Basic Techniques and principles in plastic surgery
How to assess a reconstructive problem?
By(1):correct diagnosis.
(2): determine the extent and type of missing tissues.
(3): formulate a plan for reconstruction by using a
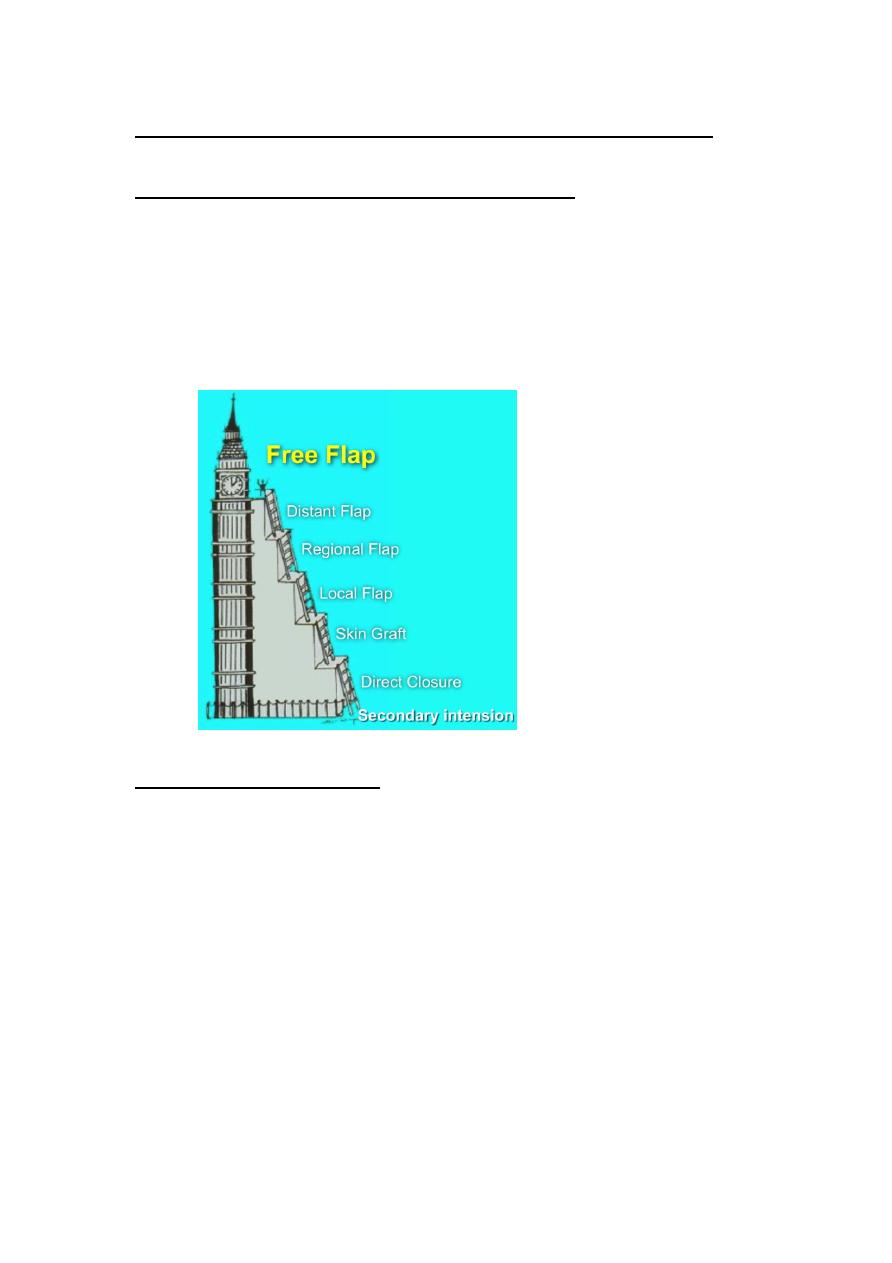
"Reconstructive Ladder”.
Reconstructive Ladder
: Begins with the simplest one followed progressively by
a more complex one.
: Healing by secondary intensiondirect
closure(primary intension)skin graftlocal
flapregional flap distant flapfree flap.
:some time a higher option is chosen e.g. local flap
chosen over a skin graft to reconstruct a nasal defect
because it may provide a superior result.
(we should put the reconstructive ladder in mind for
proper planning).
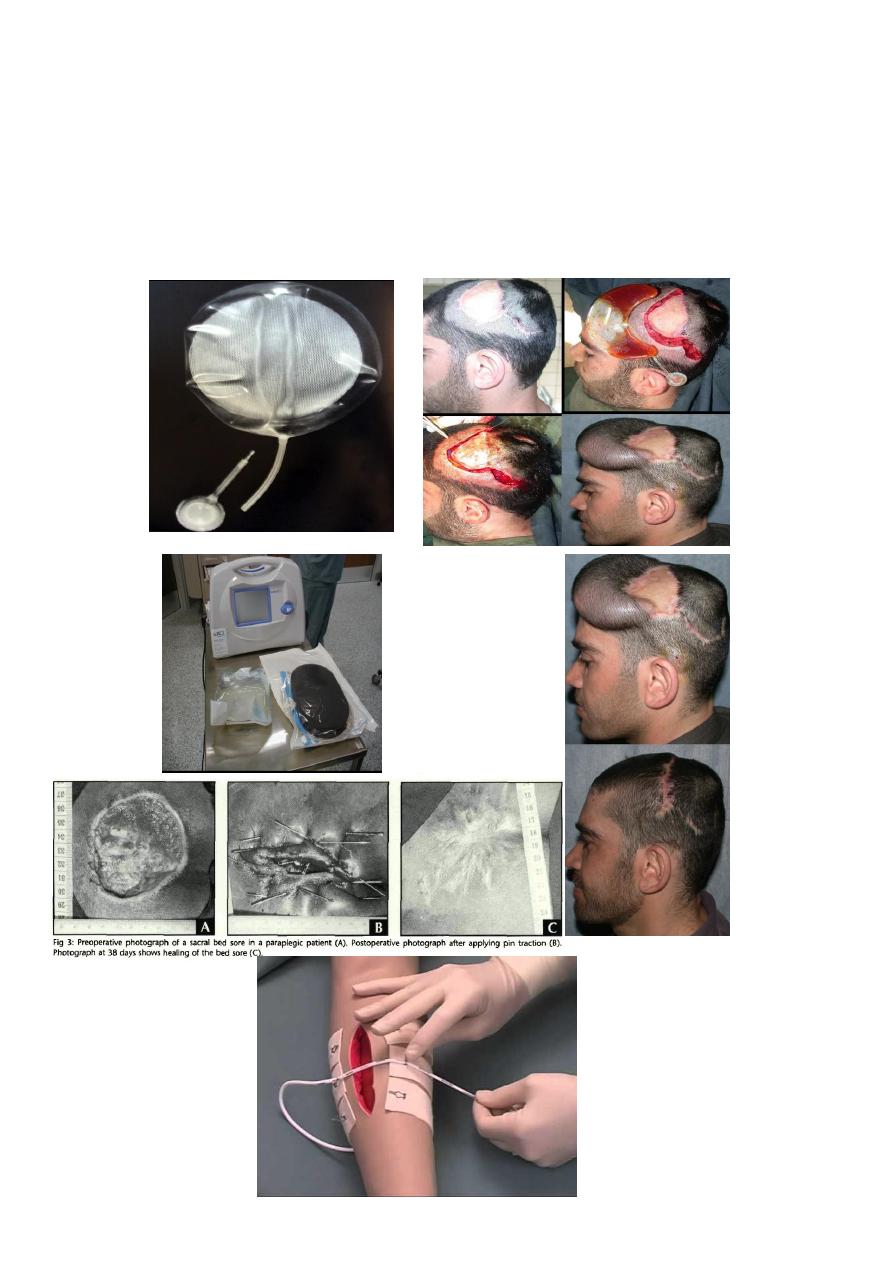
: Special procedures e.g. skin traction, pin traction using
stainless steel wires, tissue expansion, vacuum assisted
closure (VAC).
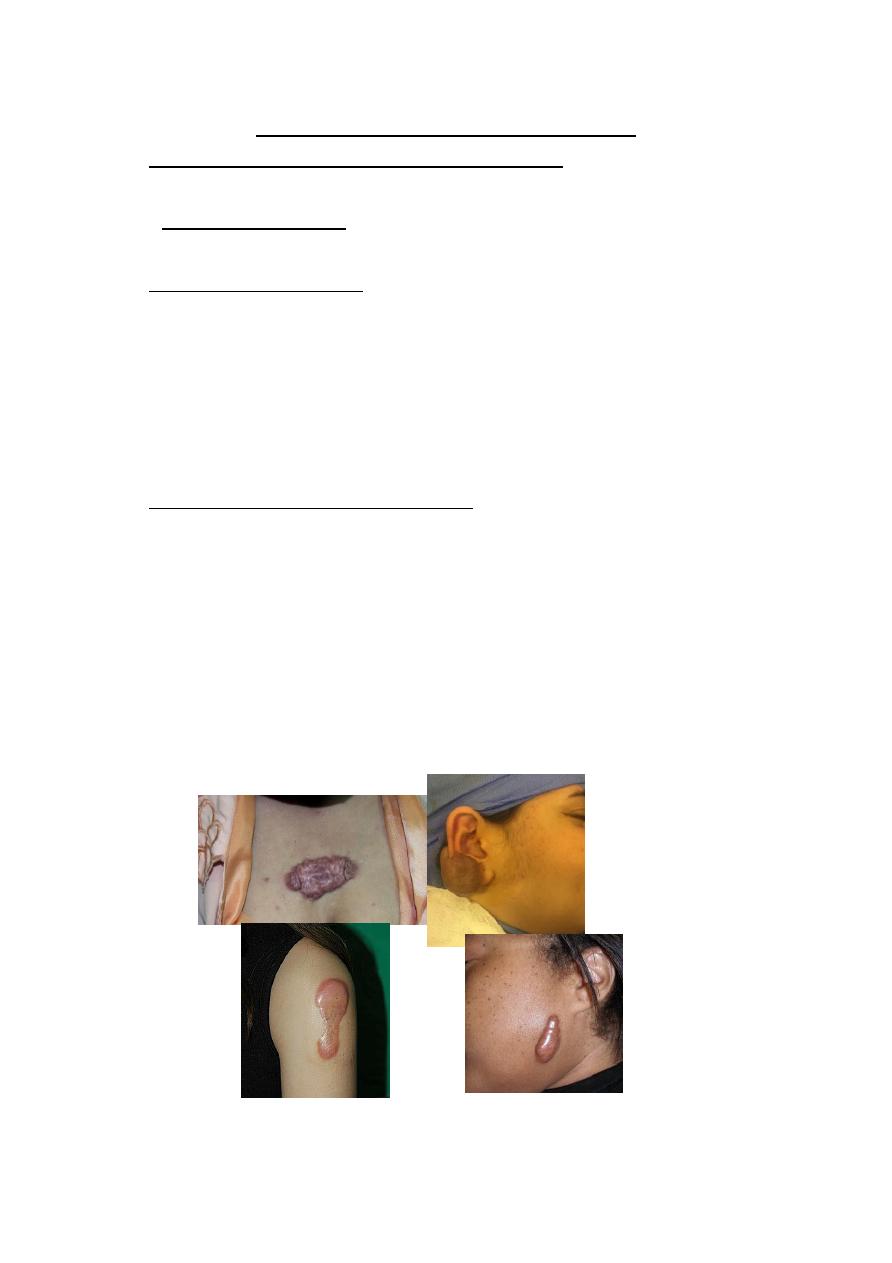
Factors influencing scar formation:
1. Race and Individual genetic makeup.
Keloid is more in Chinese and African.
2. Type of the skin:
Oily pigmented skin unsightly scar.
3. Age of the patient.
Skin loses its elasticity with increasing
agewrinklingso make scars in older pt less obvious
and less prone to stretching. As a rule, the quality of the
scar is better the older the patient is at the time of the
surgical excision.children's scars remain red and
hypertrophic for long periods of time.
4. Anatomical site on the body.
At extensor surface of joint e.g. knee , elbow, wrist
stretched scar.
While eyelids scars almost always heals with a fine line
scar.
Increased keloid risks at:
presternal area, especially in female.
Over the deltoid insertion at the shoulder.
Subcutaneous border of the mandible
External ear.
5. Co-morbid condition and nutritional status.
protein depletion, anemia.Affect wound healing.
vitamin A: reverse the healing retardation caused
by steroids.
vitamin C deficiency scurvy: characterized by
failure of collagen synthesis.
Zinc: required for epithelialization and fibroblast
proliferation.
Ferrous iron and copper: necessary for normal
collagen metabolism.
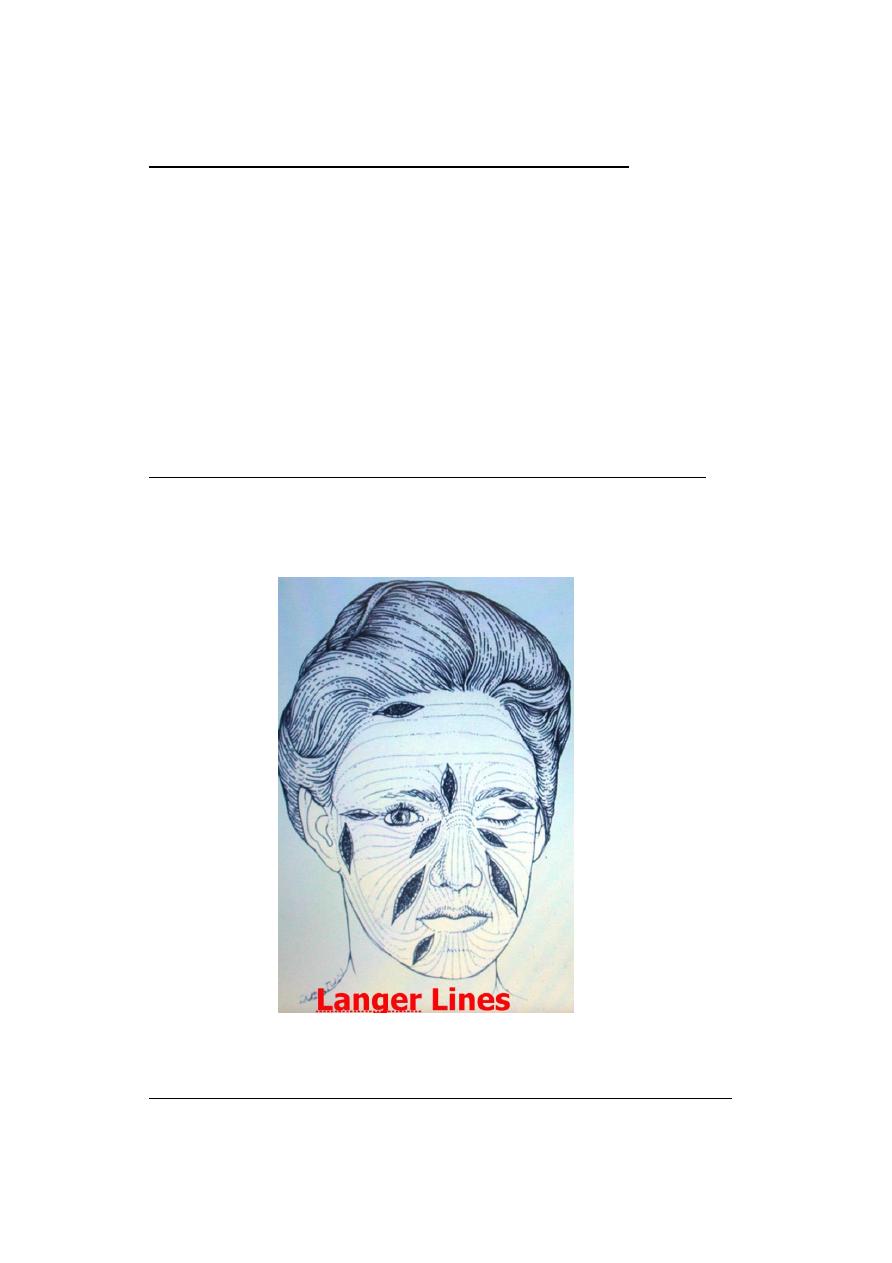
6. Placement of incision (i.e. direction of the wound) i.e.
proper planning.Parallel to Langer's line, relaxed skin
tension lines (RSTL).Wrinkle lines are generally the
same as the RSTL.
7. Surgical techniques used for closure of skin wounds.
Notice: Ultimately, however, scar formation is
unpredictable even with meticulous technique.
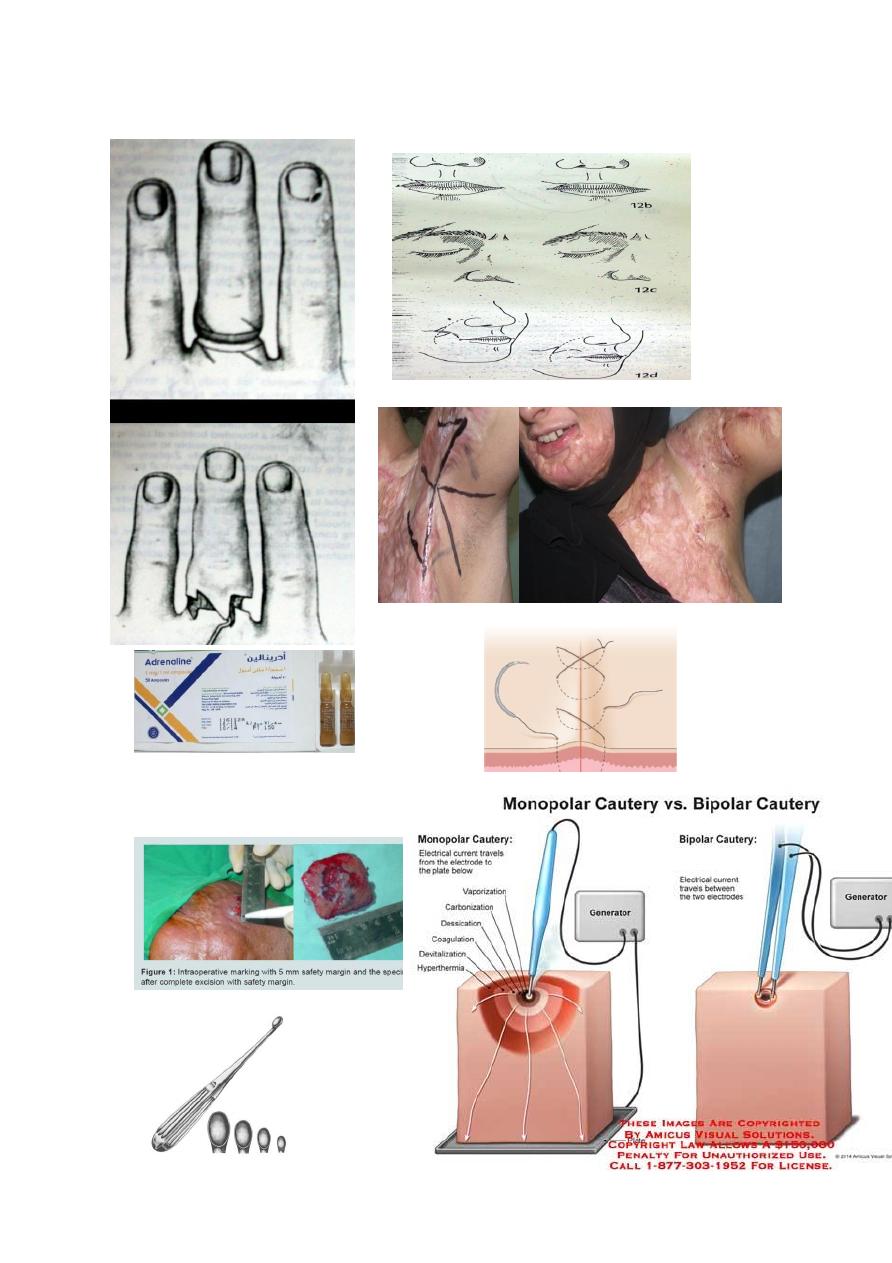
Surgical techniques used for closure of skin wounds
(1): Adequate local anesthesia: with or with out diluted
adrenaline, except in digit.
(2): Correct preoperative planning:
Will confirm whether the wound can be closed
primarily without tension or need skin graft, local
flap…etc.Correct plan with removal of proper safe
margin in case of tumor resection e.g.
1mm in benign lesion, 5mm in BCC,10mm in
SCC,30 mm or more in MM.
(3): Proper hemostasis.:compression, ligation ,figure of 8
suture, unipolar and bipolar cauterization, cryo, diluted
adrenaline( as local infiltration or through compression
using saline/diluted adrenaline socked gauze)…..etc.
Avoid using adrenaline for finger injury because it may
cause ischemic necrosis.
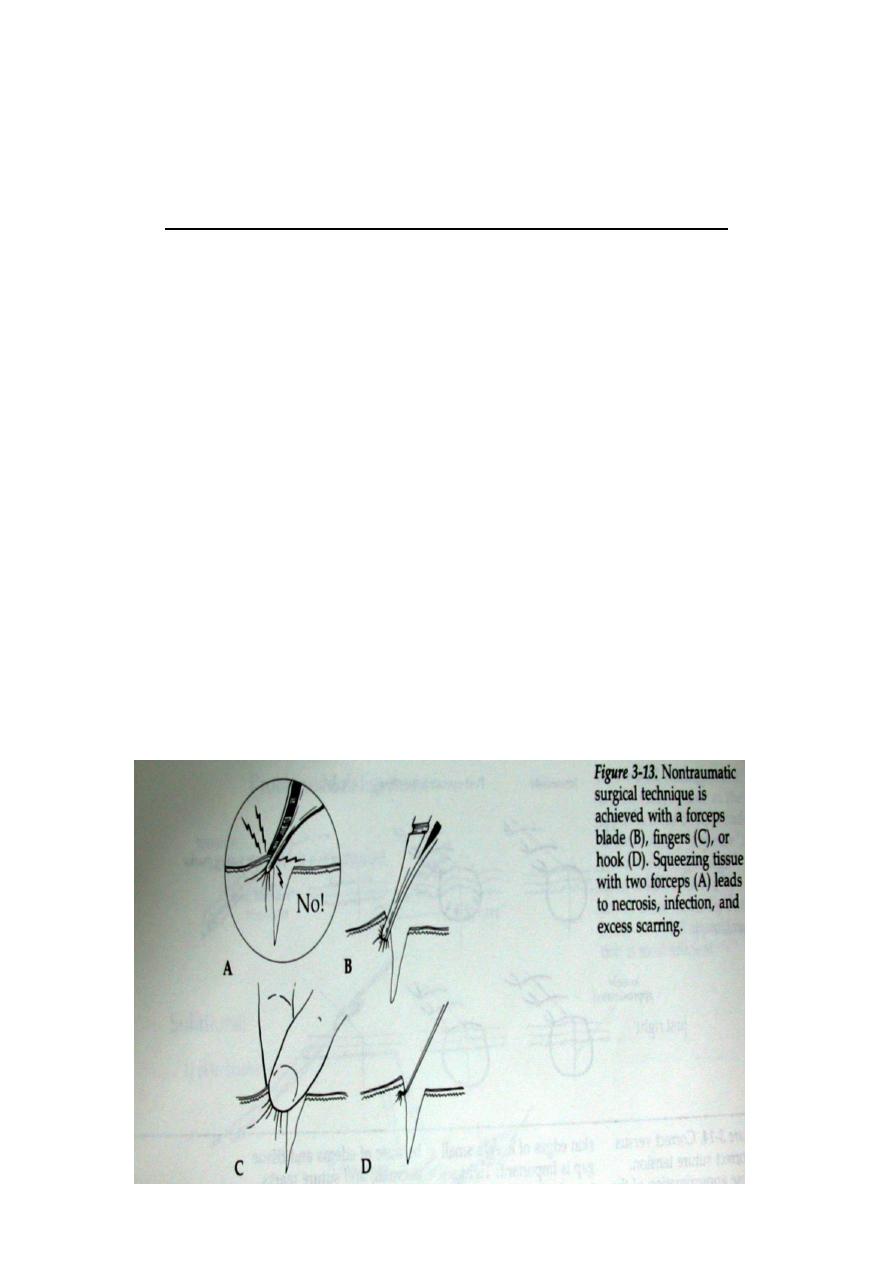
(4): Minimal damage to skin edge with atraumatic
technique.
(5): Debridement of necrotic tissues or foreign material.:
using gauze, back of knife, curette, varsajet , VAC also
for debridement, or using knife.
We have surgical (sharp and non-sharp debridement),
and non surgical debridement(e.g enzymatic debridement
using collagenase ointment).
(6): Irrigation: rapid jet lavage with normal saline.with
electric machine or wide bore syringe etc.
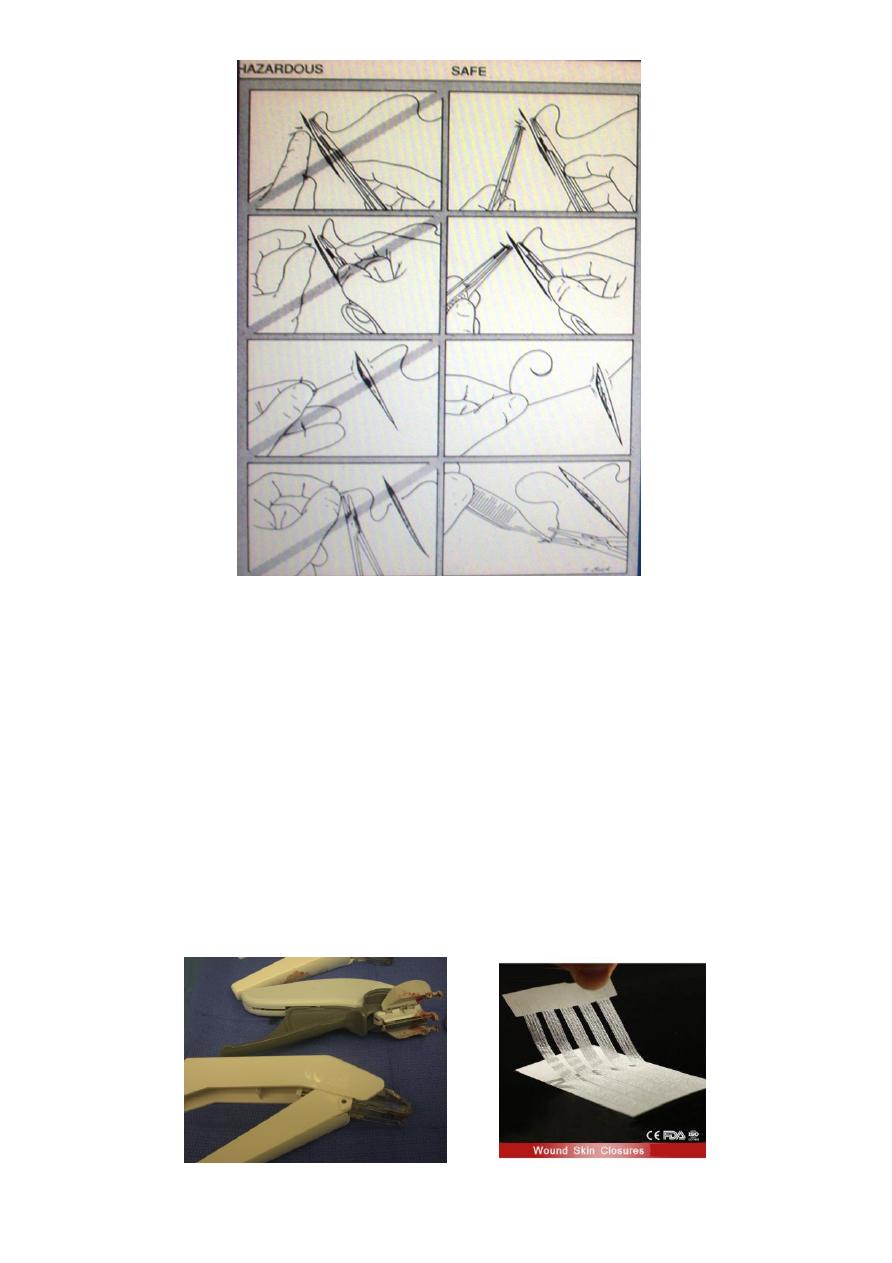
(7): Method of suturing (suturing techniques):
.Type of skin closure: sutures, staples, steristrips ,
wound adhesive.
.Tension free closure.
.Wound closed in layers.
.Subcutaneous fat sutures: reduce dead space but
have no effect on reducing Wound tension in the skin.
May lead to ischemia of the tissue and increase Risk of
infection.
.Dermal stitches: provide strength and relieve the
tension on the wound edges.
.All sutures that do not exit the skin should be
buried.(inverted stitches)
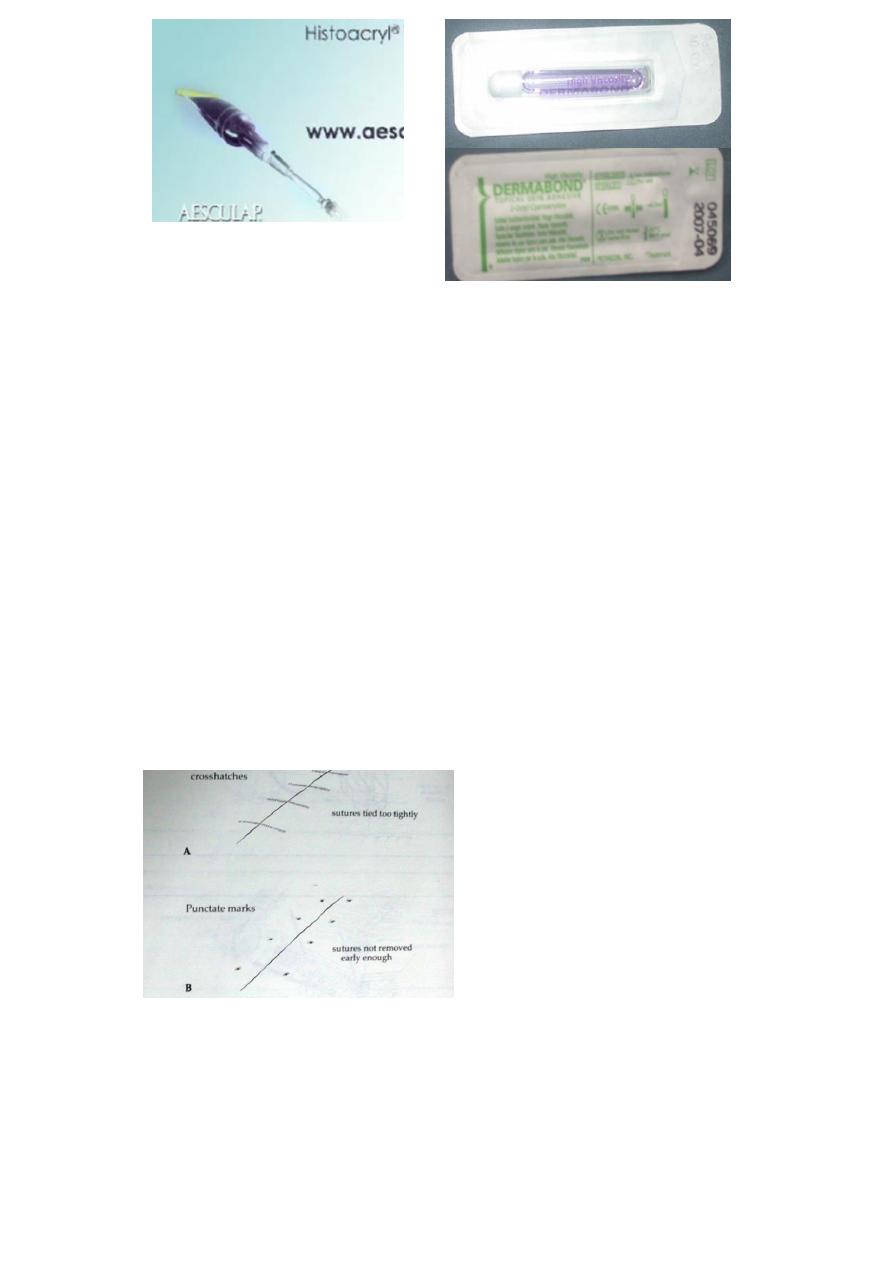
.Avoid (cross hatch stitch marks) and (punctate
marks).How: by appropriate suture selection, early
removal, sub cuticular stitches with steristrips or tissue
glue.

(8): Method of excision:
.Simple elliptical excision: 3/1 or 4/1 to avoid dog
ear.
.Wedge excision:
Excision of skin lesions in special anatomical areas e.g.
lips, eyelids, alar Margin of the nose i.e. lesions in close
proximity to an orifice should be Excised at right angle
to the margin of the orifice by a wedge excisionWhile
excision parallel to the margin will produce a deformity
like Ectropion.
1/3
rd
of lower lip and 1/4
th
of the upper lip and eyelids
can be excised With primary closure.
.Circular excision:
The defect closed with skin graft or local flap.
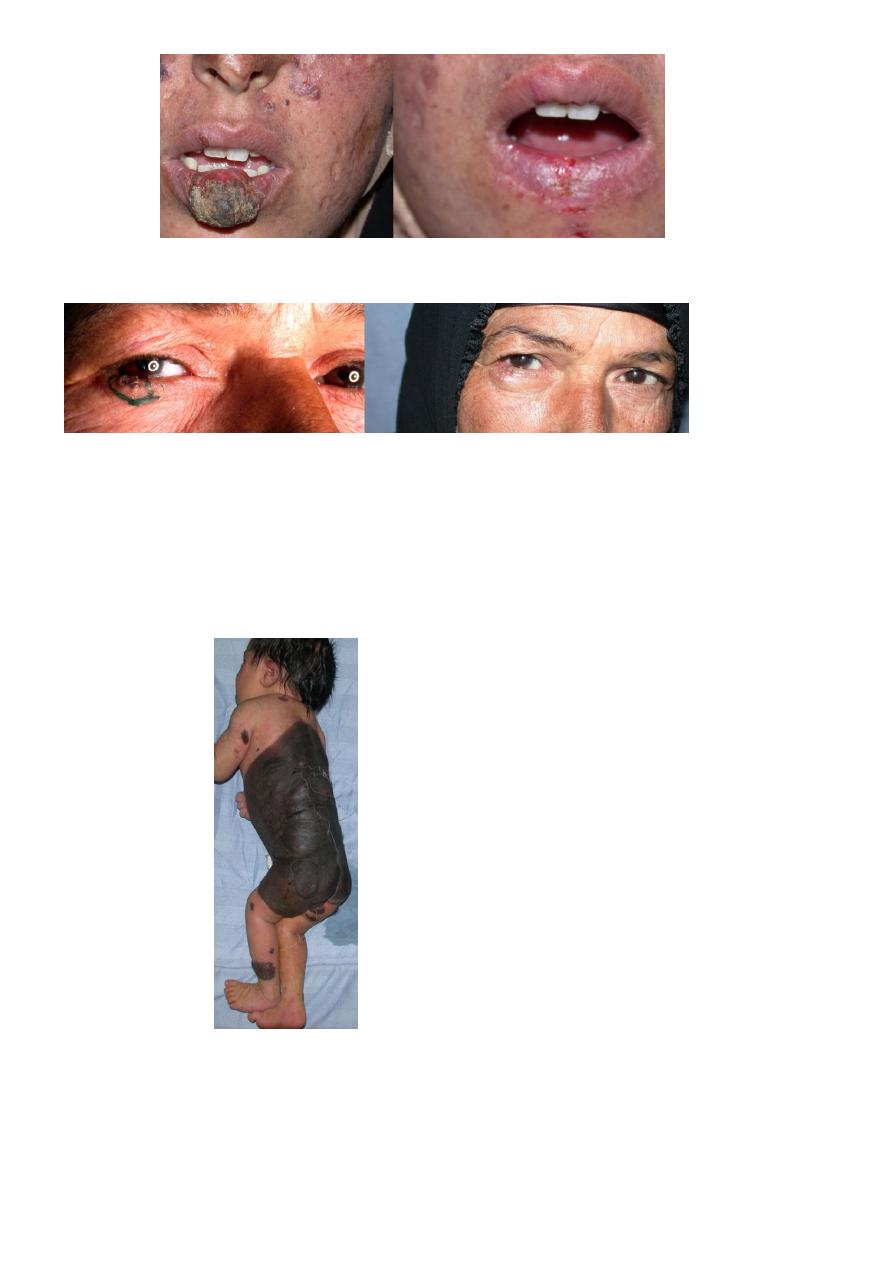
.Multiple excision technique:
Serial excision or tissue expansion is used for large
lesions e.g.Congenital hairy nevus.
(9): Scar revision by:
Z plasty , W plasty , Dermabrasion…etc.
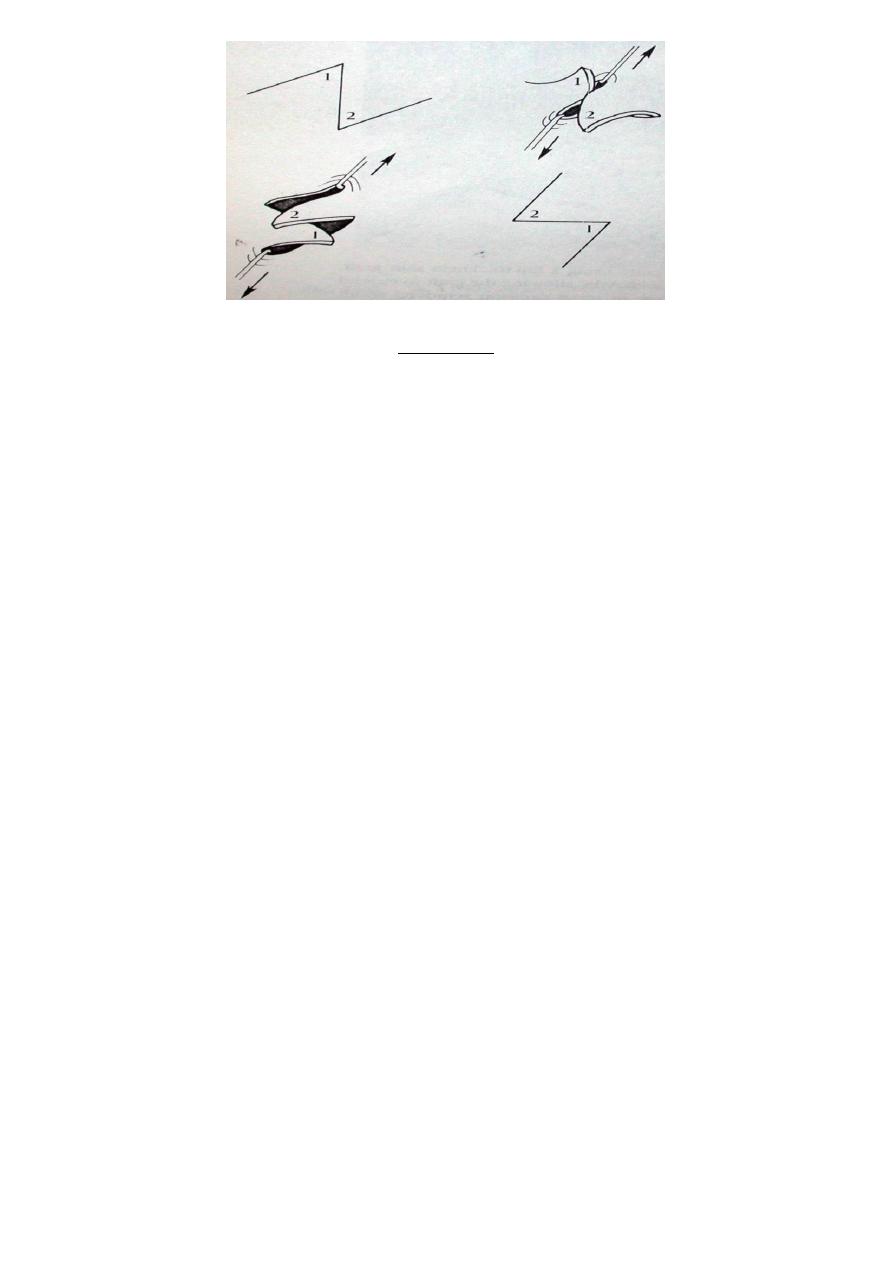
Z Plasty
.Is an ingenious principle used to: (Revise, Elongate,
Change direction) of the scar.
.Involve transposition of 2 triangular flaps.
.The limbs of the Z must be = to the central limb, but can
extend at varying Angles (from 30 to 90 degree) depend
on the desired gain in length.
.The classic Z plasty: 60 degree angle.Give 75%
theoretical gain in length of the central limb byRecruiting
lateral tissues. The actual gain is based on the
Mechanical properties of the skin and is always less.
.The resulting central limb after flap transposition will be
perpendicular to the Original central limb .In scar
revision, the final central limb should lie in the
Direction of the skin line and and should be selected
first.
.Uses:
1: Release of longitudinal scar contracture specially in
cases in which the scar
Crosses a flexion creases.
2: Multiple Z plasty break up the appearance of a
straight line scar e.g. at face.
3: Congenital skin webs.
4: (U shaped) or (Trap door) scars.
5: Circumferential scars e.g. constricting bands of the
extremities.