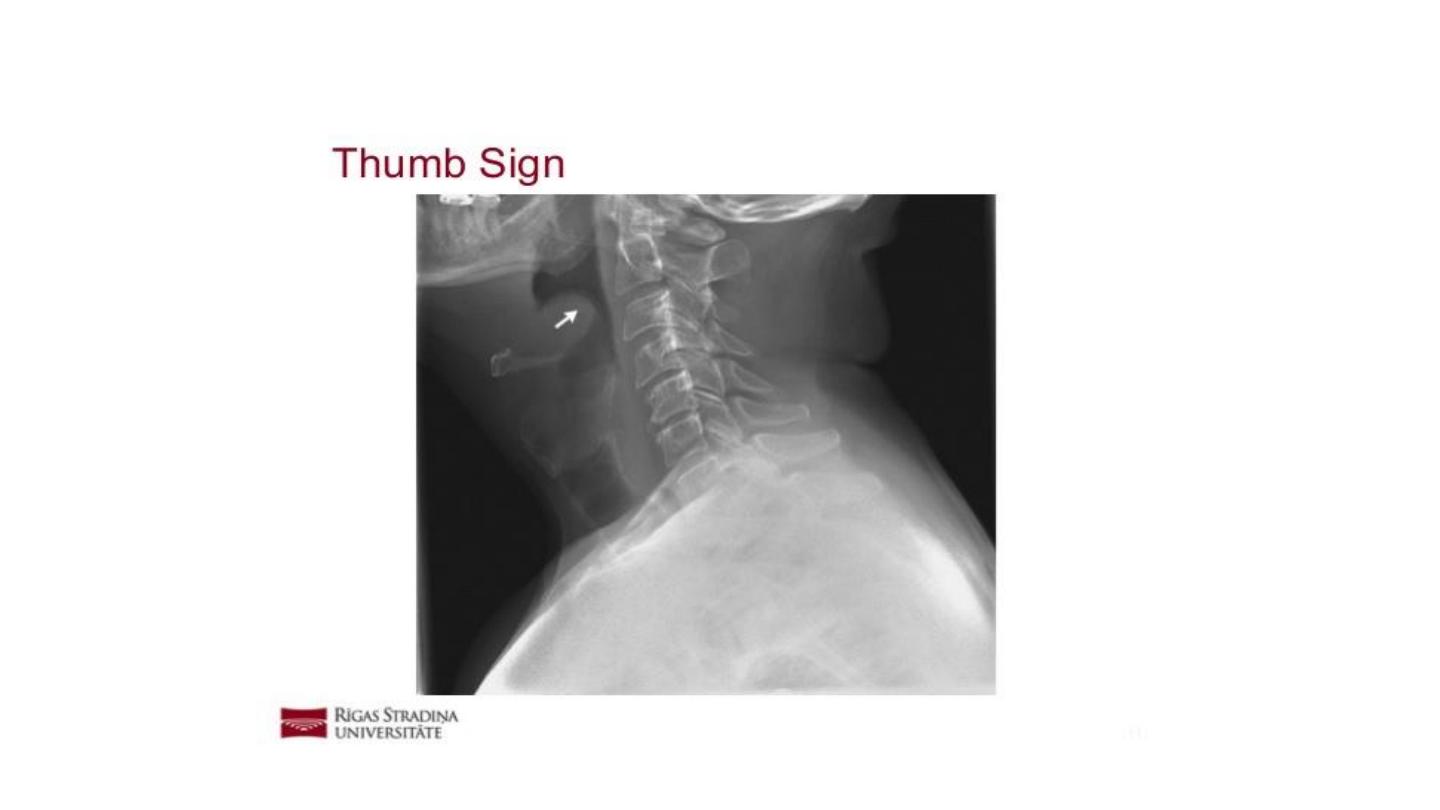
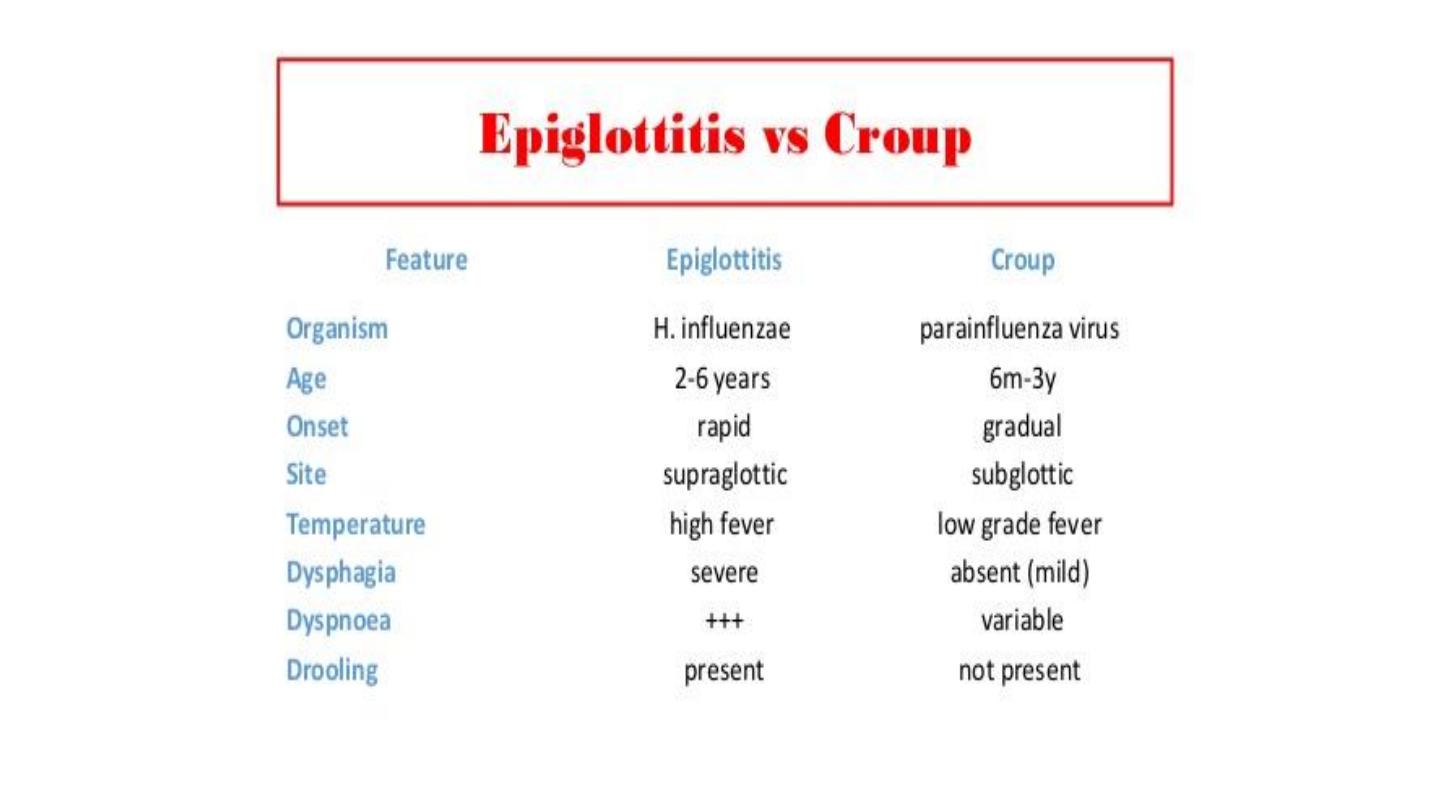
Acute epiglotitis:
A special form of acute laryngitis in which the inflammatory changes affect mainly the loosly attached
mucosa of the epiglottis.
Pathology:
Localised oedema may obstruct the airway,H.influenzae is usual causative organism
On examination:
Examination is diagnostic but may be delayed until the facilities for intubation and tracheostomy are
available so no attempts to depress the tongue or indirect laryngoscopy as this can cause laryngospasm.
Clinical features
:
1.Dyspnoea may be progressive and alarming especially in children in which lead to sever stridor and
death within few hours.
2. The child may be critically ill, toxic, flushed appearance, and high temperature (38-40)
Treatment
Admission to hospital
Establish the airway by passing endotrachial intubation
I.V line,fluid,sedation,AB
Swab and blood culture
Proper antibiotic(chloramphenicol(100mg\kg\24hours)as up to 30% of haemophilus strains are resistant to
penicilline,Third generation of cephalosporins are alternative because of side effect of chloramphenicol
Nasogastric tube should be inserted for feeding

30
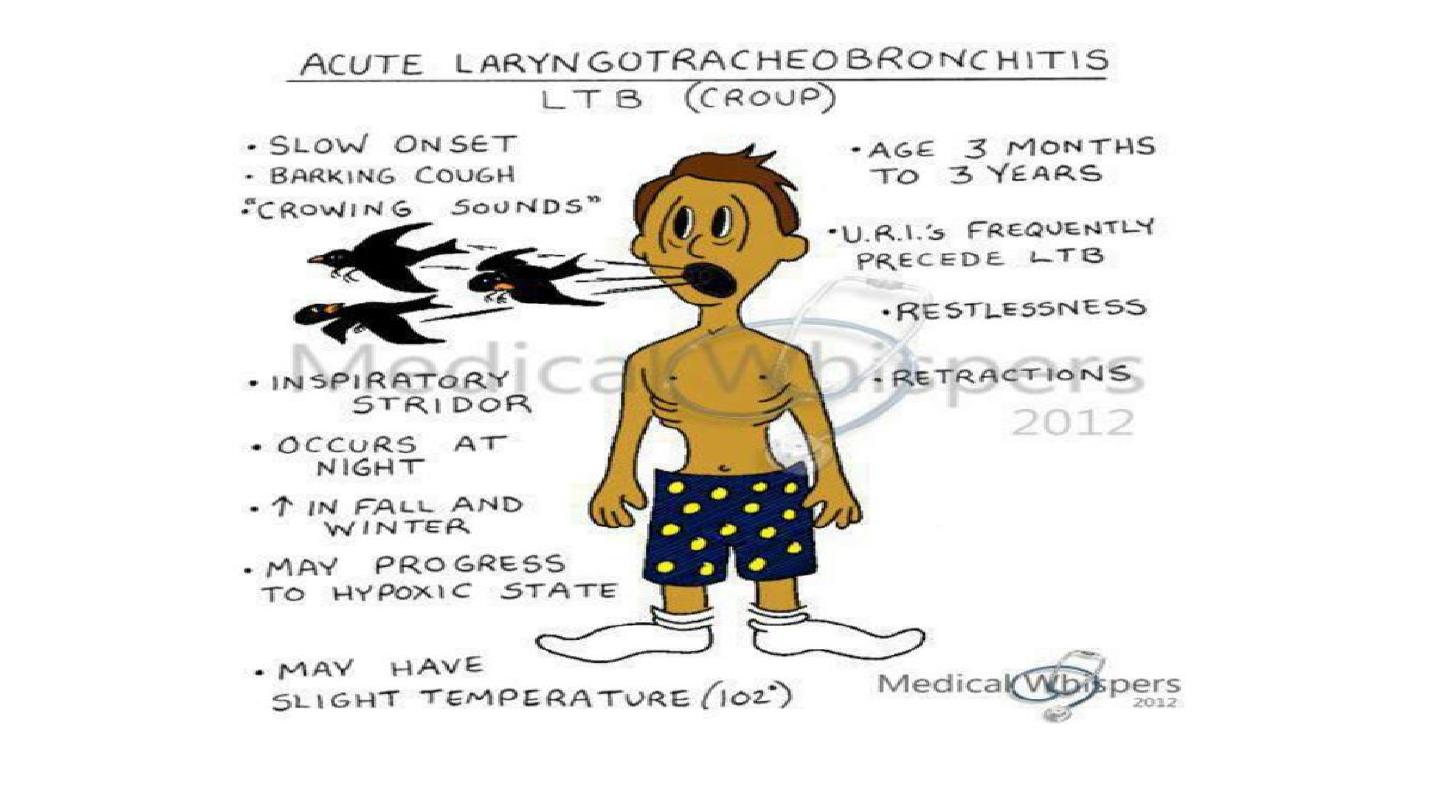
Acute laryngotracheobronchitis(croup)
It is less common dangerous than eiglottitis, it is usually viral infection by
parainfluenza virus type one. It occur in children under three years age, Its
onset is slow usually 48 hours after previous attach of URTI.It cause barking
cough,stridor,but no dysphagia ,the child is feverish,lying on
back,struggling,restlessness,horseness of voice, no drooling of saliva with
small cervical lymph nodes.
Treatment:
●observation
●●reassurance
●●●humidification
●●●●Oxygen with or without adrenaline, with or without steroid
●●●●●steroid
●●●●●●antibiotic for secondary bacterial infection

Turbulent flow due to partial obstruction of the airway gives rise to abnormal or
unwanted noise.
Obstruction of the small intra-thoracic airways, such as occurs in bronchial
asthma, is termed
wheezing
Noise originating in the larynx or trachea is typically high-pitched and termed
‘
stridor
’.
The low-pitched snoring type of noise made by naso- and oropharyngeal
obstruction is usually termed
stertor
This type of noise can occasionally be produced by the supraglottic larynx.
A rigid differentiation between stridor and stertor is not only artificial but can
wrongly limit the differential diagnosis
Stridor
Definition

ASSESSMENT
Stridor is the noise from a narrowed airway.
The aim of the history, Examination and special examinations is to
determine not only the site and cause of the obstruction (the
diagnosis) but also
its effect on the airway (the severity). It is important to consider the
effect of airway obstruction on feeding,sleep,execise and growth

Typically ,laryngomalacia is better with the child at rest and asleep
but made worse by crying, feeding and when the child is
distressed.
Airway obstruction with the baby supine can occur with a
pedunculated laryngeal mass but more often is due at least in part
to a degree
of supralaryngeal obstruction such as micrognathia and resultant
tongue base occlusion.
Improvement in the airway with crying occurs in gross nasal
obstruction such as bilateral choanal atresia.

36
Stridor
Stridor is the most common manifestation of paediatric airway disease. It is the audible
result of turbulent air flow in the larynx or trachea. Its phase during respiratory cycle and
its characteristics can help locate the site of an obstruction.
Supraglottic stridor is classically inspiratory.
Glottic or subglottic is biphasic.
Tracheal is expiratory.
Stridor must be distinguished from stertor, which is generated by pharyngeal obstruction.
Causes of stridor in children
◙Congenital anomalies:
●Laryngomalacia
●●Laryngeal web
●●●Laryngeal cysts
●●●●Subglottic stenosis
●●●●●Vascular ring
●●●●●●Congenital laryngeal tumours as haemangioma
◙

37
◙Acquired causes of stridor
●Foreign body
●●Trauma
●●●inflammatory causes:
1.Acute laryngitis
2.Acute Epiglottitis
3.Acute laryngotracheobronchitis
4.Tumour as benign multiple laryngeal papilloma
5. Neurogenic diseases as bilateral vocal cord palsy
6.spasmodic laryngitis