
Excessive Hair Growth
Growth of hairs that are longer, thicker or more numerous than the
location, age, and racial background of the patient would predict.
Hirsutism
Increased growth of terminal hairs in androgen-dependent areas,
producing male-like hair growth pattern in women. It is a common
problem among Iraqi females. Family history is positive in third of cases.
Areas of androgen dependence may be affected singly or in
combination, these are chin, sides of face, moustache, neck, chest
presternally, breast especially around the nipples, upper back and
shoulders, linea alba above the umbilicus.
Virilization is the association of hirsutism with other signs of male
development, such as voice deepening, clitoral enlargement, increased
muscles, loss of breast tissue, acne, and androgenetic alopecia.
Causes:
1- Physiologic: Some degree of hirsutism may be a racial or familial
trait constituting most cases of hirsutism. Minor facial hirsutism is
common after the menopause
2- Idiopathic: Some patients without a family background of hirsutism
become hirsute in the absence of any demonstrable hormonal cause.
Probable indemonstrable causes are:
A-Minor ovarian or adrenal dysfunction,
B-
local increased 5α reductase activity, or
C-Increased number of androgen receptors at hair follicles.
D-Increased sensitivity of androgen receptors at hair follicles.
3- Iatrogenic: Phenytoin, androgens, corticosteroids, contraceptives
(progesterone has androgen action)
4- Symptomatic: Some patients with hirsutism will have one of the
following disorders
A- Ovarian: Polycystic ovary disease, virilizing tumors.
B- Adrenal:Congenital adrenal hyperplasia virilizing tumors.
C- Pituitary: Cushing disease, acromegaly, prolactinoma
D-Ectopic virilizing broncogenic or GIT carcinomas.
Investigations
Women with a normal menstrual cycle and no signs of virilization are
unlikely to have a significant endocrine cause for their hirsutism.
Investigation is needed if these symptoms are present. Tests might
include: blood levels of LH, FSH, testosterone, prolactin; urinary free
cortisol; CT scan of suprarenal areas; pelvic ultrasound, Skull X-ray..etc
Therapy
Often unsatisfactory and needs continuous use, usually with relapse
after treatment discontinuation.

A-Treat underlying disease.
B-Removal of hairs:
1-Shaving, wax epilation, thread epilation, chemical epilation.
2-Bleaching (6
–10% hydrogen peroxide in water).
3-Destruction of individual hair follicles by electrolysis or thermolysis.
4-Photoepilation (with lasers or intense pulsed light source);
much faster and more effective.
5-Eflornithine (topical) effective but only as long as used; expensive.
C-Systemic therapy:
1-Primary antiandrogen: Flutamide, Cyproterone acetate.
2-Agents with secondary antiandrogen activity: Spironolactone.
3-GRH agonists: leoprolide and nafarelin.
4- 5-
α-Reductase inhibitor: Finasteride 2.5-5 mg daily.
5-Combination therapy.
Hypertrichosis
Excessive growth of terminal hair that does not follow an androgen-
dependant pattern.
A- Hypertrichosis lanuginosa
1-Hypertrichosis lanuginosa congenita:
Uncommon genodermatosis in which newborn is covered by long
lanugo hairs, which are not shed and replaced, but continue to grow.
Patient typically winds up with a silvery coat of hairs 10 cm long.
2-Hypertrichosis lanuginosa acquisita:
The sudden profuse covering of the skin by white lanugo hairs is a
reliable marker of internal malignancy (e.g. lung, colon, or breast, as
well as others)
B- Generalized Hypertrichosis
The entire body seems affected with regional differences. There are
many causes for diffuse excess numbers of terminal hairs:
1-Hereditary:
Porphyria
cutanea
tarda,
mucopolysaccharidoses,
chromosome abnormalities (trisomy 18).
2-Endocrine: Pituitary and thyroid disorders.
3-Eating disorders: (especially anorexia nervosa), malabsorption, fetal
alcohol syndrome.
4-Medications: Cyclosporine, minoxidil, phenytoin are most common
C- Localized (nevoid) hypertrichosis
1-Becker nevus: Localized mosaic area of increased melanin and
increased hair growth.
2- Faun tail nevus: Localized hair growth over sacrum; a serious marker
for potential underlying spinal cord defects or spina bifida. Neurological
and radiological work-up mandatory.
3-Hair nevus: localized area with excess hair follicles and no other
abnormalities; Uncommon.
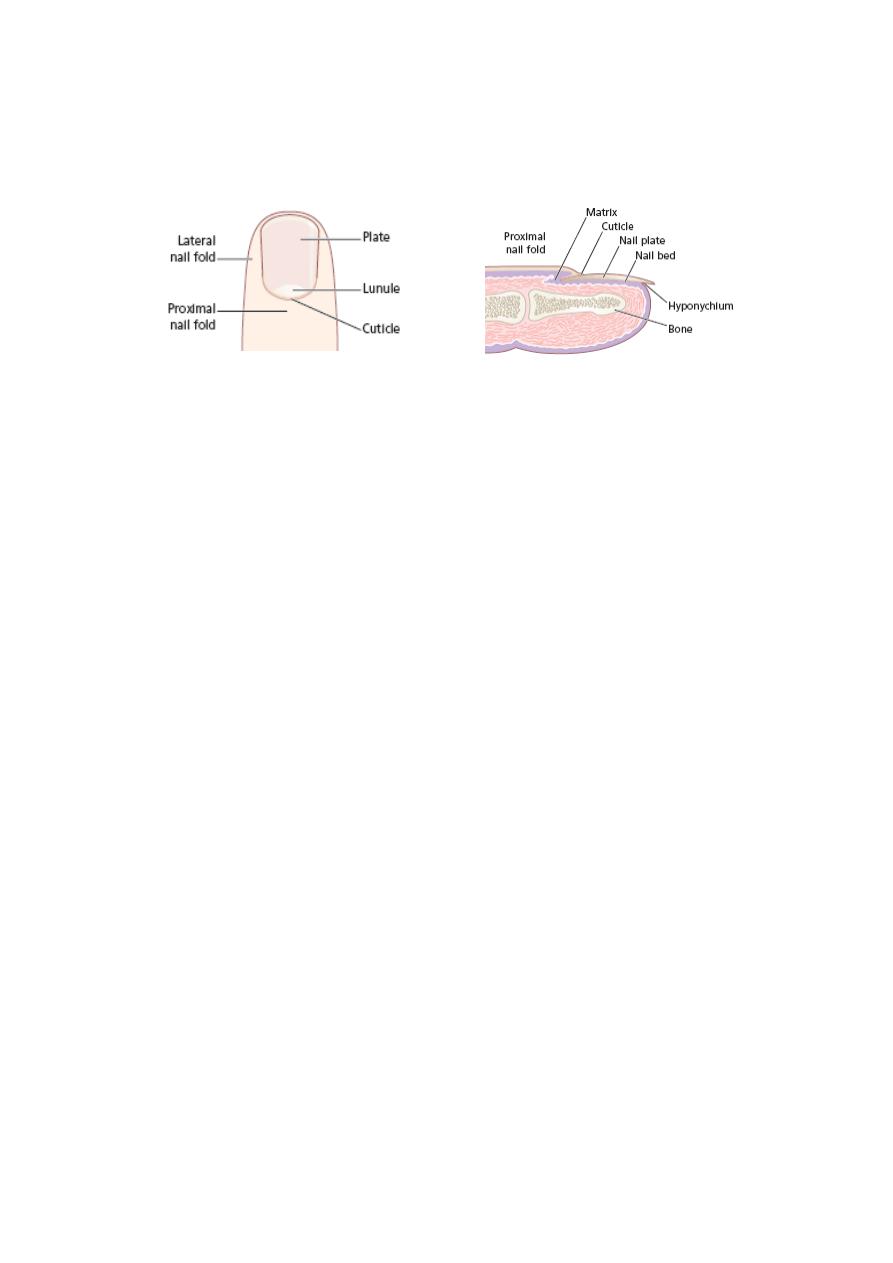
Nail
Problems
Components of the Nail
Congenital Disorders
Racket nails, characterized by a broad short thumb nail, is the
commonest congenital nail defect, dominantly inherited and seen in 1%
of the population. The basic abnormality is shortness of the underlying
terminal phalanx.
In the yellow nail syndrome, the nail changes begin in adult life,
against a background of hypoplasia of the lymphatic system. Peripheral
edema is usually present and pleural effusions may occur. The nails
grow very slowly and become thickened and greenish-yellow; their
surface is smooth but they are over curved from side to side.
Acquired Nail Changes
Beau's Lines
Transverse lines or grooves in nail. Causes include any severe
systemic illness or medications (chemotherapy), which affects growth of
the nail matrix. Clinically: The grooves or lines move distally; the
distance from the nail fold lets one assess the time of trauma.
Onycholysis
Separation of nail from nail bed. Causes include psoriasis, dermatitis,
fungal infections; medications (photo-onycholysis from tetracyclines or
psoralens), thyroid disease; rarely inherited. Idiopathic onycholysis is
most common among women; painless separation of nail without
apparent cause. Typically, the distal third separates and underlying nail
bed becomes darker and thickened. Therapy: Cut nail very short to
reduce leverage encouraging separation, apply antifungal solution.
Usually self-limited process.
Ingrown Nail
Penetration of nail plate into tissue of lateral nail fold. Almost always
involves great toes. Causes include congenital malformation of nail
(pincer nail), improper trimming, and tightly fitting shoes. Clinically:
Distorted nail with swelling, pain, and granulation tissue along the lateral

nail fold. Therapy: Mild cases: Eliminate pressure, trim nail; topical
antiseptics as foot soaks or on small piece of cotton wool pushed under
affected nail. Severe cases: lateral nail fold is excised and lateral aspect
of nail matrix destroyed.
Trauma
Trauma, especially from sport, commonly causes nail abnormalities.
Subungual haematomas usually occur when a fingernail has been
trapped or a toenail stood on or stubbed, but the possibility of a
subungual malignant melanoma must always be considered.
Splinter haemorrhages are induced by trauma, although they also
occur with infective endocarditis.
Brittle nails where nails break easily, usually at distal margins a
common complaint, usually due to repeated exposure to detergents and
water, although iron deficiency, hypothyroidism and digital ischemia are
other causes
Infections
Acute paronychia
Acute infection of nail fold, most often bacterial (staphylococcal)
infection, facilitated by damage to cuticle; less often herpes simplex;
rarely iatrogenic (patients receiving systemic retinoids). Presented as
painful swelling of proximal or lateral nail fold region. If bacterial,
incision and drainage; systemic antibiotics; if viral, no manipulation,
systemic antivirals.
Chronic paronychia
Chronic paronychia of the fingernails due to C. albicans is often seen in
wet workers. The cuticle is lost, the proximal nail fold becomes boggy
and swollen, and light pressure may extrude pus. The nail plate
becomes irregular and discolored. Gram-negative bacteria may be co-
pathogens and turn the nail a blue-green color. Management is
directed towards keeping the hands dry, applying an imidazole lotion or
cream twice daily to the nail fold, or oral itraconazole for 14 days.
Onychomycosis (tinea unguium)
Fungal infection of the nails. Toenails, especially the big toenails, are
involved more than fingernails. The process usually begins at the distal
nail edge and extends proximally to involve the whole nail. The nail
separates from the nail bed (onycholysis), the nail plate becomes
thickened crumbly and yellow and subungual hyperkeratosis occurs.
Several but almost never all the toenails may be involved. Treatment is
with systemic antifungal.

Dermatoses
The nails are commonly involved in skin disease, and are routinely
assessed in a dermatological examination. Treatment is aimed at the
associated dermatosis.
1-Eczema: Coarse pitting, transverse ridging, dystrophy, shiny nails due
to rubbing.
2-Lichen planus: Thinned nail plate, longitudinal grooves, adhesion
between distal nail fold and nail bed (pterygium), complete nail loss
3-Psoriasis: Pitting, nail thickening, onycholysis (separation of nail
from nail bed), brown discoloration, subungual hyperkeratosis.
4-Alopecia areata: Fine pitting, roughness of nail surface.
Tumors
Tumors of the nail and nail bed are rare, but it is not uncommon to see
benign tumors around the nail fold. Examples of both include:
Peri-ungual viral warts are common and stubborn. Cryotherapy must
be used carefully to avoid damage to the nail matrix. It is painful but
effective.
Periungual fibromas: These are seen in patients with tuberous
sclerosis and appear at or after puberty.
Glomus tumours: can occur beneath the nail plate. The small red or
bluish lesions are exquisitely painful if touched and when the
temperature changes. Treatment is surgical.
Myxoid (mucous) cysts: The cysts appear adjacent to the proximal
nail fold usually on the fingers. They are fluctuant, semi-translucent
papules that contain a clear gel and may arise from folds of synovium.
Treatment is by cryotherapy, injection with triamcinolone acetonide (a
steroid) or excision.
Malignant melanoma: A subungual malignant melanoma should be
excluded by biopsy if a pigmented longitudinal streak suddenly appears
in a nail, particularly if the pigment spreads to the surrounding skin.
Subungual haematomas may cause confusion but ‘grow out’ with the
nail. The risk of misdiagnosis is highest with an amelanotic melanoma,
which may mimic chronic paronychia or a pyogenic granuloma. Any
atypical or ulcerating lesion around the nail fold requires a biopsy to
exclude a malignant melanoma.