Hair Problems (2)
Excessive Hair Growth
Growth of hairs that are longer, thicker or more numerous than the location, age, and racial background of the patient would predict.Hirsutism
Hypertrichosis
Hirsutism
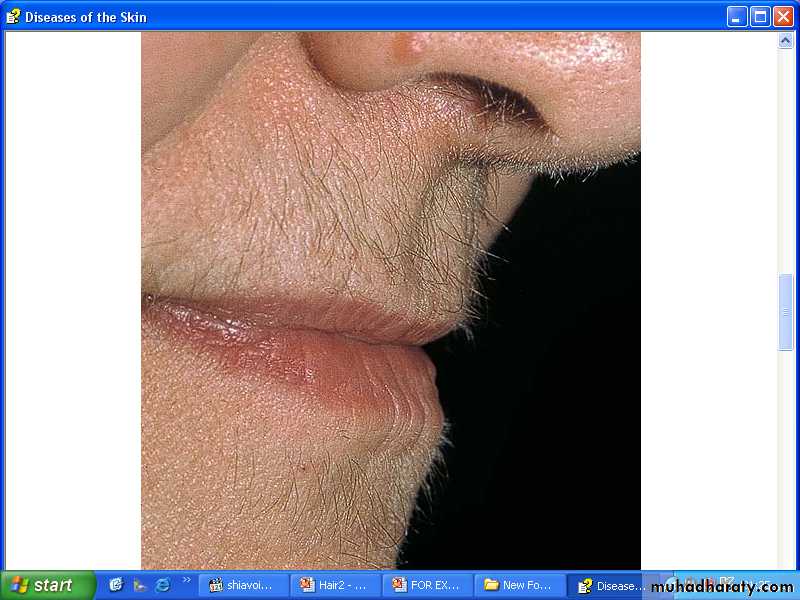
Increased growth of terminal hairs in androgen-dependent areas, producing male-like hair growth in women.It is a common problem among Iraqi females.
Family history is positive in third of cases.
Androgen dependent areas are chin , sides of face, moustache , neck , chest , breast especially around the nipples , upper back and shoulders, linea alba above the umbilicus.Virilization is the association of hirsutism with other signs of male development.
Causes:
1-Physiologic:Some degree of hirsutism may be a racial or familial trait constituting most cases of hirsutism.
Minor facial hirsutism is common after the menopause
2-Idiopathic:some patients without a family background of hirsutism become hirsute in the absence of any demonstrable hormonal cause.
Probable indemonstrable causes are:
A-Minor ovarian or adrenal dysfunction,B-Local increased 5-α reductase activity, or
C-Increased number of androgen receptors at hair follicles.
D-Increased sensitivity of androgen receptors at hair follicles.
Causes:
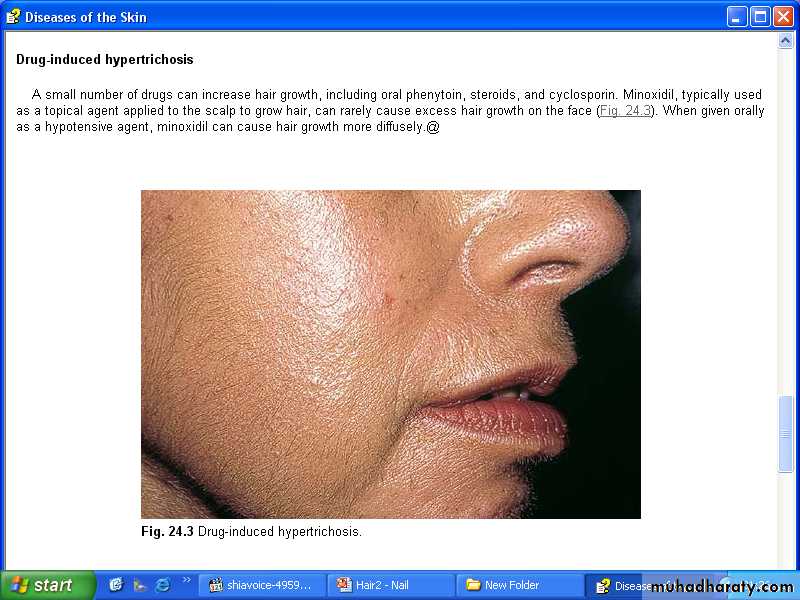
3-Iatrogenic:Phenytoin, androgens, corticosteroids, contraceptives (progesterone has androgen action)
4-Symptomatic:
Some patients with hirsutism will have one of the following disordersA- Ovarian: Polycystic ovary disease, virilizing tumors.
B- Adrenal: Congenital adrenal hyperplasia,virilizing tumors.
C- Pituitary: Cushing disease, acromegaly, prolactinoma
D-Ectopic virilizing broncogenic or GIT carcinomas.
Investigations
Women with a normal menstrual cycle and no signs of virilization are unlikely to have a significant endocrine cause for their hirsutism.investigation is needed if these symptoms are present.
Therapy
Often unsatisfactory and needs continuous use, usually with relapse after treatment discontinuation.A-Treat underlying disease.
B-Removal of hairs:
1-Shaving, wax epilation, chemical epilation (thioglycolate commercial products).2-Bleaching (6–10% hydrogen peroxide in water).
3-Destruction of individual hair follicles by electrolysis or thermolysis.
4-Epilation with lasers or intense pulsed light source;
much faster and more effective.5-Eflornithine (topical) effective but only as long as used;
also expensive.
C-Systemic therapy:
1-Primary antiandrogen: Flutamide, Cyproterone acetate.2-Agents with secondary antiandrogen activity:Spironolactone.
3-GRH agonists: leoprolide and nafarelin.
4- 5-α-Reductase inhibitor: Finasteride 2.5-5 mg daily.
5-Combination therapy.
Hypertrichosis
Excessive growth of terminal hair that does not follow an androgen-dependant pattern.A- Hypertrichosis lanuginosa
1-Hypertrichosis lanuginosa congenita:Uncommon genodermatosis in which newborn is covered by long lanugo hairs, which are not shed and replaced, but continue to grow. Patient typically winds up with a silvery coat of 10 cm long hairs.
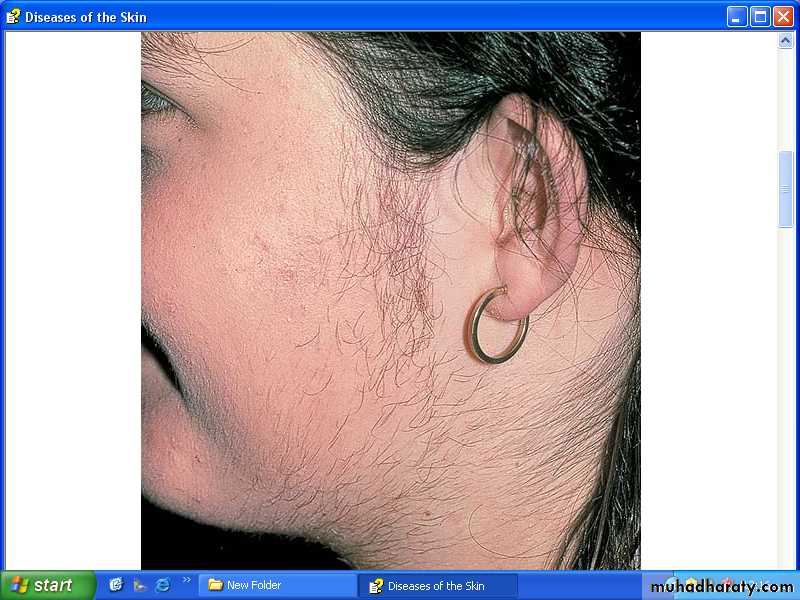
2-Hypertrichosis lanuginosa acquisita:
The sudden profuse covering of the skin by white lanugo hairs is a reliable marker of internal malignancy (e.g. lung, colon, or breast, as well as others)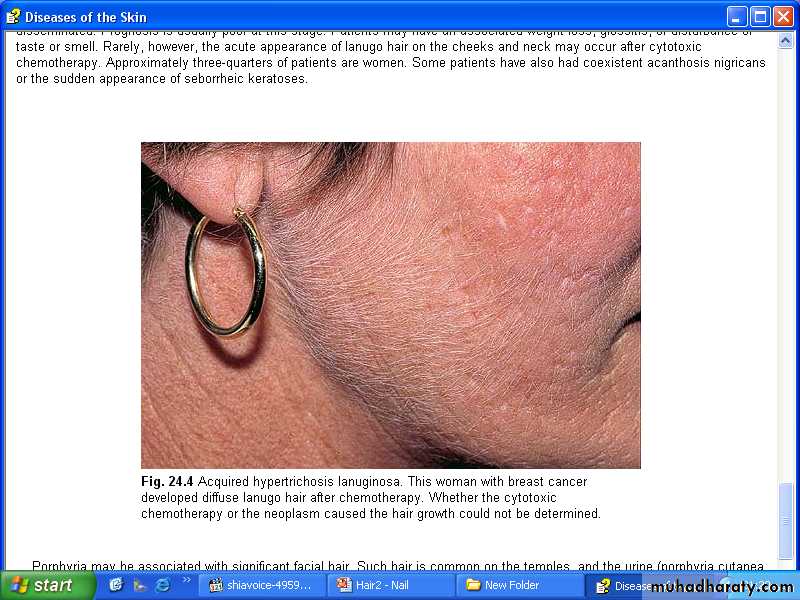
B- Generalized Hypertrichosis
The entire body seems affected with regional differences. There are many causes for diffuse excess numbers of terminal hairs:1-Hereditary: Porphyria cutanea tarda, mucopolysaccharidoses, chromosome abnormalities (trisomy 18).
2-Endocrine: Pituitary and thyroid disorders.
3-Eating disorders: (especially anorexia nervosa), malabsorption, fetal alcohol syndrome.
4-Medications: Cyclosporine, minoxidil, phenytoin are most common
C- Localized (nevoid) hypertrichosis
1-Becker nevus: Localized mosaic area of increased melanin and increased hair growth.
2- Faun tail nevus: Localized hair growth over sacrum;
a serious marker for potential underlying spinal cord defects or spina bifida. Neurological and radiological work-up mandatory.
3-Hair nevus: localized area with excess hair follicles and no other abnormalities; Uncommon.
