Roseola (Human Herpesviruses 6 and 7)
Human herpesvirus 6 (HHV-6A and HHV-6B) and human herpesvirus 7 (HHV7)
cause infection in infancy and early
childhood. HHV-6B is responsible for the
majority of cases of roseola infantum (exanthema subitum or sixth disease) and is
associated
with
other
diseases,
including
encephalitis,
especially
in
immunocompromised
hosts. A small percentage of children with
roseola
have
primary infection with HHV-7.
Epidemiology:
Primary infection with HHV-6B is acquired rapidly by essentially all children
following the loss of maternal antibodies in the 1st few mo of infancy, 95% of children
being infected with HHV-6 by 2 yr of age. The peak age of primary HHV-6B infection
is 6-9 mo of life, with infections occurring sporadically and without seasonal
predilection or contact with other ill individuals.
Primary infection is presumed to be spread by the saliva of asymptomatic individuals.
Pathology/ Pathogenesis:
HHV-6 has a recognizable cytopathic effect, consisting of the appearance of large
refractile mononucleated or multinucleated cells with intracytoplasmic and/or
intranuclear inclusions. Primary infection with HHV-6 and HHV-7 is followed by
lifelong latency or persistence of virus at multiple sites. HHV-6 exists in a true state of
viral latency in monocytes and macrophages.
Clinical Manifestation:
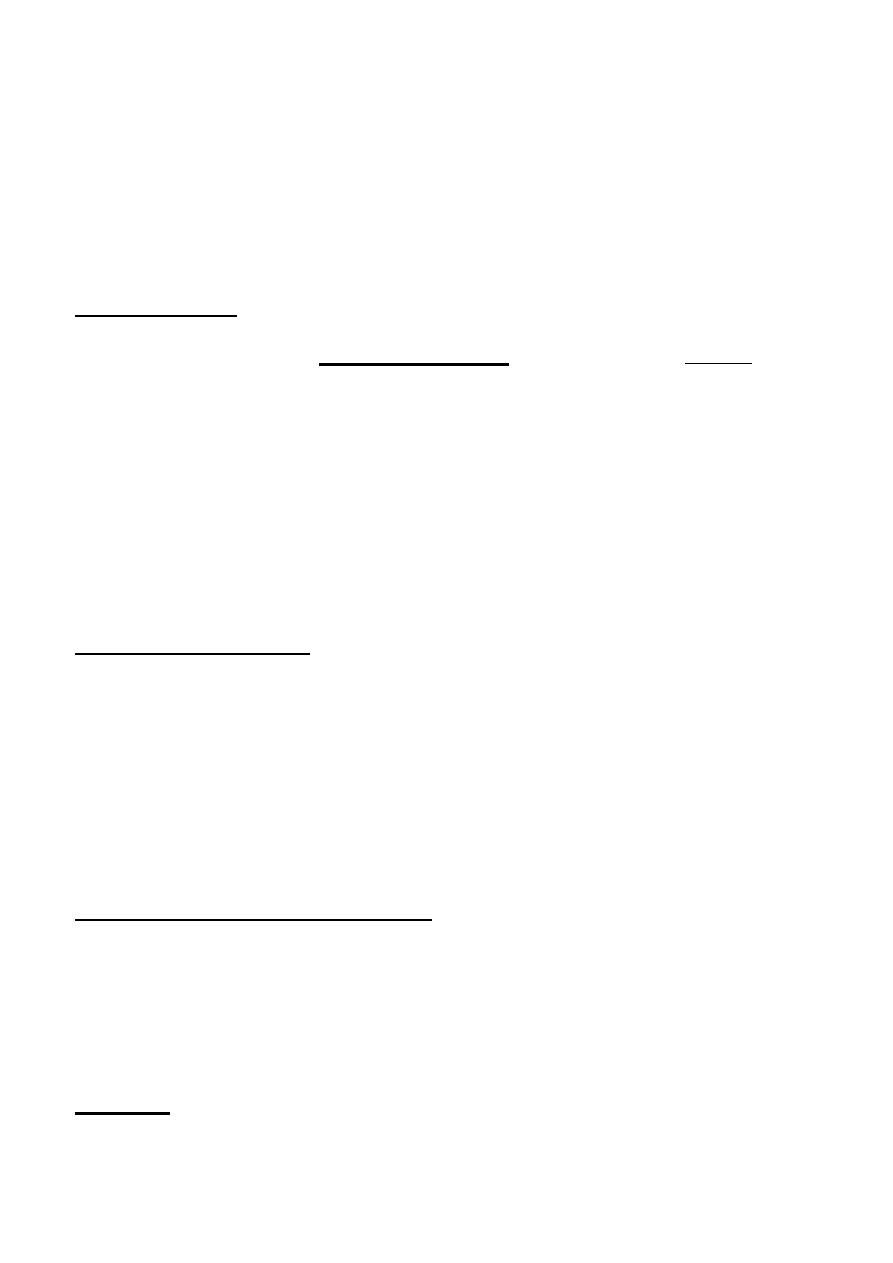
Roseola infantum (exanthem subitum, or sixth disease) is an acute, self-limited disease
of infancy and early childhood. It is characterized by the abrupt onset of high fever,
which may be accompanied by fussiness. The fever usually resolves acutely after 72 hr
(“crisis”) but may gradually fade over a day (“lysis”) coincident with the appearance
of a faint pink or rose-colored, nonpruritic, 2-3 mm morbilliform rash on the trunk.
The rash usually lasts 1-3 days but is often described as evanescent and may be visible
only for hours, spreading from the trunk to the face and extremities. Because the rash
is variable in appearance, location, and duration, it is not distinctive.
Associated signs are few but can include mild injection of the pharynx, palpebral
conjunctivae, or tympanic membranes and enlarged suboccipital nodes. In Asian
countries, ulcers at the uvulopalatoglossal junction (Nagayama spots) are commonly
reported in infants with roseola. High fever (mean: 39.7°C [103.5°F]) is the most
consistent finding associated with primary HHV-6B infection. Additional symptoms
and signs include irritability, inflamed tympanic membranes, rhinorrhea and
congestion, gastrointestinal complaints, and encephalopathy. The mean duration of
illness caused by primary HHV-6B infection is 6days, with 15% of children having
fever for 6 or more days.
Much less is known about the clinical manifestations of
HHV-7 infection. Primary infection with HHV-7 has been identified in a small number
of children with roseola in whom the illness is indistinguishable from that caused by
HHV-6B.
Laboratory Findings:
*Low mean WBC count.
*Thrombocytopenia, elevated serum transaminase values, and atypical lymphocytes.
*CSF: normal or only minimal CSF pleocytosis with mildly elevated protein.
Diagnosis:
1.A history of 3 days of high fever in an otherwise nontoxic 10 mo old infant with a
blanching maculopapular rash on the trunk suggests a diagnosis of roseola. Likewise, a
specific diagnosis of HHV-6 is not usually necessary except in situations in which the
manifestations of the infection are severe or unusual and might benefit from antiviral
therapy.
2.Viral culture is the gold standard method to document active viral
replication(expensive, time-consuming, and available only in research lab.).
3. Detection of viral DNA by PCR on acellular fluids such as plasma or reverse
transcriptase PCR on peripheral blood mononuclear cell samples.
Differential Diagnosis:
+Rubella
+Mumps
+Scarlet fever
+Enterovirus
+Drug hypersensitivity reactions.
Complications:
1. Convulsions (the most common, 1/3 of patients)
2. Partial seizures, prolonged seizures, postictal paralysis, and repeated seizures.
3. Encephalitis, acute disseminated demyelination, autoimmune encephalitis,
cerebellitis.
4. Hepatitis, and myocarditis
5. Reactivation esp. in imunocompromised.
Treatment:
• Supportive care is usually all that is needed for infants with roseola.(
hydration
and may use antipyretics if the child is especially uncomfortable with the fever).
• Specific antiviral therapy is not recommended for routine cases of primary
HHV-6B or HHV-7 infection.
• Unusual or severe manifestations of primary or presumed reactivated HHV-6B
infection such as encephalitis, especially in immunocompromised patients, may
benefit from treatment (Ganciclovir, foscarnet, and cidofovir).
Prognosis:
❖ Roseola is generally a self-limited illness associated with complete recovery.
❖ Although seizures are a common complication of primary infection with HHV-
6B and HHV-7, the risk of recurrent seizures does not appear to be higher than
that associated with other causes of simple febrile seizures.
Prevention:
Primary infections with HHV-6 and HHV-7 are widespread throughout the human
population with no current means of interrupting transmission.
Epstein-Barr virus (Infectious Mononucleosis) (IMN):
It is characterized by systemic somatic complaints consisting primarily of fatigue,
malaise, fever, sore throat, and generalized lymphadenopathy. Originally described as
glandular fever, it derives its name from the mononuclear lymphocytosis with
atypical-appearing lymphocytes that accompany the illness. Other infections may
cause infectious mononucleosis-like illnesses.
Etiology:
EBV is a double-stranded DNA virus that causes >90% of cases of infectious
mononucleosis. Two distinct types of EBV, type 1 and type 2. Both types lead to
persistent, lifelong, latent infection.
As many as 5-10% of infectious mononucleosis–like illnesses are caused by primary
infection with cytomegalovirus, Toxoplasma gondii, adenovirus, hepatitis virus,
primary HIV, and possibly rubella virus. In the majority of EBV-negative infectious
mononucleosis-like illnesses, the exact cause remains unknown.
Epidemiology:
EBV infects more than 95% of the world’s population. Among children, transmission
may occur by exchange of saliva from child to child, such as occurs between children
in out-of-home childcare. Nonintimate contact, environmental sources, or fomites do
not contribute to spread of EBV.
EBV is shed in oral secretions consistently for more than 6 mo after acute infection
and then intermittently for life.
Infection with EBV in developing countries and among socioeconomically
disadvantaged populations of developed countries usually occurs during infancy and
early childhood. Large differences are seen by family income, with highest
seroprevalence in children of families with lowest income.
The epidemiology of the illness of infectious mononucleosis is related to the age of
acquisition of EBV infection. Primary infection with EBV during childhood is usually
asymptomatic or mild and indistinguishable from other childhood infections.
Primary EBV infection in adolescents and adults manifests in 30-50% of cases as the
classic triad of fatigue, pharyngitis, and generalized lymphadenopathy, which
constitute the major clinical manifestations of infectious mononucleosis. This
syndrome may be seen at all ages but is rarely apparent in children younger than 4 yr
of age, when most EBV infections are asymptomatic.
Pathogenesis:
After acquisition in the oral cavity, EBV initially infects crypt epithelial cells, which
may contribute to the symptoms of pharyngitis. After intracellular viral replication and
cell lysis with release of new virions, virus spreads to contiguous structures such as the
salivary glands, with eventual viremia and infection of B lymphocytes in the peripheral
blood and the entire lymphoreticular system, including the liver and spleen. The
atypical lymphocytes that are characteristic of infectious mononucleosis are CD8 T
lymphocytes.
EBV, like the other herpesviruses, establishes lifelong latent infection after the primary
illness. The latent virus is carried in oropharyngeal epithelial cells and systemically in
memory B lymphocytes as multiple episomes in the nucleus. Reactivation is
apparently asymptomatic and not recognized to be accompanied by distinctive clinical
symptoms.
Oncogenesis:
Benign EBV-associated proliferations include:
❖ oral hairy leukoplakia, primarily in adults with AIDS,
❖ lymphoid interstitial pneumonitis, primarily in children with AIDS.
Malignant EBVassociated proliferations include:
➢ nasopharyngeal carcinoma,
➢ Burkitt lymphoma,
➢ Hodgkin disease,
➢ lymphoproliferative disorders,
➢ leiomyosarcoma in immunodeficient states, including AIDS.
Clinical Manifestations:
The incubation period of IMN in adolescents is 30-50 days. In children, it may be
shorter. The majority of cases of primary EBV infection in infants and young children
are clinically silent. Patients may complain of malaise, fatigue, acute or prolonged (>1
wk) fever, headache, sore throat, nausea, abdominal pain, and myalgia. This prodromal
period may last 1-2 wk.
The complaints of sore throat and fever gradually increase until patients seek medical
care. Splenic enlargement may be rapid enough to cause left upper quadrant abdominal
discomfort and tenderness, which may be the presenting complaint. The classic
physical examination findings are generalized lymphadenopathy (90% of cases),
splenomegaly (50% of cases), and hepatomegaly (10% of cases). LAP occurs most
commonly in the anterior and posterior cervical nodes and the submandibular lymph
nodes and less commonly in the axillary and inguinal lymph nodes. Epitrochlear
lymphadenopathy is particularly suggestive of IMN. Symptomatic hepatitis or jaundice
is uncommon, but elevated liver enzymes are very common.
Splenomegaly to 2-3 cm below the costal margin is typical (15-65% of cases) and is
seen in most cases by ultrasonography; massive enlargement is uncommon.
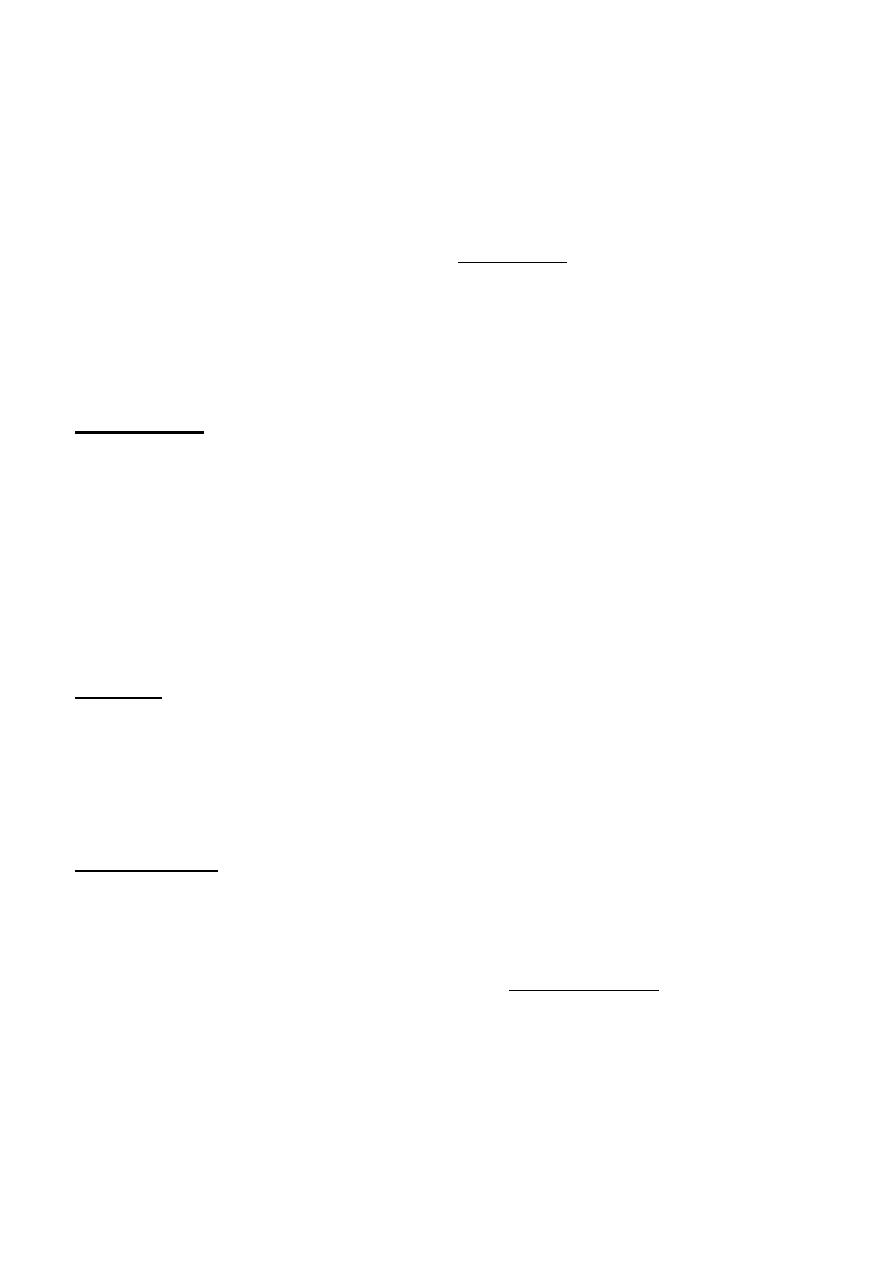
The sore throat is often accompanied by moderate to severe pharyngitis with marked
tonsillar enlargement, occasionally with exudates. Palatal petechiae at the junction of
the hard and soft palate are frequently seen. The pharyngitis resembles that caused by
streptococcal infection. Other clinical findings may include rashes and edema of the
eyelids.
Rashes are usually maculopapular and have been reported in 3-15% of patients.
Patients with IMN treated with ampicillin or amoxicillin may experience “ampicillin
rash,” which may occur with other β-lactam antibiotics. This morbilliform, vasculitic
rash is probably immune mediated and resolves without specific treatment.
Infants coinfected with HIV acquire EBV infection at an earlier age, have higher EBV
plasma loads that are slower to resolve, and more frequently develop pneumonia and
hepatosplenomegaly and require hospitalization compared to HIV-negative infants.
Diagnosis:
The diagnosis of IMN implies primary EBV infection. A presumptive diagnosis may
be made by the presence of typical clinical symptoms with atypical lymphocytosis in
the peripheral blood. The diagnosis is usually confirmed by serologic testing, either for
heterophile antibody or specific EBV antibodies. Culture of EBV is tedious and
requires 4-6 wk.
Differential Diagnosis:
• Infectious mononucleosis-like illnesses may be caused by primary infection with
cytomegalovirus, T. gondii, adenovirus, hepatitis virus, HIV, or possibly rubella
virus.
• Streptococcal pharyngitis may cause sore throat and cervical lymphadenopathy
indistinguishable from that of infectious mononucleosis but is not associated
with hepatosplenomegaly.
• Leukemia(esp. if extremely high or low white blood cell counts, moderate
thrombocytopenia, and even hemolytic anemia).
Laboratory Tests:
In >90% of cases there is leukocytosis of 10,000-20,000 cells/µL, of which at least
two thirds are lymphocytes; atypical lymphocytes usually account for 20-40% of the
total number (mature T lymphocytes that are larger overall, with larger, eccentrically
placed indented and folded nuclei with a lower nuclear-to-cytoplasm ratio).
Atypical lymphocytosis may be seen with many infections usually causing
lymphocytosis other than EBV including: acquired cytomegalovirus infection (in
contrast to congenital cytomegalovirus infection), toxoplasmosis, viral hepatitis,
rubella, roseola, mumps, tuberculosis, typhoid, Mycoplasma infection, and malaria, as
well as some drug reactions.
Mild thrombocytopenia to 50,000-200,000 platelets/µL occurs in more than 50% of
patients, but only rarely is associated with purpura.
Mild elevation of hepatic transaminases occurs in approximately 50% of
uncomplicated cases, but is usually asymptomatic without jaundice.
HeterophileAntibodyTest:
Heterophile antibodies agglutinate cells from species different from those in the source
serum. The transient heterophile antibodies seen in infectious mononucleosis, also
known as Paul-Bunnell antibodies, are IgM antibodies detected by the Paul-Bunnell
Davidsohn test for sheep red cell agglutination. The heterophile antibodies of
infectious mononucleosis agglutinate sheep or, for greater sensitivity, horse red cells.
Heterophile antibody tests are positive in 75% of cases in the 1st wk and 90-95% of
cases in the 2nd wk. The most widely used method is the qualitative rapid slide test
using horse erythrocytes.
If the heterophile test result is negative and an EBV infection is suspected, EBV-
specific antibody testing is indicated.
Specific Epstein-Barr Virus Antibodies:
EBV-specific antibody testing is useful to confirm acute EBV infection, especially in
heterophile-negative cases, or to confirm past infection and determine susceptibility to
future infection. The EBNA, EA, and VCA antigen systems are most useful for
diagnostic purposes.
The detection of IgM antibody to VCA is the most valuable and specific serologic test
for the diagnosis of acute EBV infection and is generally sufficient to confirm the
diagnosis.
Treatment:
▪ There is no specific treatment for infectious mononucleosis.
▪ The mainstays of management are rest, encouraging adequate fluid and
nutrition intake, and symptomatic treatment with acetaminophen or
nonsteroidal antiinflammatory agents to manage fever, throat discomfort, and
malaise.
▪ Bed rest is necessary only when the patient has debilitating fatigue.
▪ Advise against participation in contact sports and strenuous athletic activities
during the 1st 2-3 wk of illness or while splenomegaly is present because blunt
abdominal trauma may predispose patients to splenic rupture.
▪ Corticosteroids: short course(<2wk) prednisolone 1 mg/kg/day or equivalent
for 7 days and tapered over another 7 days, indicated in:
o airway obstruction,
o thrombocytopenia with hemorrhaging,
o autoimmune hemolytic anemia,
o seizures, and meningitis.
▪ Antiviral therapy is not recommended.
Complications:
1. Subcapsular splenic haemorrhage or splenic rupture.
2. 2. Airway obstruction.
3. Neurological manifestations ( headache, seizures, ataxia, meningitis, facial
nerve palsy, transverse myelitis, and encephalitis).
4. Alice-inWonderland syndrome (metamorphopsia)(perceptual distortions of
sizes, shapes, and spatial relationships).
5. Guillain-Barre or Reye syndrome.
6. Hemolytic anemia, aplastic anemia, mild thrombocytopenia, or severe
neutropenia.
7. Myocarditis, interstitial pneumonia, pancreatitis, parotitis, and orchitis.
Prognosis:
The prognosis for complete recovery is excellent. The major symptoms typically last
2-4 wk followed by gradual recovery within 2 mo of onset of symptoms. Cervical
lymphadenopathy and fatigue may resolve more slowly. Prolonged and debilitating
fatigue, malaise, and some disability that may wax and wane for several weeks to 6 mo
are common complaints even in otherwise unremarkable cases.
Scarlet Fever:
Scarlet fever is an upper respiratory tract infection associated with a characteristic
rash, which is caused by an infection with pyrogenic exotoxin (erythrogenic toxin)–
producing in individuals who do not have antitoxin antibodies. GAS can produce up to
12 different pyrogenic exotoxins, and repeat attacks of scarlet fever are possible.
It is most common in children 5-15 yr old. The incubation period ranges from 1-7
days, with an average of 3 days. The onset is acute and is characterized by fever,
vomiting, headache, toxicity, pharyngitis, LAP, and chills. Abdominal pain may be
present; when this is associated with vomiting before the appearance of the rash, an
abdominal surgical condition may be suggested.
The rash appears within 24-48 hr after onset of symptoms, although it may appear with
the first signs of illness. It often begins around the neck and spreads over the trunk and
extremities. The rash is a diffuse, finely papular, erythematous eruption producing
bright red discoloration of the skin, which blanches on pressure. It is often accentuated
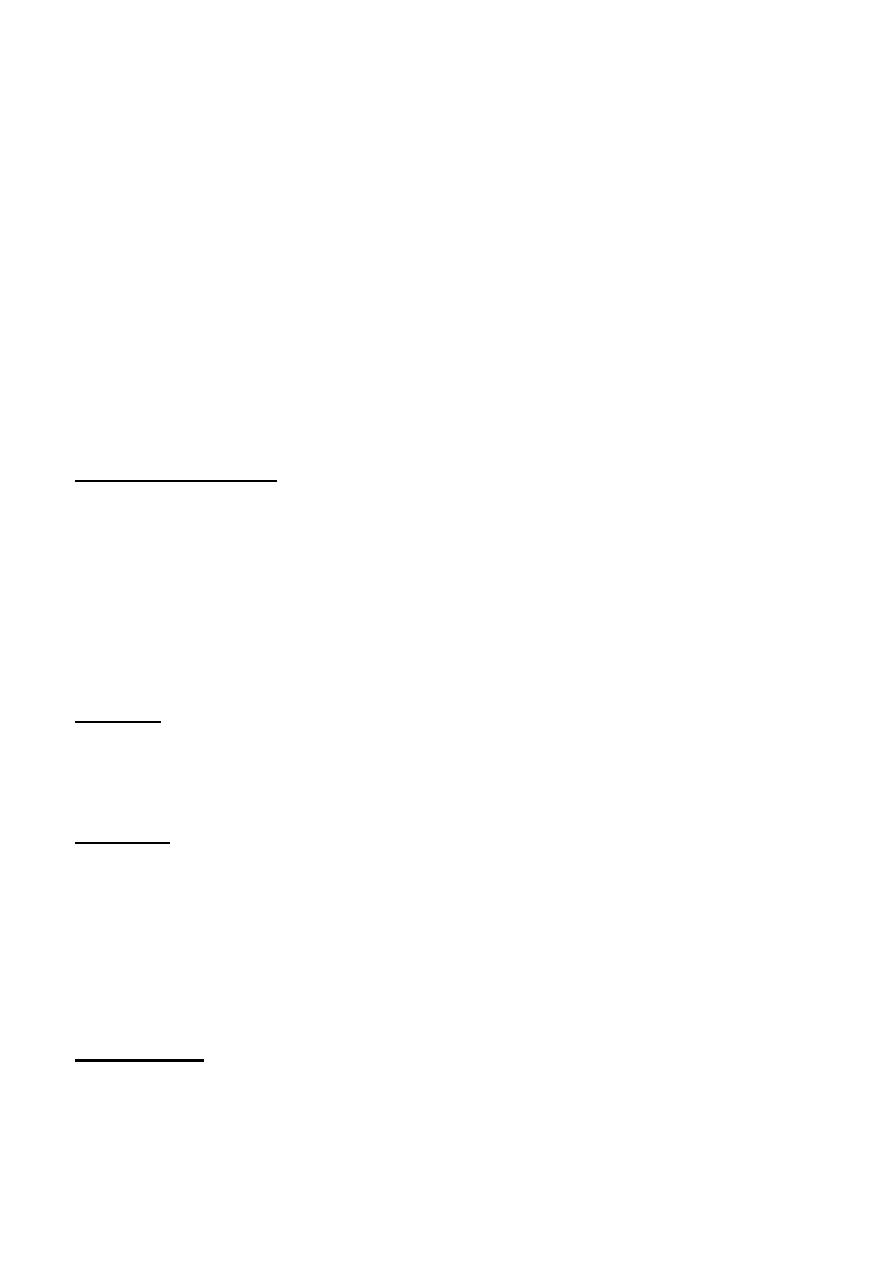
in the creases of the elbows, axillae, and groin. The skin has a goose-pimple
appearance and feels rough. The cheeks are often erythematous with pallor around the
mouth( circumoral pallor).
Generally, temperature increases abruptly, may peak at 39.6-40°C (103-104°F) on the
2nd day, and gradually returns to normal within 5-7 days in untreated patients; it is
usually normal within 12-24 hr after initiation of penicillin therapy. The tonsils are
hyperemic and edematous and may be covered with a gray-white exudate. The
pharynx is inflamed and covered by a membrane in severe cases. The tongue may be
edematous and reddened.
After 3-4 days, the rash begins to fade and is followed by desquamation, initially on
the face, progressing downward, and often resembling a mild sunburn. Occasionally,
sheet-like desquamation may occur around the free margins of the fingernails, the
palms, and the soles.
The tongue is usually coated and the papillae are swollen. After desquamation, the
reddened papillae are prominent, giving the tongue a strawberry appearance.
Differential Diagnosis:
+ Measles,
+ Rubella,
+ Roseola
+ IMN
+ Enteroviruses
+ Kawasaki disease,
+ Drug eruptions.
+Staphylococcal infections TSS(are occasionally associated with a scarlatiniform
rash).
Diagnosis:
The presentation of scarlet fever can be diagnosed clinically, further testing can be
used to confirm the diagnosis:
1. Culture of throat swab on sheep blood agar plate.
2. Rapid antigen detection test.
Treatment:
GAS is exquisitely sensitive to penicillin and cephalosporins, and resistant strains have
never been encountered. Penicillin or amoxicillin is therefore the drug of choice
(except in patients who are allergic to penicillins) for pharyngeal infections as well as
for suppurative complications.
[Oral penicillin V for 10 days, or a single i.m benzathine penicillin G, or amoxicillin
for 10 days, or cephalosporin for 10 days is the treatment].
For penicillin-allergic petients: oral clindamycin for 10 days, erythromycin or
clarithromycin for 10 days, or azithromycin for 5 days.
Complications:
Suppurative complications from the spread of GAS to adjacent structures were
extremely common in the preantibiotic era. Cervical lymphadenitis, peritonsillar
abscess, retropharyngeal abscess, otitis media, mastoiditis, and sinusitis still occur in
children in whom the primary illness has gone unnoticed or in whom treatment of the
pharyngitis has been inadequate. GAS pneumonia can also occur.

Acute rheumatic fever and acute poststreptococcal glomerulonephritis are both
nonsuppurative sequelae of infections with GAS that occur after an asymptomatic
latent period.