DR. HADAF ALJUNAIYEH
Psoriasis
A common inflammatory disease of skinChronic relapsing condition
Unpredictable course
Has a great impact on patient’s life
Emotional impact: patients with psoriasis often display: 1-Depression 2- Feeling of unattractiveness 3-Fear about future & prognosis
Wrongly assumed to be contagious
Embarrassment in public places & hair dressers
Epidemiology
Prevalence is 2-3 % of the populationRanging between 0.91% in the US to 8.5% in Norway
Equal male & female ratio
Estimated incidence 60 per 100000 per year
Age of onset
Mean age of onset 23-37, with 2 peaks with possible genetic associations:1- Early onset 16-22 years: more severe & aggressive presentation & possible first degree relative affection
2_ Late onset 57-60 years: milder & absent first degree relative involvement
pathogenesis
Two key pathophysiological aspects:1) Increased rate of keratincytes proliferation+ parakeratosis
2) Large inflammatory cell infiltrate as polymorphs, T cells, & others.
Familial component, many relatives affected, increased in successive generations, multifactorial inheritance
* Psoriasis is a T cell mediated auto-immune disease *
Current hypothesis:Unknown skin antigen stimulate immune response
Antigen-specific memory T cells are primary mediators
Leading to impaired differentiation & hyper proliferation of keratinocytes
Triggering factors in susceptible patients
1-Infection:β hemolytic strept. throat infection
precede guttate psoriasis.
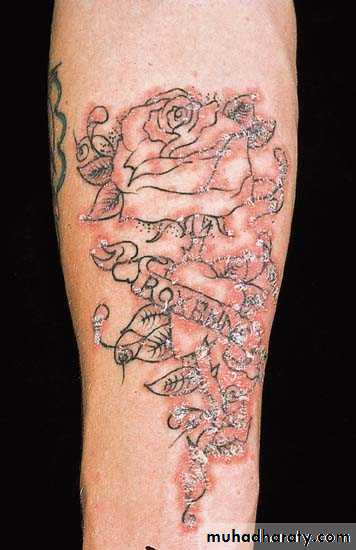
2-Trauma: positive Kobner’s phenomenon
4- Drugs:
antimalarials, lithium,β blockers worsen
psoriasis, stopping
steroids causes
rebound of the rash.

Metabolic
5-
6-Hormonal:
as in pregnancyRole of obesity
Doubles the risk of psoriasisBMI correlate with psoriasis severity
Clinical features
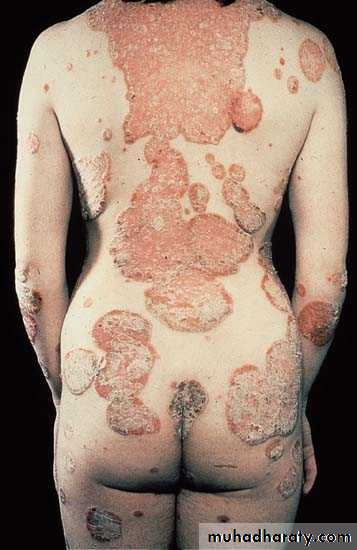
• Well-demarcated, sharply defined• erythematous (salmon pink)
• plaques covered by silvery
• white scales
• Usually symmetrical
Scalp psoriasis
Koebner’s phenomenon

The commonest complaint isscaling
scalingFollowed by:
ItchingThird is
Redness of skinNext is
Tightness of skinBleeding is the 5th
Burning the 6th complaint
Last is
• Fatigue•
Clinical types of psoriasis
Psoriasis vulgaris
Chronic plaque psoriasisThe commonest type 85%
Can be extensive
Guttate psoriasis
Numerous small lesions about 1cmUsually less scaly
Trunk & proximal limbs
Usually patients less than 30
Often preceded by strept URTI.
Flexural psoriasis
In body foldsLess scaly
Often miss DX if no
other signs of psoriasis
Napkin psoriasis
2-8 months old babies
disappear by topical treatment
Might reappear in adult life.
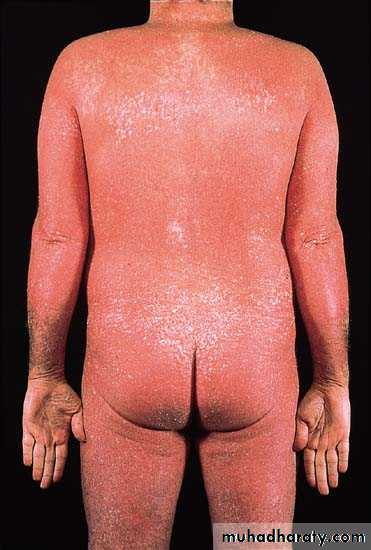
Erythrodermic psoriasis
UncommonMore than 90% of skin surface
Can evolve from chronic or eruptive
Fever, hypo & hyperthermia,
dehydration
Complications: Heart failure,
infections, malabsorption, & anaemia
Pustular psoriasis
1- Localized:more common
On palms & soles
2- Generalized:
Associated with fever
Palmoplantar psoriasis
Can be hyperkeratotic orpustular
Difficult to distinguish from
chronic eczema or tinea
May be aggravated by trauma
Psoriatic arthritis
In 5-10% of psoriaticsRare before age 20
Rheumatoid factor (–ve) arthritis
5 types either peripheral or central, often
overlap
Nail changes in psoriasis
1) Distal onycholysis.2) Random pitting from parakeratosis of proximal matrix.
3) Oil spots which are yellow areas of subungual parakeratosis
4) Salmon patches due to nail bed psoriasis.
5) Subungual hyperkeratosis resembling onychomycosis.
Nail psoriasis
Treatment
Reassurance, explanation are vitalPsoriasis is not contagious
No cure, so the aim is to induce remission or making it more tolerable
Spontaneous remission in 50% of cases
Quit smoking
Three main modalities of treatment
TopicalPhysical
systemic
calcipotriol
vitamin D agonist, only reduce thickness & scaling of the plaquesIt is irritant so better combined with steroid to get a greater response, fewer S.E., plus steroid sparing
Topical corticosteroids
Most commonly used, clean & effectivebut frequent S.E.; such as:
1- dermal atrophy
2-tachyphylaxis
3-early relapse
4- precipitation of pustular type
• Indications of topical steroids:
1)On face, ears & flexures2) Patients can’t tolerate tar, dithranol, etc, due to allergic or irritant reaction3)Unresponsive psoriasis of scalp, palm & sole4) Patients with minor, localized type5) In combination with other modalitiesPhysical treatment 1- Light therapy
Most patients benefit from sunlightUVR is the main treatment for moderate to severe psoriasis
S.E. include sunburn & increased risk of skin CA
Artificial UVB by fluorescent bulbs, either narrow band(311nm.) or broad band
Max. effect achieved is at MED (min. dose to induce erythema in a test patch after 24h)
2-PUVA
Psoralens are natural phtosensitizersHigh intensity, long wave UVR( UVA), given 2 hours after ingestion of 8-methoxy psoralen, twice weekly
20-25 sessions are needed, +maintenance doses
Clearance ‘ll occur in 75% of patients
Not for young patients
UVR resistant glasses worn for24 hours
Systemic treatment 1- Methotrexate
• Folic acid antagonist, inhibit DNA synthesis in S phase• Given orally or parentally , 7.5-15mg, once weekly
• Minor S.E. nausea & malaise in 1st.24hr.
• Serious S.E. are liver toxicity, marrow suppression, teratogenicity & male oligospermia
• Should monitor liver, renal & marrow function, before & during treatment
2-Neotigasone (=Acitretin)
Acitretin is vitamin A analougueEspecially effective in pustular psoriasis of palms& soles, & plaque psoriasis
Frequent minor S.E. as dryness of skin & m.m., pruritis, hair fall, & paronychia.
Serious S.E. are hyperlipidemia especially of triglycerides & teratogenicity
Can be combined with PUVA= RE-PUVA
3-Cyclosporine
Inhibits cell mediated immunity
Very effective in psoriasis
Serious S.E. as hypertension, renal damage, persistent viral warts & a risk of skin cancer.
4- Biologics
Biologics: new, monoclonal antibodies to key pathological pathways in psoriasisAgainst T.N.F. α(alpha)
Against receptors involved in T-cell trafficking as interleukin 12/23(IL-12/IL-23) blockade agents
Interleukin 17-A
Expensive, requires careful consideration of medical Hx, disease severity & monitoring of infections