Breast pathology
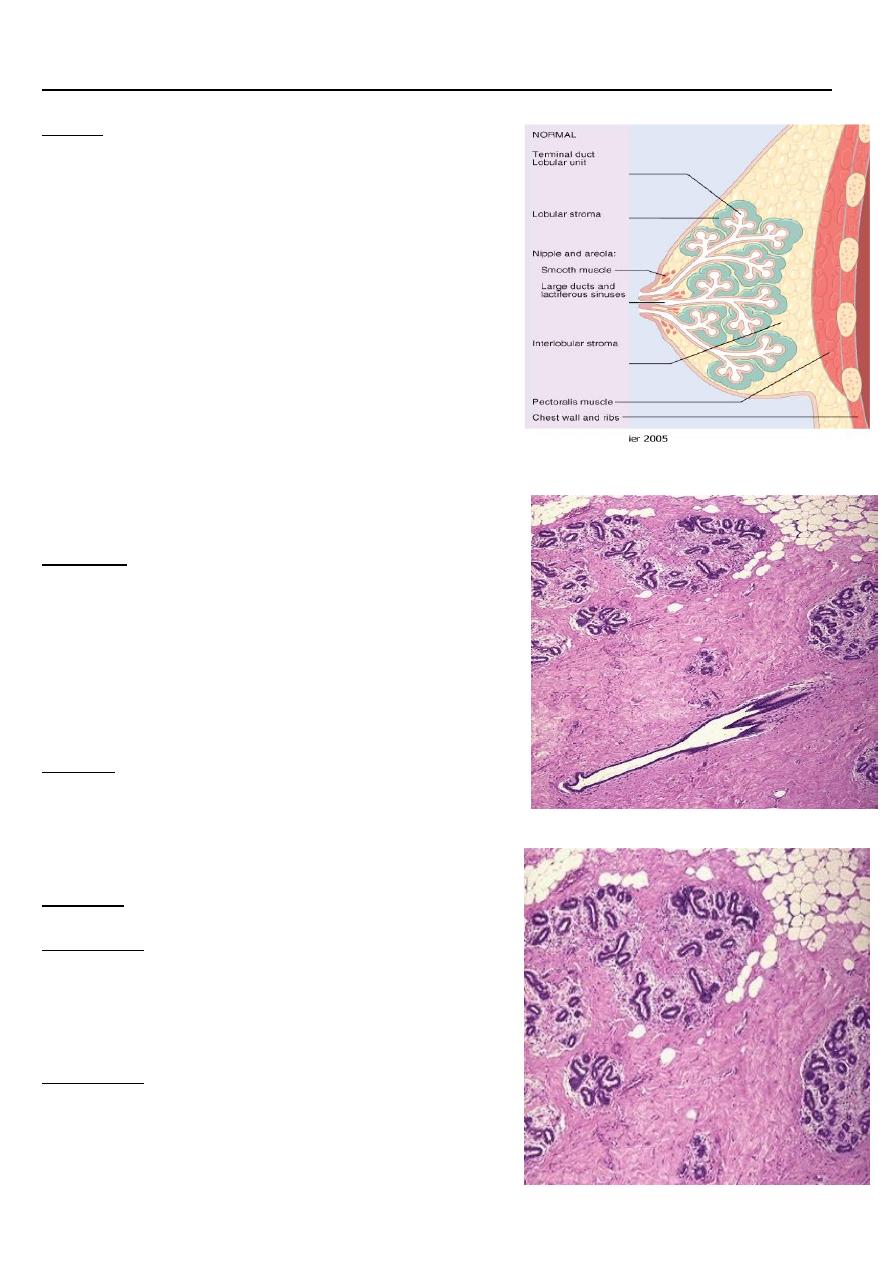
Breast:
❑
- Modified sweat gland.
❑
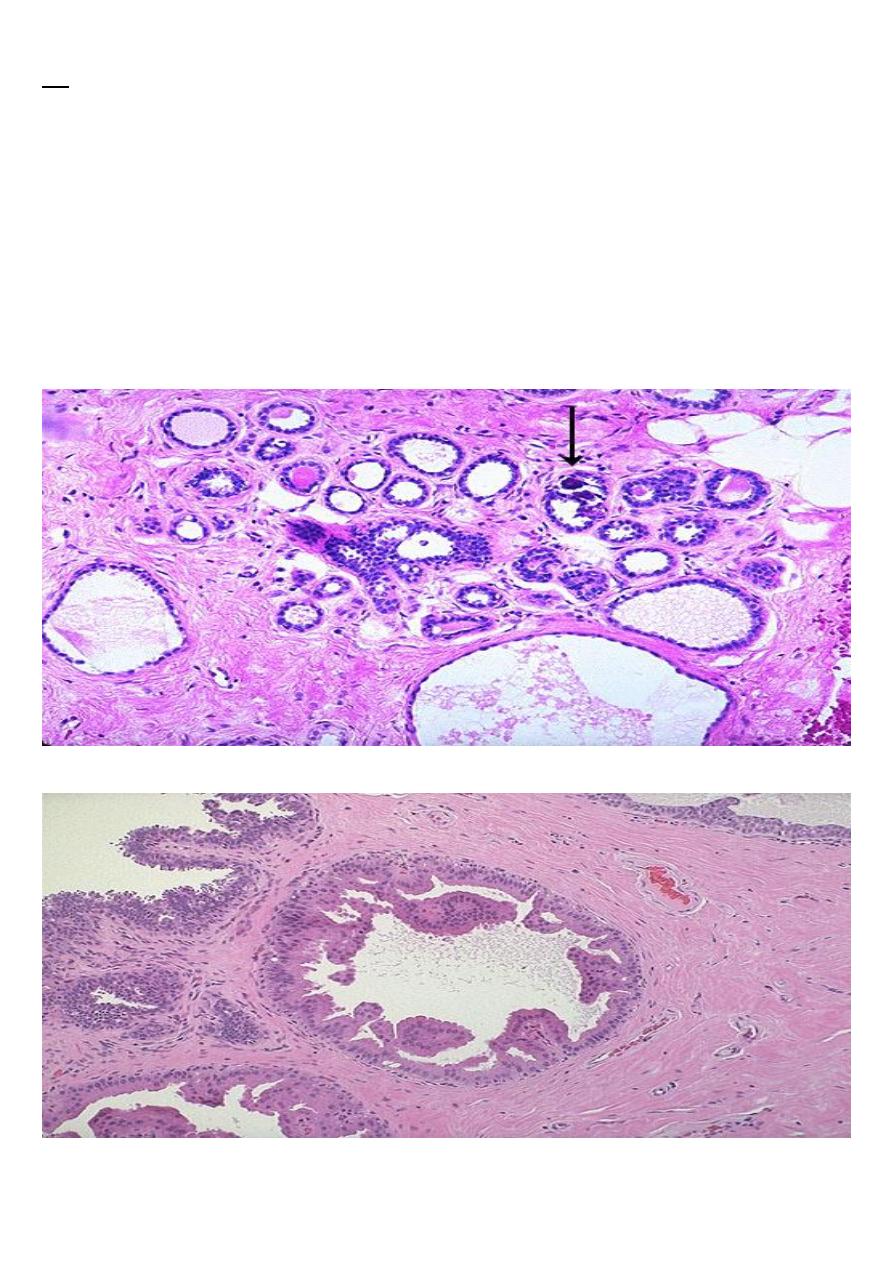
Parenchyma of the breast composed of 12-20
distinct lobes. Each lobe contains many lobules
which are the functional units. The ducts of each
lobe drain into a large duct called lactiferous
duct that open separately into the nipple.
HISTOLOGY:
Epithelial:
Ducts: Major ducts( lactiferous, major, lobar,….), small
ducts & ductules.
Acini:
- Epithelial & myoepithelial cells
Stromal:
Interlobular & intralobular.
STROMA:
Interlobular:
- The major component.
- Dense fibroconnective tissue, later replaced by fat.
Intralobular:
-
Loose myxoid tissue.
-
Poor in elastic fibers
- Hormone responsive.
Life cycle changes of breast development
Breast Pathology
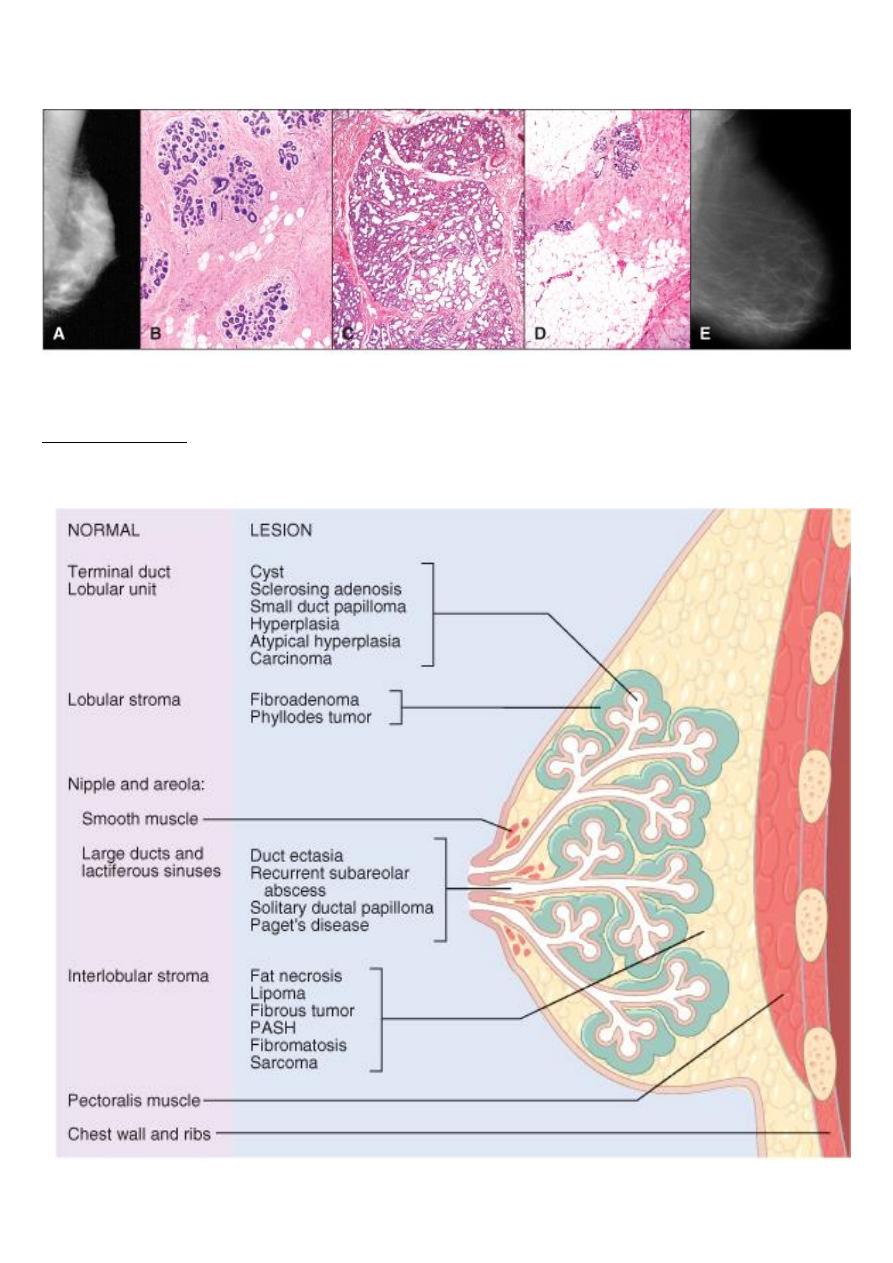
Categories of breast diseases:
Disorders of Development
A) Hypoplasia:
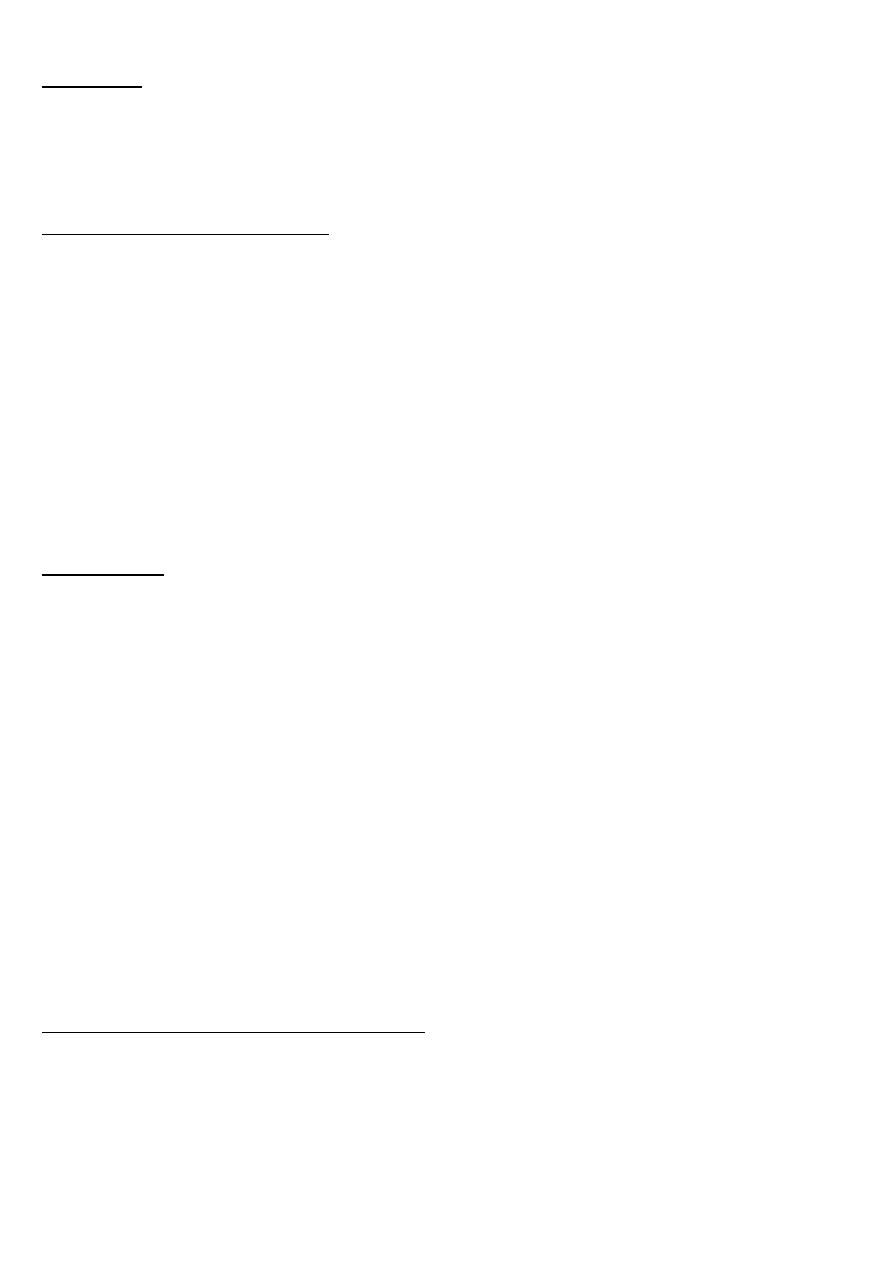
B) Supernumerary nipple:
C) Accessory axillary breast:
D) Congenital inversion of nipple:
E) Macromastia:
Supernumerary nipple:
Persistent of epidermal thickening along the milk line.
Galactocele
A cystic dilation of an obstructed duct that arises during lactation. Besides being painful
"lumps," the cysts may rupture to incite a local inflammatory reaction, which may yield a
persistent focus of induration that may arouse suspicion of malignancy
INFLAMMATIONS OF THE BREAST
Uncommon and during the acute stages usually cause pain and tenderness in the involved
areas.
Included in this category are several forms of mastitis and traumatic fat necrosis, none of
which are associated with increased risk of cancer.
1-Acute mastitis:
Develops when bacteria gain access to the breast tissue through the ducts; when there is
inspissation of secretions; through fissures in the nipples, which usually develop during the
early weeks of nursing; or from various forms of dermatitis involving the nipple.
Morpohology:
Staphylococcal infections induce single or multiple abscesses accompanied by the typical
clinical acute inflammatory changes. Streptococcal infections generally spread throughout the
entire breast, causing pain, marked swelling, and breast tenderness. Resolution of these
infections rarely leaves residual areas of induration
2-Chronic inflammatory mastitis :
True chronic inflammation of the breast due to bacterial infection is uncommon . Most
cases are due to incomplete resolution of acute mastitis in the lactating breast or due to
chronic breast abscess .
3-Tuberculosis :
It is very rare but may occur secondary to tuberculosis of the lungs .
Mammary duct ectasia (periductal mastitis)
:
It is a nonbacterial chronic inflammation of the breast associated with inspissation of breast
secretions in the main excretory ducts. Ductal dilation with ductal rupture leads to reactive
changes in the surrounding breast substance.
It is an uncommon condition, usually encountered in perimenopausal multiparous women.
Mammary duct ectasia is of principal importance because it leads to induration of the breast
substance and, more significantly, to retraction of the skin or nipple, mimicking the changes
caused by some carcinomas
Traumatic fat necrosis:
is an uncommon and innocuous lesion that is significant only because it produces a mass.
Most women with this condition report some antecedent trauma to the breast.
During the early stage the lesion is small , often tender, and sharply localized.
It consists of a central focus of necrotic fat cells surrounded by neutrophils and lipid-filled
macrophages, which is later enclosed by fibrous tissue. Eventually the focus is replaced by scar
tissue. Calcifications may develop in the scar
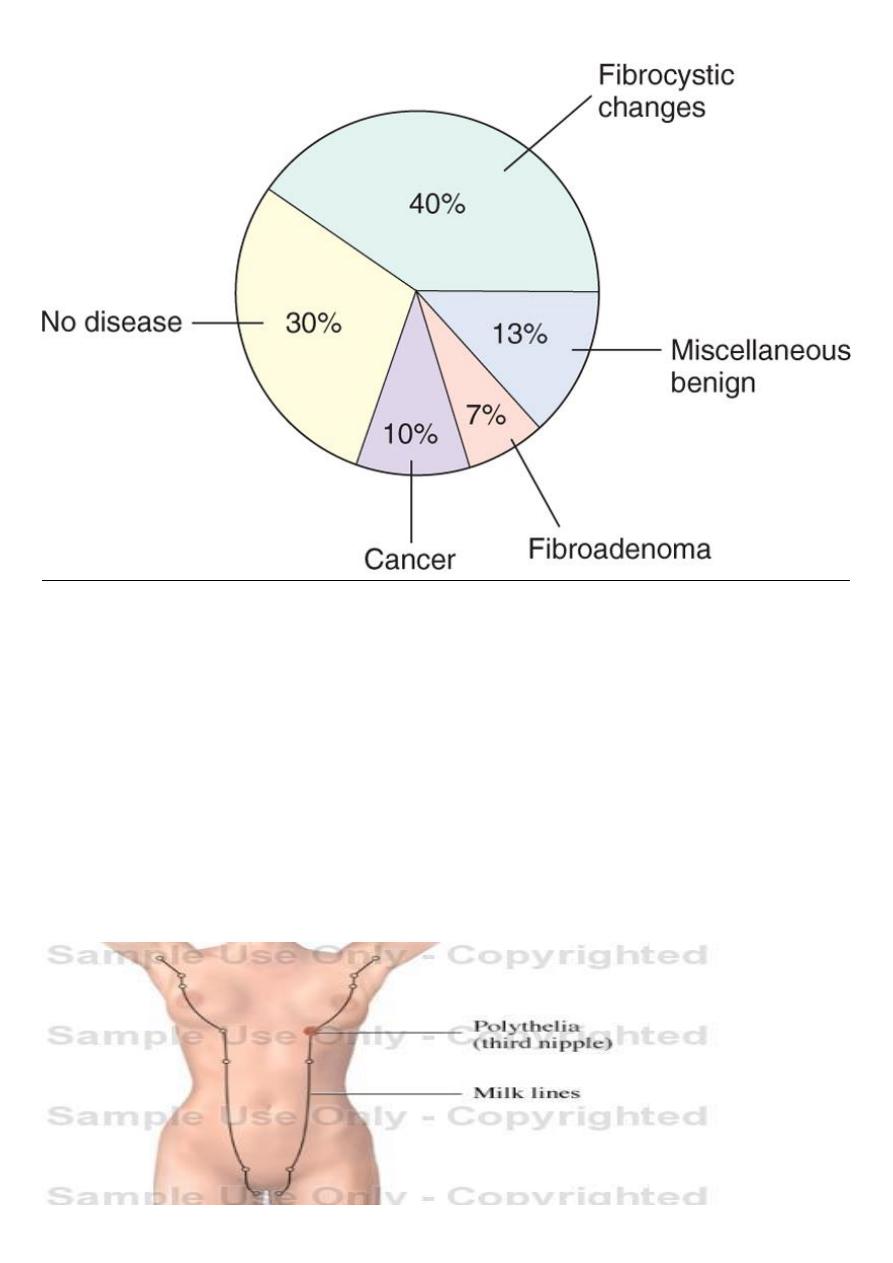
Fibrocystic Changes
This is a group of morphologic changes which very frequently develop in the FEMALE breast
during reproductive period of life but may persist after menopause, and are the commonest
cause of a lump or lumpiness of the breast. It is a common condition & often of no clinical
significance (found at autopsy in 60% to 80% of women).
Most of the changes encompassed within the diagnosis of fibrocystic disease have little clinical
significance except that they cause nodularity; only a small minority represent forms of
epithelial hyperplasia that are clinically important.
The "lumps" produced by the various patterns of fibrocystic change must be distinguished
from cancer.
The alterations are crudely subdivided into:
Non-proliferative pattern: include cysts, fibrosis, apocrine metaplasia (
simple fibrocystic
change).
Proliferative patterns: include epithelial hyperplasia (typical & atypical), papillomas &
sclerosing adenosis.
It is widely accepted that this range of changes is the consequence of an
exaggeration and
distortion of the cyclic breast changes that occur normally in the menstrual cycle.
Estrogenic therapy and oral contraceptives do not seem to increase the incidence of these
alterations; indeed, oral contraceptives may
decrease
the risk.
m.i
The changes arise mainly from the TDLU & there are 4 principal patterns ( singly or in
combination):
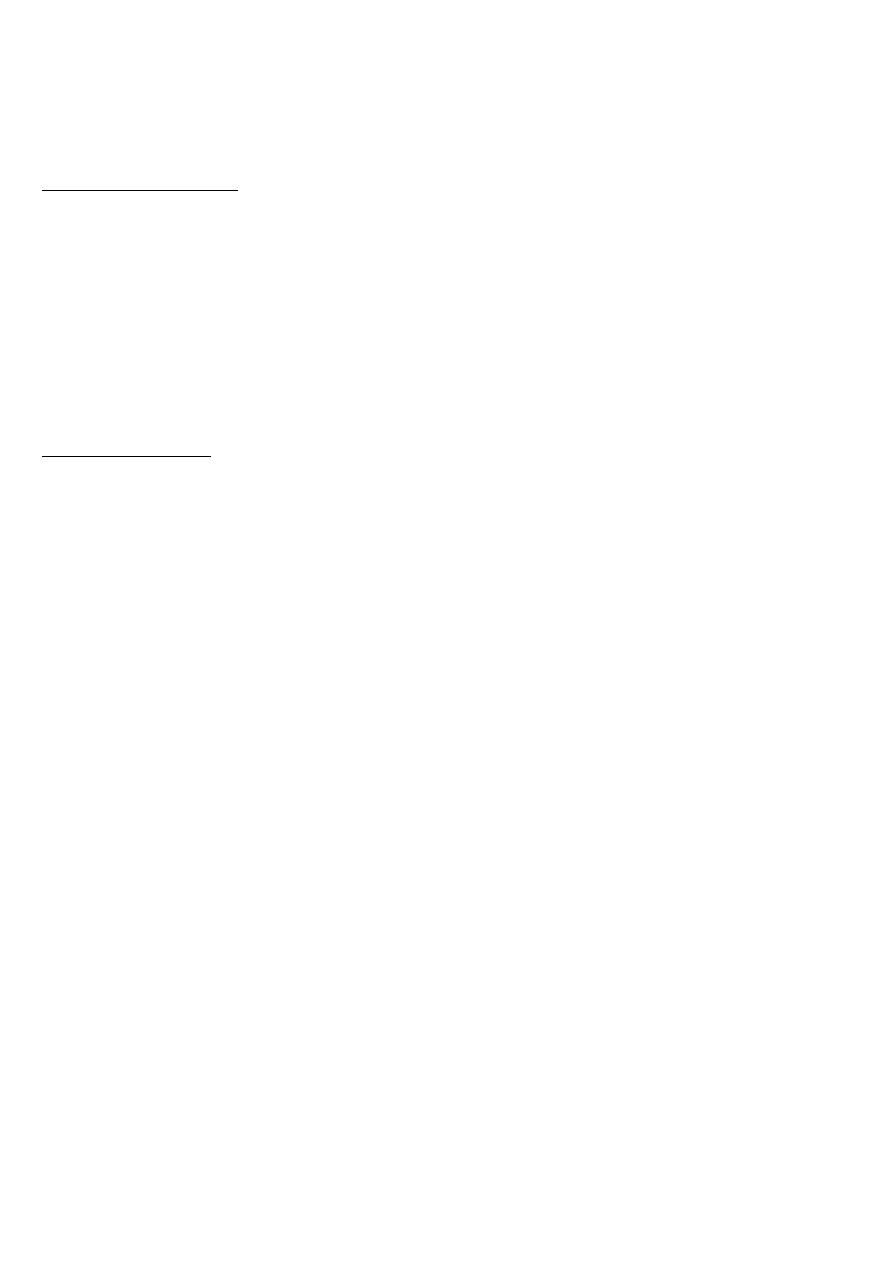
Cyst formation: Cystic dilatation of the terminal ducts & lobules of variable degree.
Fibrosis: Presence of area of dense collagenous tissue.
Apocrine metaplasia: Her the ducts become lined by large cells having abundant granular
eosinophilic cytoplasm resembling that of apocrine sweat glands.
Adenosis: It means increase in the no. of acini & lobules
Fibrocystic disease, adenosis, fibrosis,
cystic change
Fibrocystic disease, apocrine change
PROLIFERATIVE BREAST DISEASES
A group of breast disorders that characterize by proliferation of epithelial cells.
Include:
✓
Epithelial hyperplasia.( atypical hyperplasia increase the risk of malignancy)
✓
Sclerosing adenosis.
✓
Others.
Epithelial Hyperplasia:
- Increase in the no. cells that line the ducts & lobules.
- Either occurs alone or as part of FC change.
- Classification depends on:
* No. of layers.
* Presence & degree of atypia.
* Architectural pattern.
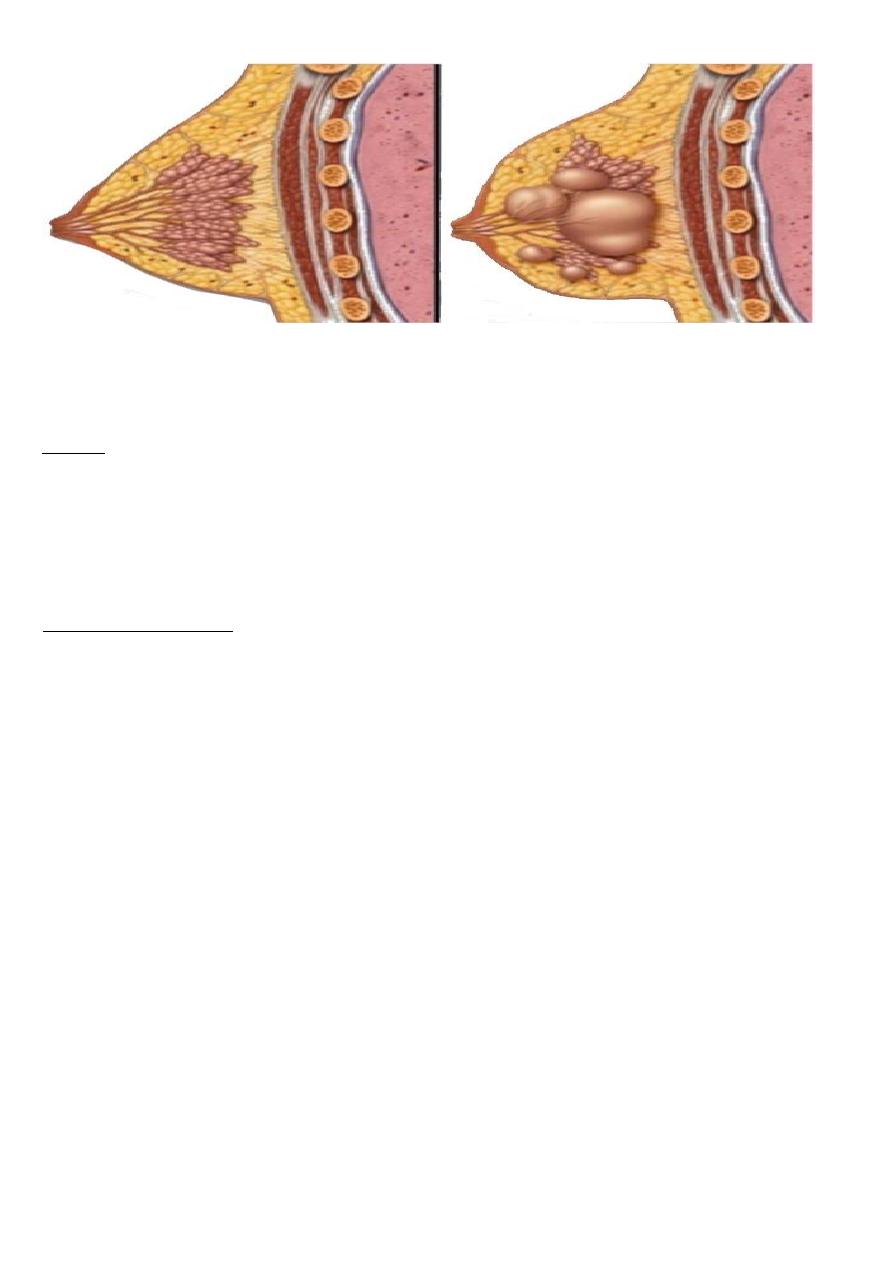
A: Atypical ductal hyperplasia. A duct is filled with a mixed population of cells consisting of
oriented columnar cells at the periphery and more rounded cells within the central portion.
Although some of the spaces are round and regular, the peripheral spaces are irregular and
slitlike. These features are highly atypical, but fall short of a diagnosis of DCIS. B, Atypical
lobular hyperplasia. A population of monomorphic small, round, loosely cohesive cells partially
fill a lobule. Some intracellular lumens can be seen. Although the cells are morphologically
identical to the cells of LCIS, the extent of involvement is not sufficient for this diagnosis
Epithelial hyperplasia
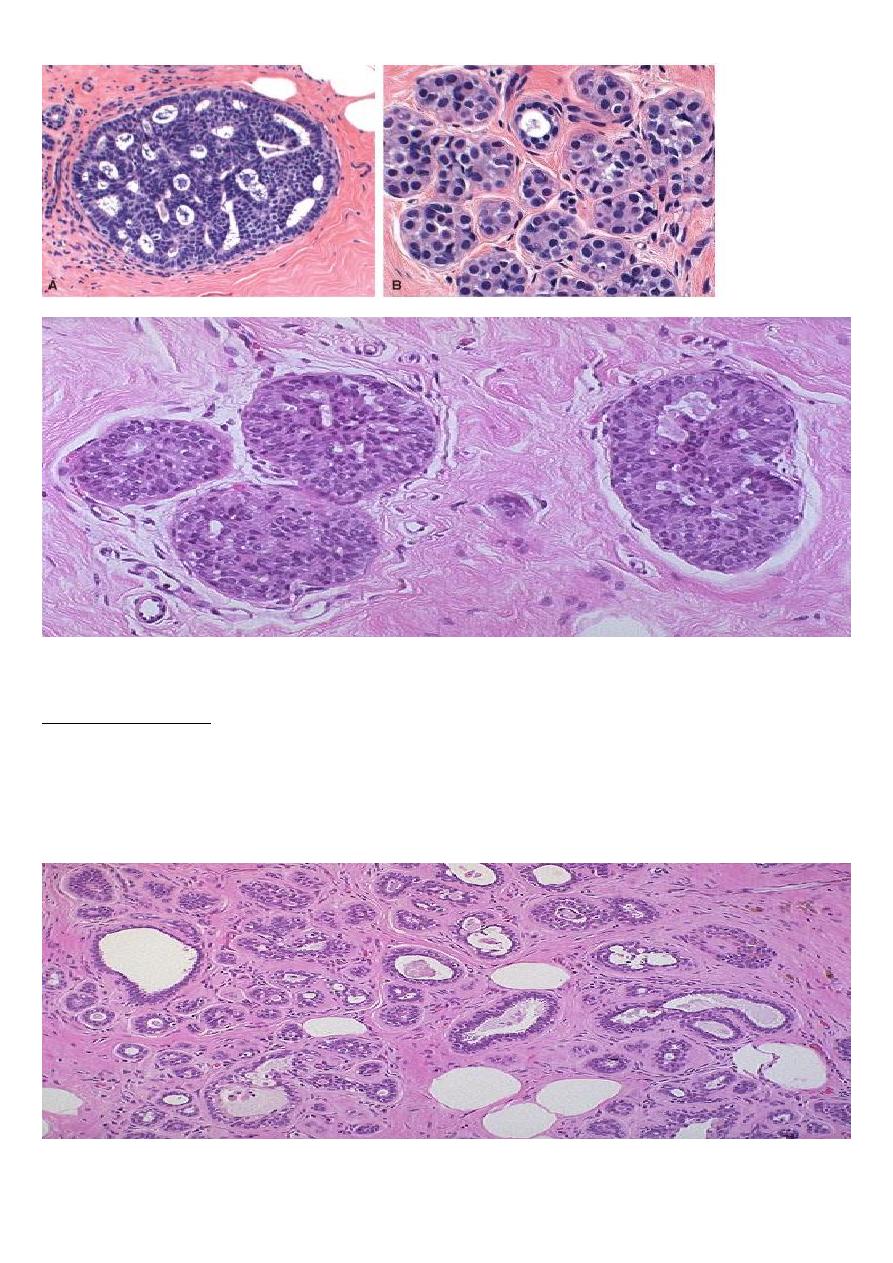
Sclerosing Adenosis
A proliferative breast disease characterized by increased no. of acini that are distorted and
compressed by excess fibrous tissue in a specialized morphological arrangement.
Clinically it can mimic carcinoma ( irregular firm-hard mass, calcification).
Sclerosing adenosis
