Disorders of the salivary glands
Dr. Ali Jaffer AlghazzawiDAdvSurg (GI)
CABS
MBChB

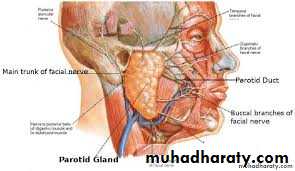
THE PAROTID GLAND- Anatomy
Bounded by : the ramus of the mandiblethe base of the skull
the mastoid process
Posterior relation : the carotid sheath
CNs XI&XII
Structures run through the gland
Facial nerve that divides into five branches
The terminal branch of the external carotid artery (maxillary & superficial temporal a.)
Retromandibular vein
Intraparotid LN
The facial nerve divides the gland into two lobes:
superficial 80%
deep 20%
accessory (ant. To the superficial lobe)
THE PAROTID GLAND- inflammatory disorders
Viral infectionsMumps is the most common cause of acute painful swelling
Predominantly affects children
Spread: airborne infected saliva
Prodromal period of 1-2 days (fever&headache)
Clinically: pain exacerbated by eating and drinking , swelling
Provides lifelong immunity
Rx: paracetamol& adequate oral fluid
Cx: orchitis, oophoritis, pancreatitis, sensorineural deafness & meningoencephalitis
Recurrent parotitis of childhood
It may be caused by an incompetent punctum that leads to soiling of the parotid ducts with contaminated oral fluids.
Children 3-6 years ,rapid swelling of one or both glands,
fever& malaise last 3-7 days. The symptoms worsen
by chewing and eating.
Sialography: punctate sialectasis (snowstorm)
Rx: endoscopic washouts& antibiotics

THE PAROTID GLAND- inflammatory disorders
Bacterial infections ( acute ascending bacterial siladentis)Previously described in dehydrated elderly patients following major surgery.
Reduced salivary flow secondary to dehydration results in ascending infection via the parotid duct into the parotid paranchyma.
Currently , it is commonly associated with a salivary calculus.
Tender, painful swelling, generalised malaise, pyrexia and cervical lymphadenopathy
Symptoms exacerbated by eating or drinking
Intraoral exam; pus exuding form the parotid gland papilla
Staphylococcus aureus or streptococcous virdans
Rx; appropriate antibiotics
absecss… aspiration with large pore needle or formal drainage under anaesthesia (the skin incision should made low to avoid damage to the lower branch of the facial nerve)
Sialography is contraindicated during acute infection.
THE PAROTID GLAND- inflammatory disorders
HIV- associated sialadenitisMay present as chronic parotitis in children.
May present as classical Sjogren syndrome in adults clinically and histologically but there is lack autoantibody.
May present with multiple parotid cysts which cause gross parotid swelling and facial disfigurement.
CT&MRI; characteristic Swiss cheese appearance of multiple large cystic lesions.
The swollen glands usually painless and may regress on the institution of antiviral therapy.Cysts may be aspirated

THE PAROTID GLAND- obstructive parotitis
Stone formation (sialolithiasis) and stricturesParotid sialolithiasis 20%
The stones are usually radiolucent.
Locations; confluence of the collecting ducts, at the point the courses over the masseter muscle or in the distal aspect of the parotid duct adjacent to the parotid papilla.
Presentation: intermittent swelling particularly in the mealtimes.
Ix : US
Rx: Small stones (less 4mm) retrieved by basket
up to 8mm broken with lithotripsy
larger than 8 mm removed by endoscopic assisted surgery
Strictures of the parotid duct 20%
Stricture lead to stagnation and mucus plug obstriction
Clinically; meal time syndrome starting at the breakfast as swelling which persists. Massage release the plug with a gush of salty saliva.
Rx dilatation and endoscopic washouts with steroid solutions
Papillary obstruction
trauma to the parotid results in inflammatory oedema and obstruction of salivary flow.
May result dilation of the duct (mega-duct) which visible coursing the patient cheek
Rx progressive dilation of the punctum& stent insertion.
Papillotomy should be avoided as it cause stricture.
THE PAROTID GLAND- tumours
The most common site of salivary tumours
Most tumors arise from the superficial lobe.
Slow-growing , painless swelling below ,in front of the ear or in the upper aspect of the neck
Less commonly arise from accessory loble
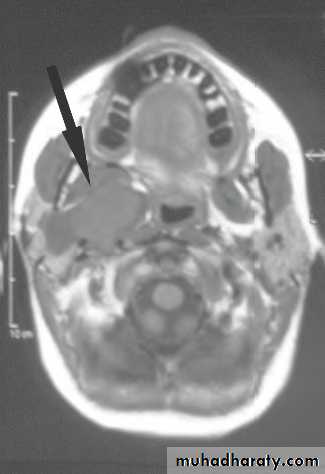
Rarely arise from deep lobe and present as paraphryngeal mass.
Symptoms include difficulty in swallowing and snoring. Clinically there is diffuse firm swelling in the soft palate and tonsils
80- 90 % are benign
Most common benign tumor is benign pleomorphic adenoma
Most common malignant tumor is mucoepidermoid carcinoma, followed by adenocystic carcinoma which is notorious for its proclivity for perineural invasion and metastatic potential.


THE PAROTID GLAND- tumours
TypeSubgroup
Common examples
I Adenoma
Pleomorphic
Monomorphic
Pleomorphic adenoma
Adenolymphoma (Warthin’s tumour)
II Carcinoma
Low grade
Acinic cell carcinoma
Adenoid cystic carcinoma
Low-grade mucoepidermoid carcinoma
High grade
Adenocarcinoma
Squamous cell carcinoma
High-grade mucoepidermoid carcinoma
III Non-epithelial tumours
Haemangioma, lymphangioma
IV LymphomasPrimary lymphomas
Secondary lymphomas
Non-Hodgkin’s lymphomas
Lymphomas in Sjِgren’s syndrome
V Secondary tumours
Local
Distant
Tumours of the head and neck especially
Skin and bronchus
VI Unclassified tumours
VII Tumour-like lesions
Solid lesionsBenign lymphoepithelial lesion
Adenomatoid hyperplasia
Cystic lesions
Salivary gland cysts
THE PAROTID GLAND- tumours
InvestigationsUS: confirm the lump intrinsic to the gland or not.
facilitates the sampling of the lesion by FNAC.
CT & MRI
Open biopsy is contraindicated unless in gross malignancy and preoperative histological diagnosis is required as a preclude to radical parotidectomy


THE PAROTID GLAND- tumours
ParotidectomySuperficial parotidectomy: the part of the gland superficial to the facial nerve is removed
- Benign, low grade and low stage malignant tumours
- Partial superficial parotidectomy for small tumours
- Extracapsular dissection: benign parotid gland tumours
B. Radical parotidectomy: is performed when there is clear histological evidence of high grade malignant tumors eg squamous cell carcinoma with invasion of the facial nerve.
it involves removal of all parotid tissue and division of the facial trunk through the main trunk with removal of the ipsilateral masseter muscle and may require neck dissection particularly when there is clinical, radioliogical and cytological evidence o f lymph nodes metastasis.
COMPLICATIONS OF PAROTID GLAND SURGERY
haematoma formation;
infection;
deformity: unsightly scar and retromandibular hollowing;
temporary facial nerve weakness;
transection of the facial nerve and permanent facial weakness;
sialocele;
facial numbness;
permanent numbness of the ear lobe associated with great auricular nerve transection;
Frey’s syndrome.
THE PAROTID GLAND- tumours
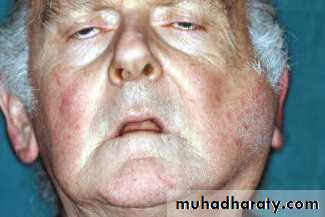
Frey’s syndrome(gustatory sweating) is considered an inevitable consequence of parotidectomy unless preventive measures are taken .
It results from damage to the autonomic innervation of the salivary gland with inappropriate regeneration of the postganglionic parasympathetic nerve fibres of the auriculotemporal nerve that aberrantly stimulate the sweat glands of the overlying skin.
Clinically; sweating and erythema (flushing) over the region of surgical excision of the parotid gland
Diagnosis ;starch iodine test. This involves painting the affected area with iodine, which is allowed to dry before applying dry starch, which turns blue on exposure to iodine in the presence of sweat.
Sweating is stimulated by salivary stimulation.
PREVENTION
● sternomastoid muscle flap;
● temporalis fascial flap;
● insertion of artificial membranes between the skin and theparotid bed.
All these methods replace the barrier between the skin and the parotid bed to minimise inappropriate regeneration of autonomic nerve fibres.
MANAGEMENT OF ESTABLISHED FREY’S SYNDROME
● antiperspirants, containing aluminium chloride;
● denervation by tympanic neurectomy;
● the injection of botulinum toxin into the affected skin. ( most effective and can be performed as an out-patient).