
Urinary Tract Infections
• Dr. Ali Althabhawi

Urinary tract infection
Urinary tract infections (UTIs) commonly occur in children of all
ages,
UTIs are most common in children under age 1 yr
➢
1-3% of girls and 1% in boys
➢
Peak via infancy and toilet training, after the 1st attack of
girls, 60-80% will develop 2nd attack of UTI, within 18
months
➢
In boys, more common in 1st year and much more common
in uncircumcised,
➢
In 1st year M/F 2.8-5.4:1, beyond infancy , the ratio is 1:10
▪
Atiology
➢
Mainly by colonic bacteria, in female, 54–67% due to E-coli
followed by proteus and Kliebsiella .In male, older than 4
year , proteus common as E-coli, reported G+ve in male
➢
Staph-saprophyticus is a pathogen in both sex
➢
Virus(adeno) 11,21 cystitis
➢
UTI have been consider as imported cause in development of
renal insufficiency and end stage renal disease
▪Pathogenasis
▪Nearly all UTI are secondary from bacteria arise from fecal flora ,
colonized the perineum and enter the bladder via urethra, or from
bacteria beneath the prepuse in
uncircumcised boy , it may lead to
pyelonephritis.
▪Rarely hematogenous spread
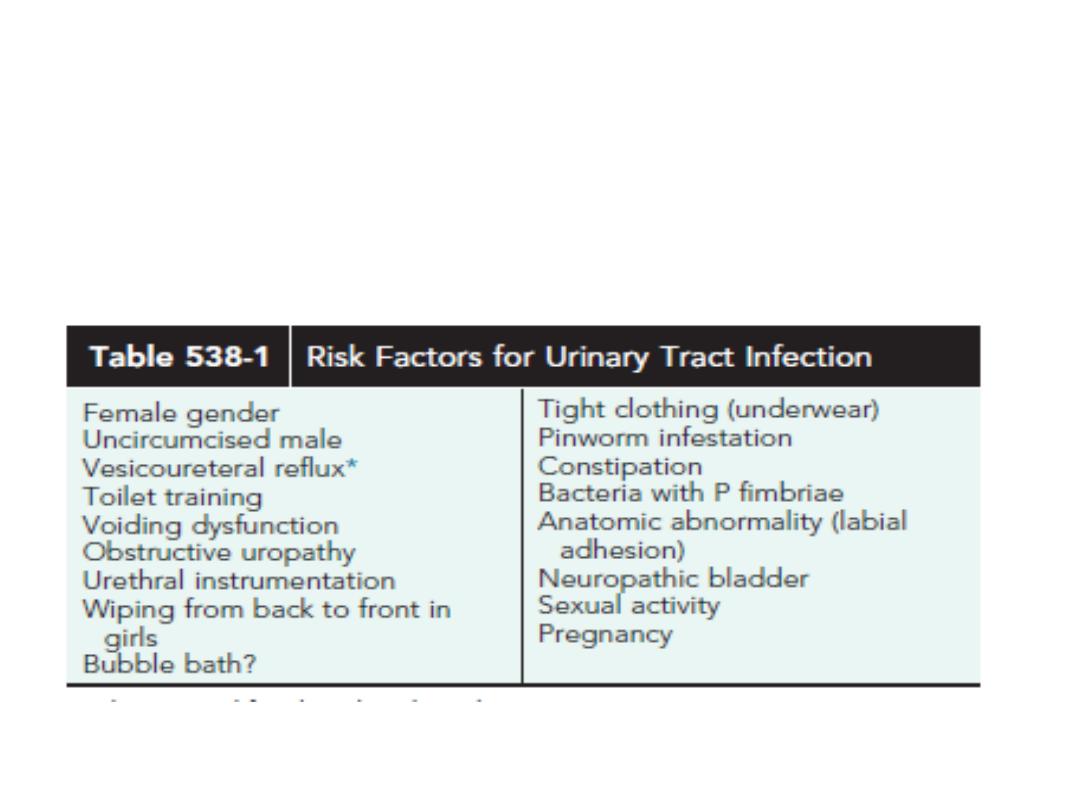
▪Risk Factors of UTI
The incidence of UTI in breast fed babies is less than formula fed
.

According to the 2011 AAP Guidelines for children 2-24 mo,
Risk factors for girls include
white race, age younger than 12 mo, temperature >39°C (102.2°F
, fever for longer than 2 days, and absence of another source of
infection
.
Risk factors for boys
include nonblack race, temperature >39°C (102.2°F), fever for longer
than 24 hr, and absence of another source of infection.
Atypical features include
➢
Failure to respond within 48 hr of appropriate antibiotics.
➢
Poor urine flow,
➢
Abdominal flank or suprapubic mass,
➢
Non–E. coli pathogen,
➢
Urosepsis,
➢
Elevated creatinine level.

Clinical features
1
-
Pyelonephritis
➢ Is characterized by any or all of the following
➢ Abd pain(flank), fever(may be the only manifestation), malaise,
nausea, vomiting, and accocianly diarrhea, in newborn and infant,
nonspecific (irritability, jaundice, poor feeding, weight loss).
➢ Pyelonephritis is the most common serious bacterial infection in
infants <24 mo of age who have fever without an obvious focus
➢ Involvement of renal parenchyma is termed acute
pyelonephritis whereas if there is no parenchymal
involvement, the condition maybe termed pyelitis.
➢ Renal abscess typically occurs following hematogenous
spread with S. aureus or can occur following a
pyelonephritic infection caused by the usual
uropathogens

2- Cystitis
➢ Baldder involvement, dysurea, frequency, urgency, malodorous urine,
no renal damage, no fever
➢ cystitis is more common in boys; it is self-limiting, with
hematuria lasting approximately 4 days.
➢ Acute hemorrhagic cystitis, though uncommon in
children, is often caused byE. coli; it also has been
attributed to adenovirus types 11 and 21. Adenovirus
3- Asymptomatic bacterurea
➢ +ve urine culture but no manifestation, benign condition , no
treatment require except in pregnancy

Diagnosis
▪Suspected from
▪symptoms and or finding of urine analysis or
both.
▪+culture for confirmation and appropriate
treatment
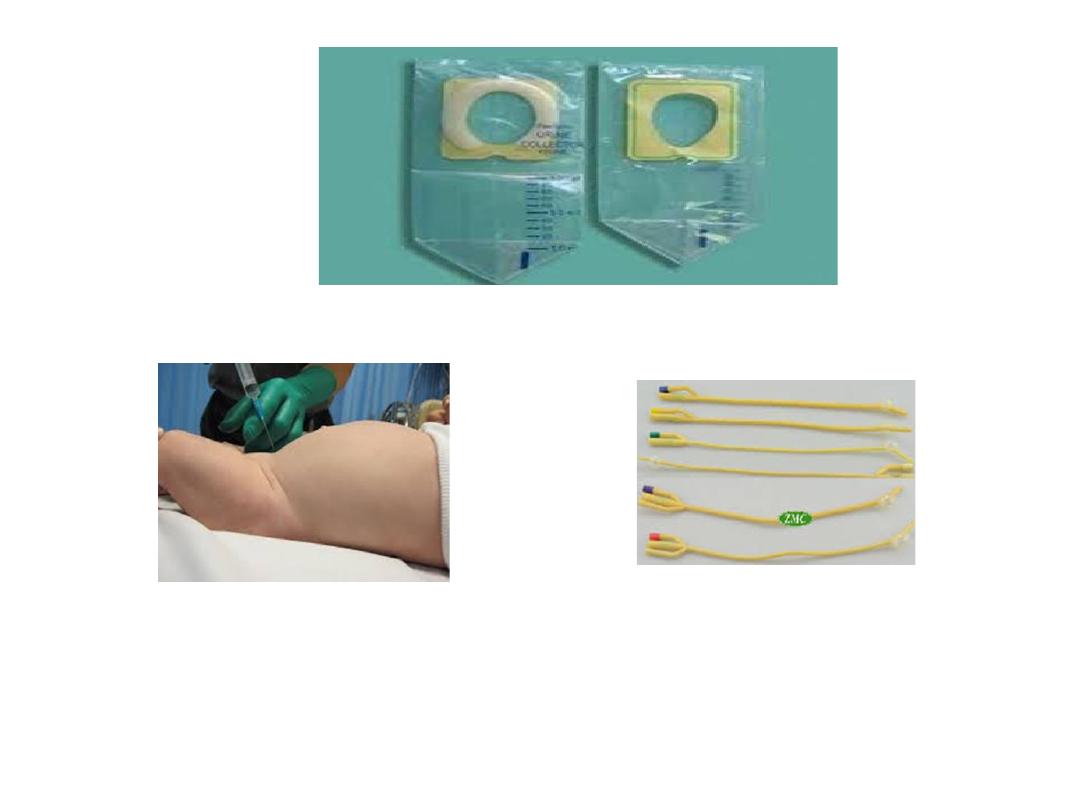
▪the DX of UTI, depend on proper sampling of
urine(4 ways)
▪1- Midstream urine
= in child having toilet
training +ve if the colony count more than
100,000 colony –forming units(CFU)of single
MO or child is symptomatic, and 10,000 CFU is
consider UTI, In
uncircumcised boy , the
prepuce should be retracted.
2- Adhesive , sealed
, sterile collecting urine
bag= in infant, after disinfection of skin of
genitalia.
false-positive rate too high to be suitable for
diagnosing UTI; however, a negative culture
is strong evidence that UTI is absent.
+ve if the colony count more than 100,000
CFU
of
single
MO
and
child
is
symptomatic,and
+ve
urine
analysis,
however if any of this critera are not met , we
may need next way

Catheterized sample
= proper skin preparation , gentle technique of
catheter is important, feeding tube poly thene nu 5 or nu 8 with
lubricant in older child to decrease risk of trauma, +ve if more than
10000 CFU of
4-
Suprapubic puncture
= +ve if any MO best method
NOTE
Prompt plating of urine sample is important (stay in room temp for
60 min, lead to over growth of minor contamination the may
suggest UTI), put it in refrigerator.
single MO

Others indicators of UTI
A- pyurea
(pus cell in urine) suggest UTI, this finding is more confirmatory
than diagnostic. Conversely, pyuria can be present without UTI.,so its absence
does not exclude UTI(sterile pyurea)
Sterile pyuria
(positive leukocytes, negative culture) occurs in
1- partially treated bacterial UTIs,
2-viral infections,
3-renal tuberculosis,
4- renal abscess,
5- UTI in the presence of urinary obstruction,
6- urethritis due to a sexually transmitted infection
7-inflammation near the ureter or bladder (appendicitis, Crohn disease),
8- interstitial nephritis (eosinophils)
B- Nitrate and leukocytestrase +ve in urine
If a child asymptomatic, GUA normal, it is unlikely UTI, however, if child
symptomatic, and GUA normal, possible UTI.
C- Blood (neutrophilia, increase ESR, CRP,
in renal abscess, WBC 20,000-
25,000, blood culture is indicated sp in infant(sepsis)

E-Renal
Scannig
with
Techneutiaium-
labeled
DMSA(DiMarcoptoSuccinic Acid)
Is the most sensitive and accurate way to detect the renal
scaring.
F- Urogram
less sensitive than DMSA in detecting the
renal scaring, and need 1-2 year to detect the pathology , risk
of radiation
G- CT of abdomin
to detect the scaring in some time.

Treatment
1- Acute Cystitis
should be treated to prevent pyelonephritis
A- if symptomatic (sever), urine culture should be obtained, a 3- to 5-
day course of therapy with trimethoprim-sulfamethoxazole (TMP-
SMX) (6-12 mg TMP/kg/day in 2 divided doses) or trimethoprim is
effective against many strains of E. coli. Nitrofurantoin (5-7 mg/kg/24
hr in 3-4 divided doses) also is effective and has the advantage of being
active against Klebsiella and Enterobacter organisms. Amoxicillin (50
mg/kg/24 hr in 2 divided doses) also may be effective as initial
treatment but has a high rate of bacterial resistance.
B- if symptomatic (less sever ),treatment started till result of urine
culture
.
2- Pyelonephritis
14
days
course
of
broad
spectrum
of
AB
(Ampicillin
100mg/kg+Gentamycin 3-5mg/kg ) cefotaxime (100 mg/kg/24 hr), or
Ceftriaxone 50-75mg/kg not exceed 2 gram)is preferable (less
ototoxicity and nephrrotoxicity), serum cr and level of Gentamycin
should be obtained before and during treatment if prolonged
.a

Indications of hospitalization
A- dehydration
B- unable to drink
C-possiple sepsis
D-age less than 1month
➢
Alkinization of urine is valuble in treatment of proteus with
Gentamycin.
➢
Oral 3rd generation cephalosporin(Cefixim) is effective in G-ve
ather than Pseudomonus
➢
4 quinololl drevative is effective(contraindicated below age of
17years, effect the growing cartlige ), occasion for short-course
therapyin younger children with Pseudomonas UTI
Levofloxacin is an alternative quinolone with a good safety profile in
children
➢
Some outhers suggest loading dose of Ceftriaxone then oral 3rd
generation cephalosporin(cefixim).
➢
In absecce
percuatenus drange +parental AB
➢
Urine culture should be obtained 1week after complete the
treatment(should be sterile)

In recurrent UTI and in absence of risk factor , periodic urine culture every
3months for 2 years (if child asymptomatic) is indicated.
In recurrent UTI
, identify the risk factor and treat it and give AB
prophylactic(1/3 of therapeutic dose) , Trimetheprime, Nitrofurantuine ,
Nalidixic acid., indicated in
1- neurogenic bladder
2- stasis due to obustruction
3- VUR, stone
Amoxil, Keflex is effective but increase risk of breaking through
UTI(become resistant)
Probiotic, cranberry juice
Imaging Study
1-1st episode of clinical pyelonephritis
2-Those with a febrile UTI
3- In infants, those with systemic illness
4-A positive urine culture, irrespective of temperature,
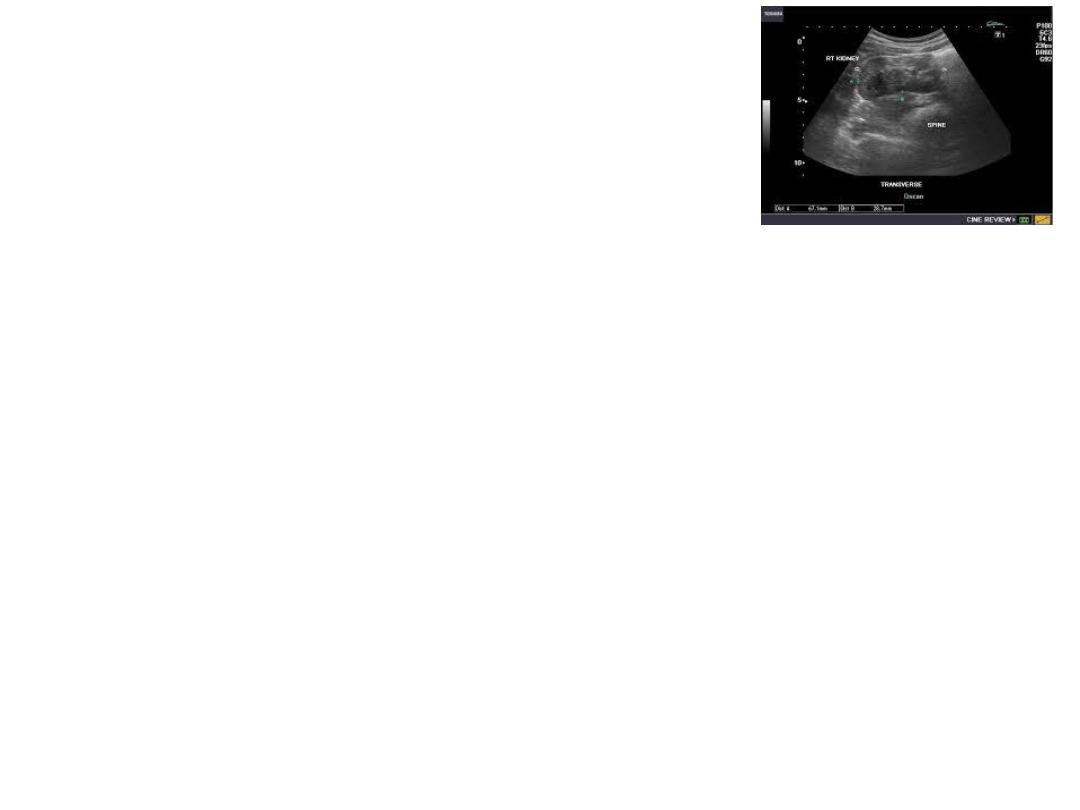
a
sonogram
of kidneys and bladder should be
performed to assess
1- Kidney size
2-Detect hydronephrosis
3- Ureteral dilation,
4- Identify the duplicated urinary tract
5- Evaluate bladder anatomy.
Next,
a DMSA
scan is performed to identify whether the child has
acute pyelonephritis. If the DMSA scan is positive and shows either
acute pyelonephritis or renal scarring,
.
a
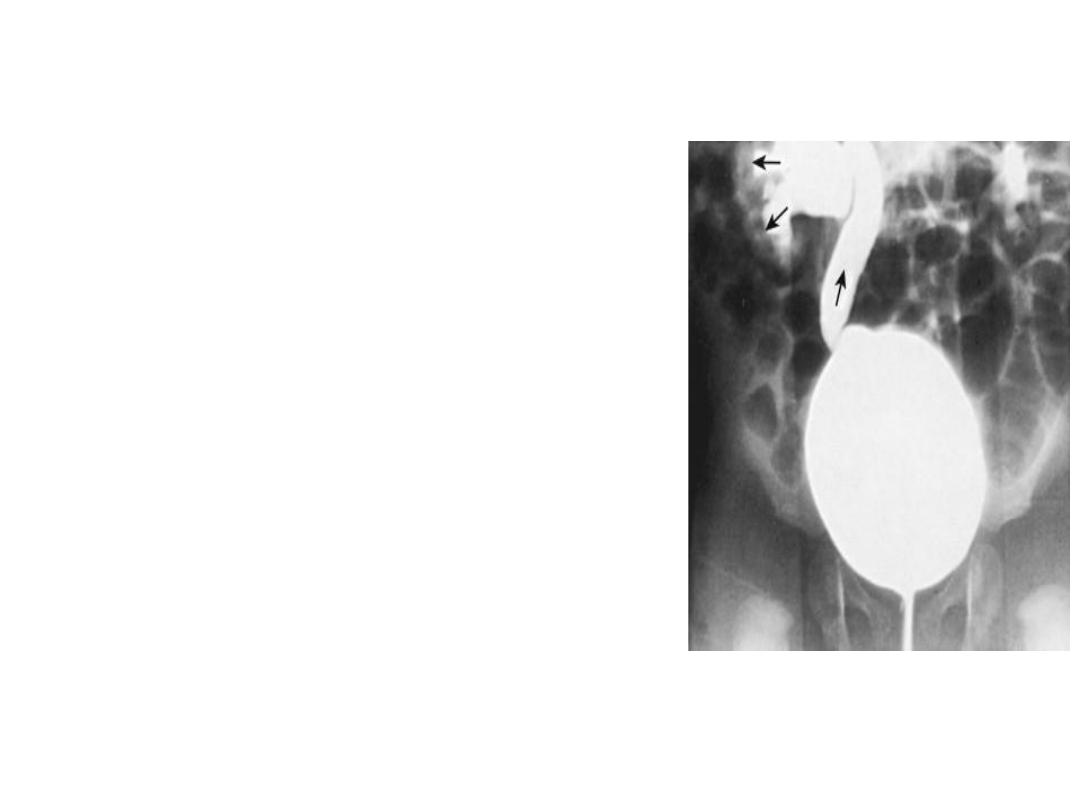
voiding cystourethrogram
(VCUG) is
performed in(AAP)
1-Ultrasound study is abnormal.
2-Atypical features.
3- Recurrent febrile UTI
. If reflux is identified, clinician needs to
decide on whether to send the child to a facility
with DMSA capability(if available) or instead
do a VCUG
VCUR
Time= 2-6 week after infection
2types
1- Radionucltide less radiation, less
anatomical differentiation
2- Contrast
more radiation , good
differentiation

Definitions of atypical and recurrent UTI
Atypical UTI
UTI associated with sepsis or bacteraemia
Concern regarding obstructive uropathy
Failure to respond to antibiotics within 48 hours
Associated impaired renal function
Infection with a non E. coli organism
.
Recurrent UTI:
➢
Two or more episodes of UTI with acute pyelonephritis/upper
urinary tract infection, or
➢
One episode of UTI with acute pyelonephritis/upper urinary tract
infection plus one or more episode of UTI with cystitis/lower
urinary tract infection, or
➢
Three or more episodes of UTI with cystitis/lower urinary tract
infection.
VesicoUretric Reflux(VUR)
IS retrograde flow of urine from the bladder to the ureter and renal
pelvis
Normally , ureter is attached to the bladder in oblique direction
perforating between the bladder mucosa and detroser muscle ,
creating a flap-valve mechanisim that prevent reflux. Reflux occur when
the tunnel between the mucosa and detroser muscle is short or
obliterated.
-reflux usually congenital, run in family (1%), 35%of sibling of a child
with reflux also have a reflux
- reflux in 25% in neuropathic bladder, 50% in boy with posterior
urethral valve, 15%inrenal agenasis
- 20% of ESRD, gave ahistory of reflux
- reflux is important cause of HT in children
Reflux pyelonephritis renal scaring renal
insufficaincy ESRD

Clinical feature
Usually discovered during evaluation of UTI, 80% in
female , average age is 2-3 year
Renal insufficiency, HT
DIAGNOSIS
1- VCUG, reflux occurring during bladder filling is
called (low pressure)or passive and less likely to
show spontaneous resolution,
high pressure or active more
likely to show
spontaneous resolution,
2- Renal U/S
3- DMSA
4- Check the Bpr , ht, wt, urine culture

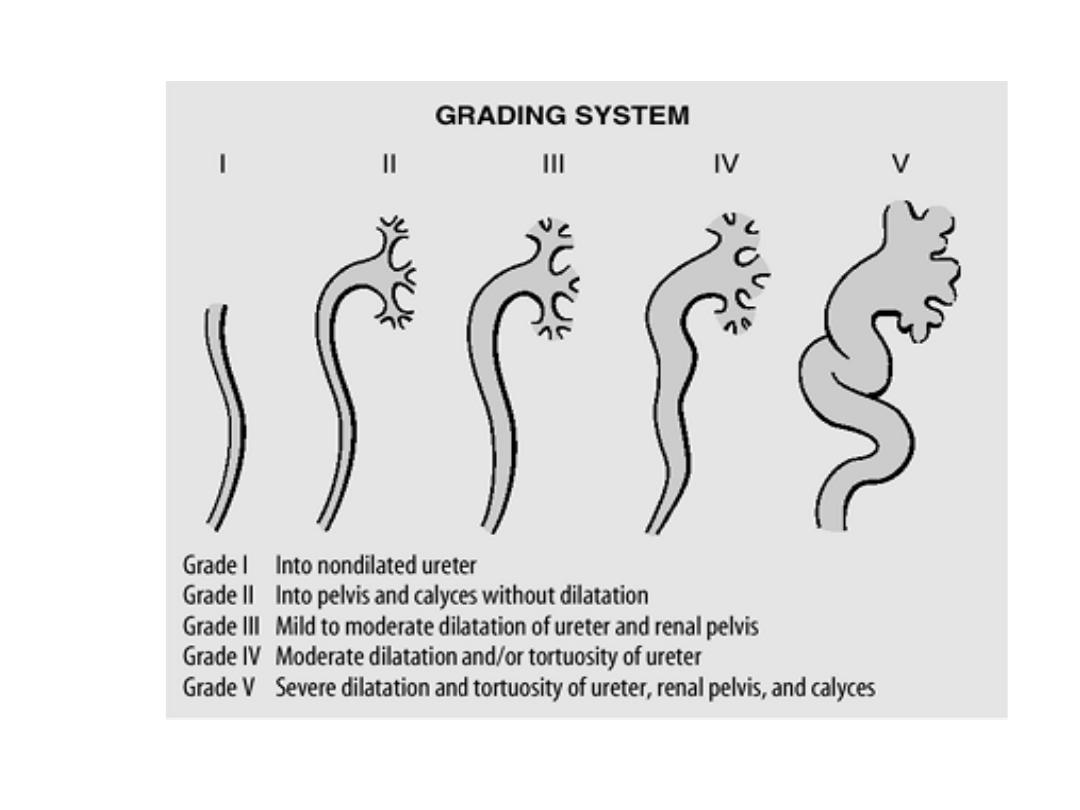
Natural History
1- Grade 1 and 2 ,whether uni or bilateral
spontenous resolution
2- Grade 3 younger age and unilateral
high rate of resolution
3- Grade 4 bilateral less likely to resolve
than unilateral
4- Grade 5 rarely resolve
The main age of spontaneous resolution is 6
years

▪Treatment
The goal are to 1- prevent pyelonephritis
2- renal insufficiency
3- others reflux complication
Treatment contain the following
➢ AB prophylaxis , urine culture
➢ VCUG every 12-18 month
➢ Check the Bpr , ht, wt frequently
The above medical treatment is successful when
❖ No infection.
❖ No scar .
❖ Reflux resolve
Surgical treatment
indicated in
➢ New scar
➢ Breakthrough UTI
➢ Not resolve at the age more than 7 year(failure of
medical treatment)
➢ Grade 4 and 5

THANK YOU