1
Ophthalmology
Dr. Muataz Hasan
Strabismus (Squint)
Anatomy of extraocular muscles:
They are four recti, two oblique's and levator palpebrae superioris. Recti origin is in
the apex of the orbit from a fibrous ring called "Annulus of Zinn" which surrounds
the optic nerve.
The recti muscles:
- Medial rectus: originates from the medial side of the annulus to be inserted on the
medial side of the eyeball 5.5 mm posterior to the limbus.
- Inferior rectus: originates from the inferior surface of the annulus to be inserted
on the inferior surface of the eyeball 6.5 mm posterior to the limbus.
- Lateral rectus: originates from the lateral side of the annulus to be inserted on the
lateral side of the eyeball 6.9 mm posterior to the limbus.
- Superior rectus: originates from the superior surface of the annulus to be inserted
on the superior surface of the eyeball 7.5 mm posterior to the limbus.
* The insertions of all muscles are anterior to equator and covered by tenon's
capsule and conjunctiva, so we cannot see them externally.
Innervations of the recti:
Medial, inferior and superior recti are innervated by oculomotor nerve.
The lateral rectus is innervated by abducent nerve.
Action:
- Medial rectus: Adduction.
- Lateral rectus: Abduction.
- Superior rectus: elevation (primary action) and intortion (2
nd
action) in primary
position of the eye. It is pure elevator in abduction and pure intorter in adduction.
- Inferior rectus: depression (primary action) and extortion (2
nd
action) in primary
position of the eye. It is pure depression in abduction and pure extortion in
adduction. So the best position to examine superior and inferior recti muscles is
abduction to assess elevation and depression respectively.
2
The Oblique muscles:
- Inferior oblique: originates from angle between medial and inferior walls of orbit
posterior to inferior orbital margin just lateral to the lacrimal sac, and then it passes
below the eyeball and laterally to be inserted on the posterior lower temporal
quadrant of eyeball (posterior to equator).
* It is inserted at area corresponding to macula, so during operations when there is
aggressive manipulation for this muscle, it may lead to macular hemorrhage.
- Superior oblique: originates from roof of orbit just superior to annulus of Zinn,
passes forward and medially to the angle between the roof and the medial wall to be
reflected by passing through the trochlea and then directed backward, downward and
laterally to be inserted in the posterior upper temporal quadrant.
Innervation:
- Inferior oblique: Oculomotor nerve.
- Superior oblique: Trochlear nerve.
Action:
- Inferior oblique: extortion (primary action) and elevation (2
nd
action) in primary
position of the eye. It is pure elevation in adduction and pure extorter in abduction.
- Superior oblique: intortion (primary action) and depression (2
nd
action) in
primary position of the eye. It is pure depressor in adduction and pure intorter in
abduction. So the best position to examine inferior and superior obliques muscles is
adduction to assess elevation and depression respectively.
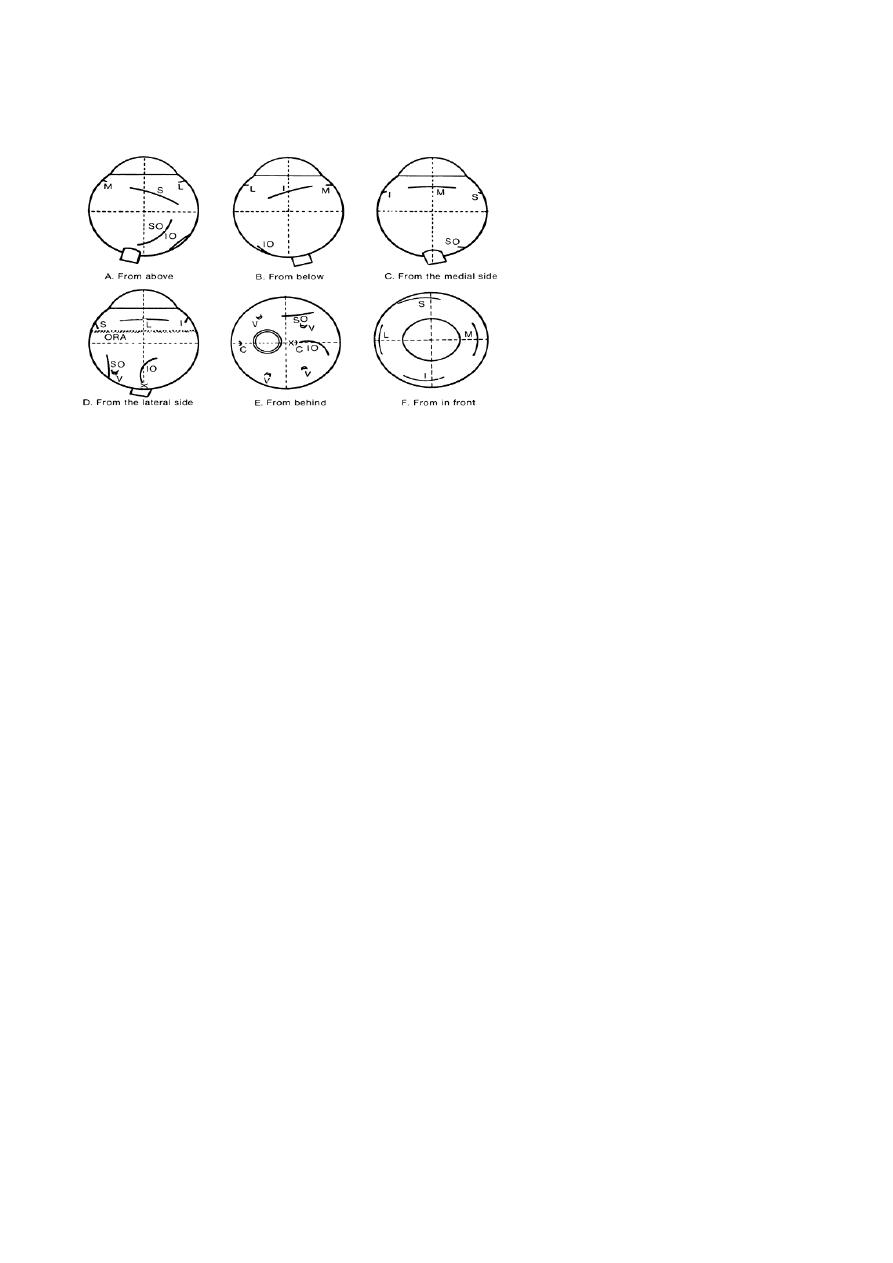
Insertion of eye muscles onto the
right eye. Note position of the optic
nerve (ON); its center is just above
the horizontal meridian. Position of
the macula (X); long ciliaries (C);
vortex veins (V); superior oblique
(SO); ora serrata (ORA); inferior
oblique (IO); medial rectus (M);
lateral rectus (L); inferior rectus (I);
superior rectus (S).

3
Axes of Fick:
Axes around which the movements of eyeball are occur. They are three; X
(horizontal axis parallel to the iris plain), Y (horizontal axis perpendicular to the iris
plain and X-axis) & Z (vertical axis).
- Movements around X-axis are elevation and depression.
- Movements around Y-axis are Intorsion and extorsion.
- Movements around Z-axis are adduction and abduction.
* Listing plane: Imaginary plane dividing the eyeball into anterior and posterior
halves, passing through the centre of rotation.
* For movement of one eye, we use terms "Adduction" (for inward movement) and
"Abduction" (For outward movement).
* For simultaneous movement of both eyes, we use terms "Dextroversion" (for
movement to right) and "Levoversion" (for movement to left).
* We have combined movement like: dextro-elevation, dextro-depression, levo-
elevation and levo-depression.
Squint:
is a misalignment of the visual axes.
Visual axis: is a line between the point of fixation and the fovea passing through
nodal point. The normal visual axes intersect at the point of fixation.
Optical axis: line perpendicular to iris that falls on the retina between the mucula and
the optic nerve.
* The angle between visual axis and optical axis is called kappa (κ).
The squint is either:
Manifest (-tropia): is a squint present when both eyes are open.
Or: Latent (-phoria): is a squint seen only when one eye is covered.
* Latent squint is not seen normally when both eyes are opened, but when we occlude
one eye it will deviate behind the cover, but as we remove the occluder there will
corrective movement which is not seen in normal person.
Eso-= inward,
Exo-= outward,
Hyper-= Elevation,
Hypo-= depression.

4
Latent strabismus (heterophoria)
Definition:
It is tendency of the eye to deviate from orthophoric position (straight head)
When the patient is fatigued and the brain loses interest in binocular single
vision but this tendency is checked subconsciously by the brain to maintain
binocular single vision.
Types:
Esophoria
Exophoria
Hyperphoria
hypophoria
Etiology:
1. Uncorrected errors of refraction:
Hypermetropia: the patient uses excessive accommodation to see
clearly. As a result, excessive convergence occurs with accommodation
which causes latent convergent squint.
Myopia: the patient relaxes his accommodation which results in lack of
convergence and the concurrent divergent squint.
2. Congenital weakness of one or more of extra ocular muscles.
Examination:
The idea is to abolish the stimulus for binocular single vision by covering one
eye (cover test).
Ask the patient to fix object.
Each eye is covered separately.
The occluder is quickly removed and the examiner notes whether or not the eye
under cover had deviated.
The examiner must also note if the eye makes a movement inwards or
outwards to pick up fixation once cover is removed.
If the covered eye deviates under the cover and when the cover is removed
returns to the original fixing position, latent squint is present.

5
Manifest squint is of two types:
1- Comitant (or Concomitant): when the angle of squint is the same in all
directions of gaze.
It can be:
a) Uniocular: same eye deviate all the time and the fellow eye always fixated.
b) Alternating: each eye fixes and deviates alternately.
2- Incomitant (paralytic): when angle of squint varies in various direction of gaze
and it become larger in the direction of paralytic muscle.
Paralytic squint (Incomitant squint)
Definition:
deviation of the eye due to paralysis of one or more of the extra ocular
muscles.
Surgery should not attempt till there is no hope for spontaneous recovery and
this is usually after 6 months to one year.
Etiology:
1. Nuclear lesions:
2. Nerve lesions:
3. Muscle lesions:
Diagnosis:
1. Ocular deviation: the paralyzed muscle loses its tone; the antagonist draws
the eye towards it i.e. the eye deviates to the opposite direction of the paralyzed
muscle.
2. Limitation of movement of the eye in direction of action of the paralyzed
muscle diagnosed by motility test.
3. Angle of deviation: changes in different directions of gaze and also changes
depending on which eye is fixing
4. Binocular diplopia
5. Compensatory head posture: abnormal head position adapted to avoid
diplopia.

6
Acquired comitant esotropia:
Classification of comitant esotropia: which can be accommodative or non-
accommodative.
1- Accommodative esotropia: related to accommodation, starts at 6m-5y and
mostly at 2y. It is divided into:
a) Refractive accommodative esotropia with a normal AC/A ratio is a physiological
response to excessive hypermetropia (usually between +4 and +7 D). For
example, a 4-year old boy has a refractive error of +5 D in each eye. Without
spectacles there is esotropia measures 20 Δ (4 Δ /1D). As spectacles control the
deviation for distance and near, the esotropia is of the fully accommodative type.
In these cases the eyes usually remain straight and surgery is not required.
b) Non-refractive accommodative esotropia is associated with a high AC/A ratio.
The refraction is usually normal for the age of the child (1.5 -3.0 D) and there is
little or no deviation for distance, although there is a significant esotropia for
near. It is corrected by bifocal glasses (Its upper part is made of 0 D glasses (for
distant) and has a lower part of 3D, to avoid accommodation for near)
c) Mixed accommodative esotropia: caused by the mechanisms above, and it is
treated by bifocal lenses, its upper part has the refractive power which corrects
the hypermetropia for far and its lower part has additive 3D for near.
Management of Accommodative esotropia:
(refractive, non-refractive and mixed)
Aims of management of child with Squint:
1- Restore binocular single vision (BSV).
2- Cosmetic.
a- History:
- Diplopia: it means squint develop in old children age when there is development
of BSV. If squint develops early in life there is suppression and ignorance of the
central nervous system to the image coming from squinting eye. Continuous
suppression leads to amblyopia called strabismic amblyopia.
- Age of onset. Most of congenital need surgery while many cases of acquired can
be treated with spectacles because it is related to the use of accommodation.
- General health. Other systemic diseases should be excluded prior to surgery if
needed and also other neurological diseases which are can be associated with
squint.

7
- Family history. We should search for any previous family history of squints and
the way of their treatment because the recent case is most likely corrected by the
same way.
- Way of delivery: forceps delivery may cause 6
th
nerve palsy.
b- Visual acuity: it is the corner stone, as our aim in management of child with
squint is to restore his binocular single vision.
* Binocular single vision is represented by simultaneous perception, fusion of
image and stereopsis. It may be affected even if the visual acuity is 6/6 because the
child using the fixating eye at one moment and squinting eye suppressed to avoid
diplopia and this event alternating between both eyes.
c- Motor examination: to exclude nerve palsy and other congenital abnormalities
of muscles.
d- Refraction: for assessment and determining its type and the way of treatment
(e.g. there is hypermetropia or not). This is done objectively be using retinoscope
instrument under complete cycloplegic effect by using atropine or cyclopentolate or
homotropine.
e- Fundoscopy: to exclude retinal diseases e.g. retinoblastoma, congenital optic
disc anomaly, and macular hypoplasia.
f- Correction of amblyopia: occlusion or penalization.
1. Correction of refractive errors: by giving the patient spectacles.
2. Occlusion of the fellow eye: this is done to enforce the amblyopic eye to
send stimulus to CNS by occlusion the fixating eye in uniocular squint. In
this method, we occlude the normal eye for 1week/1year of age, and then we
open the eye for three days, and then occlude it again and so on until
improvement of VA to its normal level (6\6). Don’t forget that continuous
occlusion of normal eye without rest and for long time can lead to more
serous amblyopia in this eye called deprivation amblyopia.
3. Penalization: it means partial occlusion to normal eye by daily instillation of
cycloplegic drugs (mostly atropine), where lead to blurring of vision. This is
done instead of occlusion if the amblyopia is mild.
g- Surgery: if the squint is not corrected or corrected partially by contiuous
wearing of spectacle for 2 months, the residual angle should be corrected by
surgery (recession and resection). In recession, we cut the muscle from its insertion

8
and insert it into a new site more far posteriorly from the limbus (weakening),
while in resection, we cut a part of the muscle and re-insert the muscle in its normal
insertion (strengthen).
* In alternating squint, the surgery done depends on the severity of squint, so we
may do:
- Unilateral medial rectus recession (weakening).
- Bilateral medial rectus recession (weakening) with or without unilateral or
bilateral lateral rectus muscles resection (strengthening).
* In squint surgical correction, you have to tell the child's parents that their child
might need more than one operation to get full correction.
2- Non-accommodative esotropia:
Essential infantile esotropia (congenital):
It is esotropia with onset since birth or during the first six months of life
Convergence excess.
Convergence spasm.
Divergence insufficiency.
Consecutive: patients with divergent squint who are underwent an operation
for correction of exotropia and ends with convergent squint due to
overcorrection.
Essential infantile esotropia (congenital):
Signs (or criteria):
a- Large angle.
b- Alternating in primary position and cross fixation in side gaze.
c- Usually associated with Nystagmus.
d- Not associated with refractive error.
e- Associated with inferior oblique overaction (if we have convergence, then
there will be elevation of the eye on adduction).
f- Usually it is squint per se, there is no neurological defect.
Management: the same way of accommodative esotropia but here the surgery is
most likely is the treatment and few cases are corrected by spectacles.
Treatment: bilateral medial rectus recession as soon as possible, but we have to
check for refractive errors (and correct any if found) and to do fundoscopy to
exclude retinal diseases as we do in all types of squint prior to surgery.
9
Exotropia (Divergent squint):
Classification:
1- Constant: see when both eyes are open all the time.
Congenital.
Sensory: This is usually associated with myopia.
Consecutive: due to surgical overcorrection of esotropia.
Congenital exotropia:
Signs:
Normal refraction.
Large and constant angle.
Usually associated with Neurological anomalies.
Treatment:
It is mainly surgical and done by bilateral lateral rectus recession ± resection of one
or two medial recti.
2- Intermittent: present in some times of the day and sometimes the eyes looks
normal (no squint). The diagnosis is just from the history taken from parents and
there may be no squint seen during the moment of examination. We should trust
parents in squint till improve otherwise because they live with the child 24 hours/
day and we examine him in few minutes.
Management:
Spectacles if associated with myopia or any other refractive errors.
Treatment of amblyopia.
Surgery: recession of both lateral recti.
Pseudosquint:
It is a false impression of ocular deviation.
Causes:
Convergent Pseudosquint
Divergent Pseudosquint
1- Small inter-pupillary distance
Wide inter-pupillary distance
2- Negative angle kappa e.g. myopia
Large
positive
angle
kappa
e.g.
hypermetropia.
3- Wide epicanthic folds