
Endometriosis & Adenomyosis

LEARNING OBJECTIVES
Understand the pathology of endometriosis and
recognize its involvement in chronic pelvic pain
Recognize the association between endometriosis and
subfertility.
• • Understand how to diagnose and treat
endometriosis.

Endometriosis

Definition:
• defined as the presence of endometrial
surface epithelium & or presence of
endometrial glands & stroma outside the
lining of the uterine cavity .

Incidence:
• Endometriosis occurs in approximately 5–10% of
women of reproductive age.
• It is most commonly found in the pelvis , on the
surface of the ovary , on pelvic endometrium ,
fallopian tubes & broad ligament .
• It may be seen in remote sites such as skin , joint ,
lung.Typical peritoneal lesion is described as a
powder burn .
• These ectopic endometrial tissues respond to the
clinical changes in ovarian hormones .

• It is a condition that is oestrogen dependent
and therefore it resolves after the menopause
or when treatment is directed towards
inducing a pseudomenopause.
Aetiology & pathogenesis:
•1- Menstrual regurgitation& :
Sampson’s implantation theory:
endometriosis result from the retrograde
menstrual reguargitation of viable endometrial
glands & tissue within the menstrual fluid &
subsequent implantation on the peritoneal
surface .

• Implantation of endometrium within
human surgical scars after caesarean
section
• or perineal repair following delivery
lends support to this theory

2-Coelomic epithelium transformation Meyer’s
‘coelomic metaplasia’ theory:
There is a common origin for the cells lining the
mullerian duct , the peritoneal cells & the cells of
the ovary . These cells return back to their primitive
origin & then transform into endometrial cells .

e32qe
3-Genetic & immunological factors :
increased incidence in first degree relatives of
patients with the disorder . Racial differences
(increase in oriental women (japenese ) . a low
prevalence in women of Afro-Caribbean origin.
4- Vascular & lymphatic spread :
vascular & lymphatic embolization to distant sites
such as skin , joints , kidney , & lung.

•Clinical features
• Endometriosis occur in women throughout their
reproductive years (20-50 years). They are characteristically
nulliparous & often have delayed their child - bearing , high
socio - economic status .
• The symptoms may vary depending on the site of ectopic
endometrial lesion , but there is a lack of correlation
between the apparent extent of the disease , & the
intensity of symptoms.

• Classical clinical features are severe cyclical non-
colicky pelvic pain restricted to around the time of
• menstruation, sometimes associated with heavy
menstrual loss. Symptoms may begin a few days
before
• menses starts until the end of menses.
• Deep pain with intercourse (deep dyspareunia) and
on defaecation
• (dyschezia) are key indicators of the presence of
endometriosis deep within the pouch of Douglas.

Endometriosis and infertility
• in the more severe stages of endometriosis, there is
commonly anatomical distortion, with
• periadnexal adhesions and destruction of ovarian
tissue when endometriomas develop.
• A number of possible and variable mechanisms
have been postulated to connect mild
endometriosis with
,infertility including negative effects on ovarian
reserve,
• ovulation dysfunction, sperm survival in the female
• genital tract and egg quality (and thus embryo
quality).

Endometriosis and infertility
• medical treatment of endometriosis does not
improve fertility
• and should not be given to patients wishing to
conceive.
• However, surgical ablation/excision of minimal and
mild endometriosis does improve fertility chances.
• leave endometriomas alone prior to IVF unless they
are symptomatic or reduce
• access for egg collection

Symptoms
site
• 1-female reproductive dysmenorrhea ( secondary
or congestive )
• tract
• lower abdominal & pelvic pain dysparenunia (deep
rupture or tortion endometrioma
• lower back pain
• infertility (30-40% )

2-urinary tract cyclical haematuria ,
dysuria
ureteric obstruction
3-G.I.T cyclical rectal bleeding .
obstruction
4-surgical scars
umbilicus cyclical pain & bleeding
5- lung cyclical haemoptysis
haemopneumothorax

Differential diagnosis
1-Adenomyosis
2-PID
3-CA.of colon or rectum
4- CA. of ovary
5- Pelvic congestion syn.

Staging:
American Fertility Society's Scoring System to
classify endometriosis
Stage 1 (minimal) = 1-5
Stage 2 (mild) = 6-15
Stage 3 (moderate) = 16-40
Stage 4 (severe) =>40

Staging:
American Fertility Society's Scoring System to classify endometriosis
1-Peritoneum:
Endometriosis < 1cm 1-3 cm >3cm
score 1 2 3
Adhesions filmy dense with partial
Obliteration of pouch
Of Douglas dense
With Complete
obliteration
score 1 2 3

2-ovary
Endometriosis <1cm 1-3 cm > 3 cm or
ruptured
endometrioma
right score 2 4 6
left score 2 4 6
Adhesions filmy dense with partial dense with
enclosure of ovary complete
enclosure Of ovary
right score 2 4 6
left score 2 4 6

• 3-Tube
• Endometriosis <1cm >1cm tube occluded
• right score 2 4 6
• left score 2 4 6
• Adhesions filmy dense with dense with
tube distorded tube occluded
• right score 2 4 6
• left score 2 4 6

Sites of endometriosis
ovarian endometriosis:
This is the most common site for endometriosis,
the lesions may be either superficial or deep.
Superficial form :
haemorrhagic lesions , red vesicles , or blue - black
powder burn lesion .
Deep lesions (severe form) :
Endometrioma or chocolate cyst : arises from the
characteristic dark brown chocolate - coloured
content of the cyst arises from repeated menstrual
bleeds .

Diagnosis:
1-Clinical finings
• is suggested by the clinical findings of thickening or
nodularity of the uterosacral ligaments , tenderness
.
• Endometriosis in the pouch of Douglas , an ovarian
mass & a fixed retroverted uterus .
• However, a specific diagnosis requires visualization
& in uncertain cases , biopsy of lesions , either at
laparoscopy or laparotomy .

2- Non - invasive tests
a-Ca 125 level : non - specific.
b- ultrasound : is of limited value , helpful when
there is endometriomas or chocolate cysts) .
c- MRI : is of little benefit also , useful when
there are ovarian cyst , or invasion of
surrounding organs such as bowel , bladder ,
recto - vaginal septum

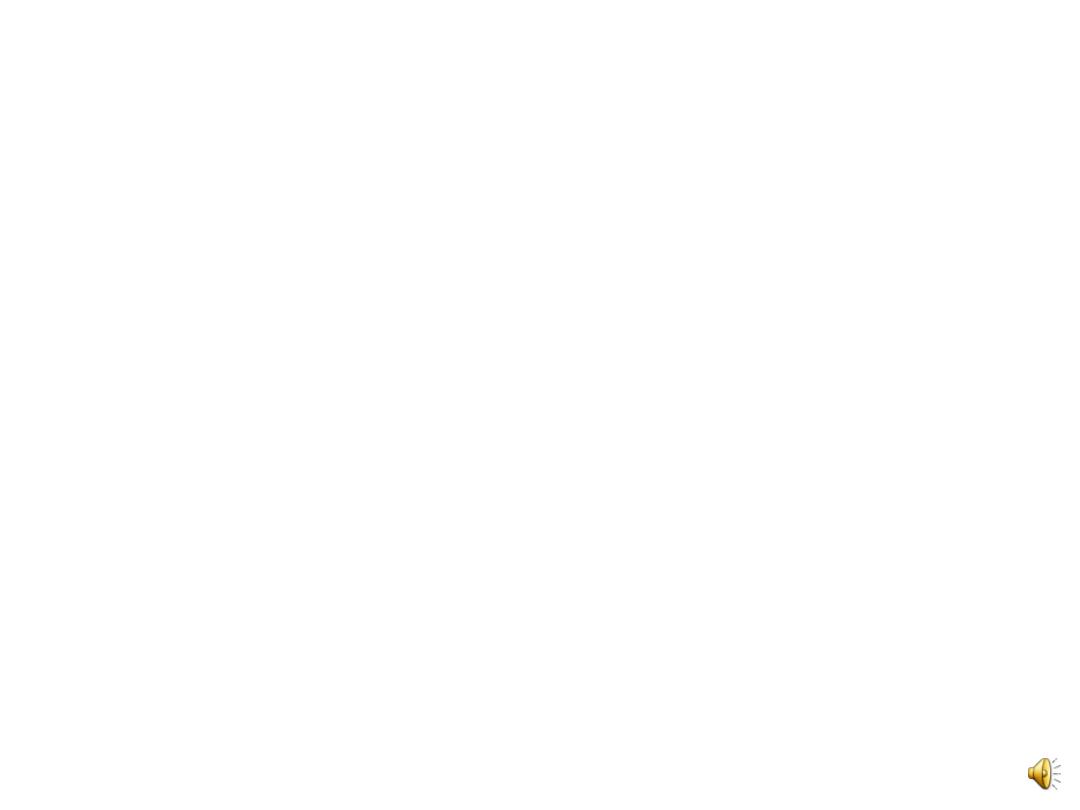
3- Laparoscopy: remains the gold standard means of
diagnosing endometriosis . endometriotic lesions
can be red, puckered, black ‘matchstick’ or appear
white and fibrous.
Role of laproscopyis vital:
a. provides direct visualization of endometriotic
lesions .
b. possibility to biopsy suspected areas .
c. allow staging of the disease .
d.It allow concurrent therapy at the time of
laproscopy in the form of cautery or laser treatment
in selected cases .
d. Allow checking patency of fallopian tubes.
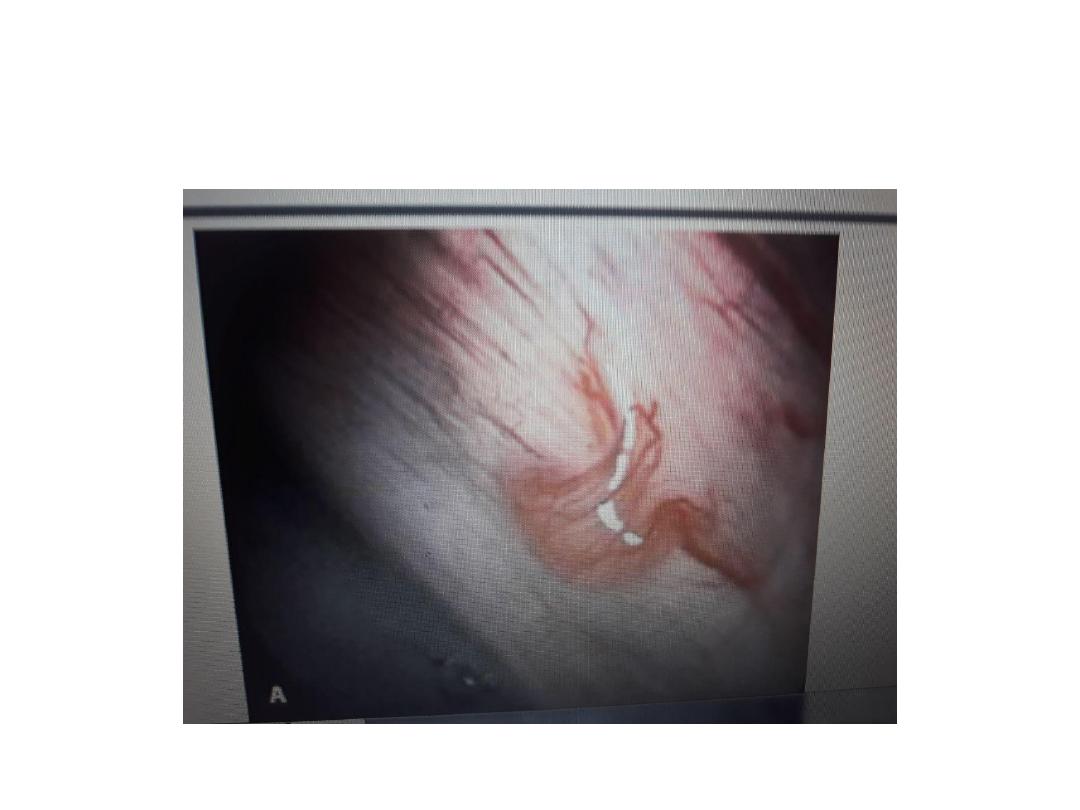
A: Red lesions on peritoneum
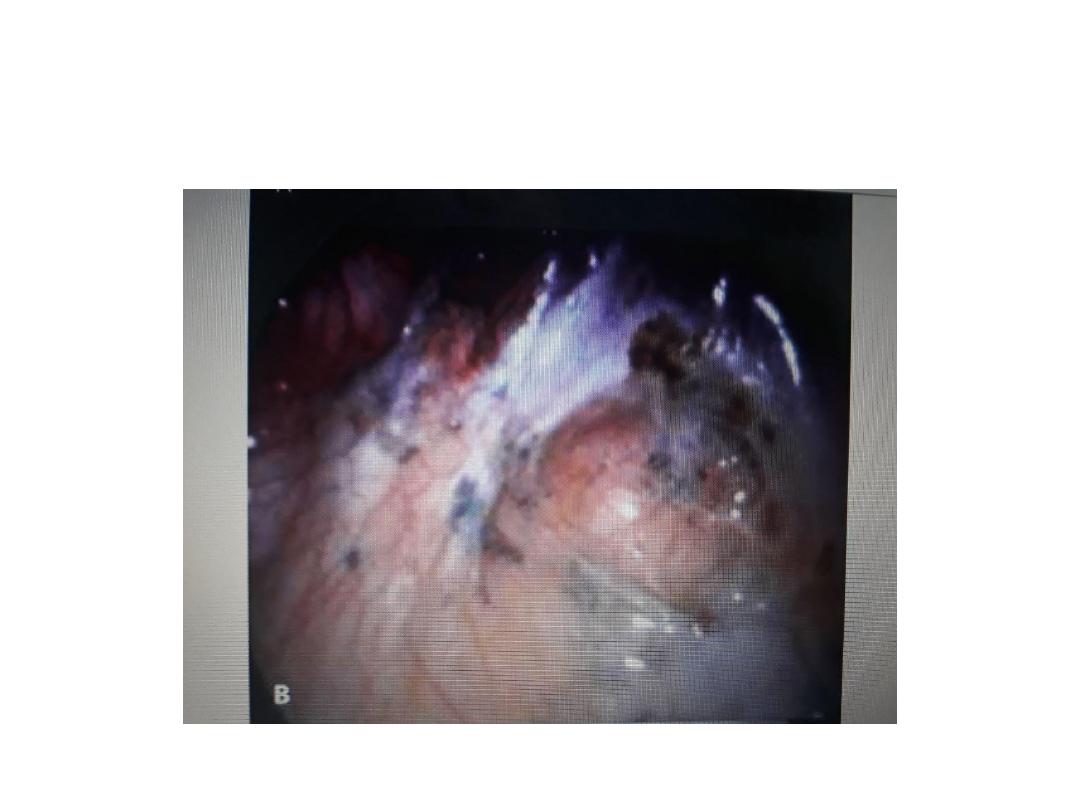
B: black ‘matchstick’lesions
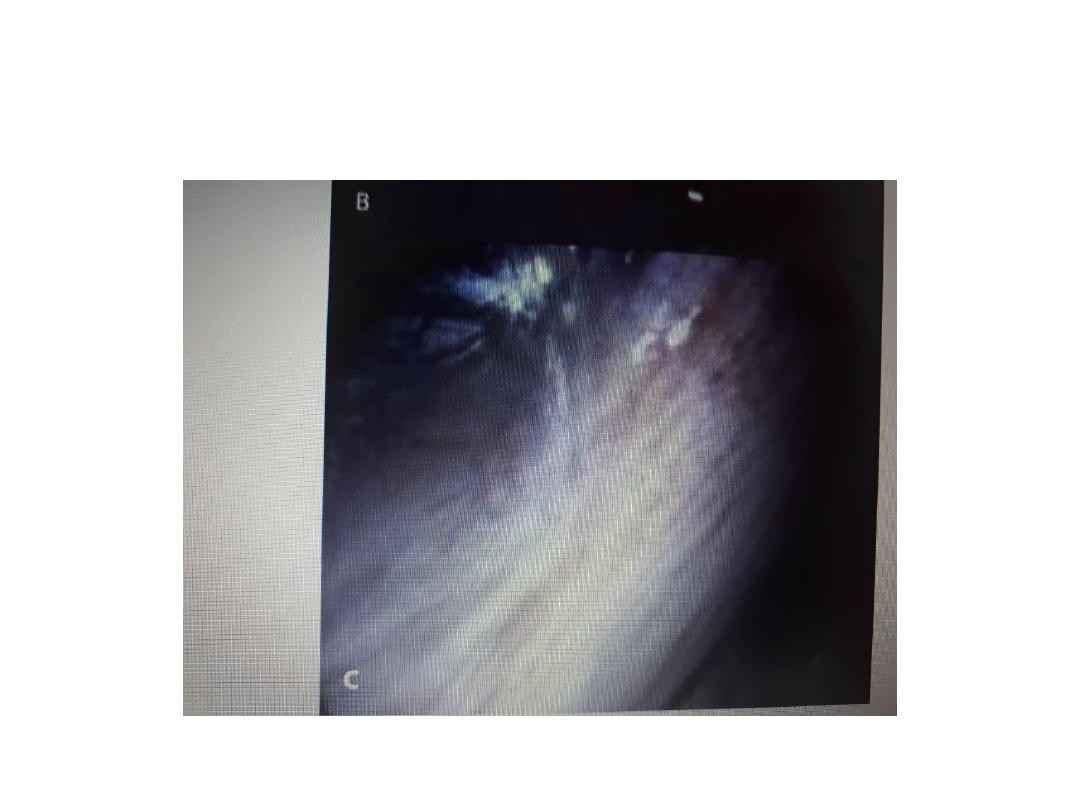
C: white fibrous lesion.

Treatment
Surgical or medical or combination of both. choice of
treatment depend on age of patient , reproductive
wishes , severity of symptoms , site & extent of her
endometriosis .
The therapeutic aims are:
1. to relieve pain .
2. to permit satisfactory coitus .
3. to control abnormal bleeding .
4. to promote the possibility of pregnancy if the
endometriosis is severe enough to interfere with
infertility .

Prophylaxis:
1. Oral contraceptive pills.
2. Patients who have a strong family of
endometriosis should be encouraged to
attempt pregnancy sooner rather than later.

Treatment
1- Drug therapy:
a. NSAID
are helpful in reducing the severity of dysmenorrheal
& pelvic pain .
b. Hormone therapy:
medical treatment of endometriosis aimed at the
prevention of menstruation using sex steroids in
various ways . oestrogens , androgens,
progestogens , & combinations have been used .
:

• 1.COC
• use of continuous COC & in increasing dosage
for up to 9 months to induce a state of
pseudopregnancy ; with anovulation &
amenorrhea , would lead to necrosis &
absorptiopn of decidualized endometriosis .
S/E weight gain , nausea , vomiting ,
breakthrough bleeding .

2-Danazole & Gestrinone :
it is mild androgenic , antiprogestogenic ,
antigonadotrophic , immunosuppressive effect ,
also has direct inhibition of endometrial cell
growth, used in the past but are no longerv
appropriate.
Dose Danazole 400 -800 mg / day
Gesrinone 2.5 mg twice weekly
used in courses for 3 - 6 months .
S/E androgenic S/E e.g. weight gain , greasy skin ,
acne, deepening of voice .
longer - term administration may leads to
alterations in lipid profile , or liver function , which
needs to be monitored .

3- progestogens
such as medroxyprogesterone acetate or
dydrogesterone .
given on continuous basis and the levonorgestrel
intrauterine system (LNG-IUS) (Mirena) .
4- GnRH agonists
Temporary induction of pseudo - menopause . used
as intranasal or subcutaneous routes or slow -
release depot formulation for one month .
S/E hot flush , night sweats , atrophic vaginitis , long -
term use may leads to osteoporosis .

• a newer class of drug called aromatase inhibitors
that inhibit the
• action of the enzyme aromatase, which converts
androgens into oestrogens and is over expressed in
endometriotic tissue.
• Further research needed to be used in refractory
cases.

Surgical treatment
Conservative or definitive.
1. Conservative surgery
Through laproscopy or open surgery . By eradicate
vissible endometriotic lesions with diathermy or
laser . also endometrioma treated in 2 ways either
the cyst opened & drained , & base lasered , or do
ovarian cystectomy .
lysis of tubo - ovarian adhesions or do salpingostomy .
2- Definitive (radical ) surgery : TAH & BSO
indications
a. severe symptomatology

b.progressive disease .
c.women whose families are complete .
d. large adherent endometriotic cyst.
e.patient with deep - seated endometriosis involving
the bowel or bladder .
so endometriosis remains a disorder of little hope of a
perminant cure , & one with repeat recurrences
throught the reproductive life .
Malignant changes in endometriosis is very rare ,
usually involves ovarian endometriosis . it is either
endometriod ca. or adenocanthoma.

Adenomyosis
is a disorder in which endometrial glands & stroma
are found deep within the myometrium.
Predisposing factors
1. usu. occur in multiparous women ; repeated
pregnancies may predispoes to extension of
endometrium into the myometrium .
2. Age; in late thirties or early forties ( near the end
of reproductive life ).
3. Vigorous curettage; may leads to damage of the
uterine wall, thus allowing acess by the
endometrium
4. Cystic glandular hyperplasia of the endometrium .
5. High socio - economic status

Pathology
uterus is usu. enlarged (symmetrical enlargement ) ,
lesion may be localized or diffuse .
Clinical features
the principal symptom is menorrhagia (perhaps from
interference with normal uterine haemostatic
mechanisms) , progressive secondary
dysmenorrhea , pelvic discomfort , & dysparunnia.

Diagnosis
is difficult pre -op.
1. Ultrasound; may be useful when adenomyosis is
marked & localized to one area.
2. MRI
•
3. Pathological examination of the hysterectomy
specimen . where it is identified in 40% of uteri
from a general female population of reproductive
age.
Treatment
Conservative surgery & medical treatment poorly
developed .
Hysterctomy ; is the only definitive treatment .