


INSTRUMENTAL DELIVERY
DEFINIFITION: delivery of a baby vaginally using an instrument for assistanceINDICATIONS:
1.fetal indication: fetal distress or cord prolapse during the second stage of labor, malposition of fetal head
2.maternal indications: maternal exhaustion and distress during second stage of labor or certain maternal medical disease that necessitate shortening second stage like heart disease
3.ellective use in epidural anesthesia, premature baby, delivery of after coming head in breach vaginal delivery.
FORCEPS DELIVERY
Classification1.low forceps(Wrigley's)
. short and light
. used if deeply engaged head
. used in caesarian section
2.mid cavity non rotational forceps (Simpsons)
. engaged head
. direct occiput anterior
3.midcavity rotational forceps (Keillands)
. engaged head
. reduce pelvic curve on the blades of the forceps allow rotation about the axis of the handle
. help to correct asynclitism and malposition
. must only attempt by an experienced operator
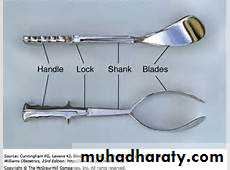
Forceps vary in size and shape
Consist basically two crossing branching introduce separately into the vagina
Each one has four components: plate shank lock handle
Shank short or long, plate contain cephalic and pelvic curve

Condition necessary for application of forceps
1.fully dilated cervix2.rupture membrane
3.suitable presentation (vertex, mentoanterior face)
4.position is well known
5.the head must be engaged
6.empty bladder
7.exclude obstruction :no obstruction below the head
Technique of use
.adequate analgesia or anesthesia.female in lithotomy position
.identification of position of fetal head by feeling sagittal suture and fontanel
.application of forceps after checking both plate of the forceps outside the pelvis and locked them .the left plate is introduce by the left hand into the left side of the pelvis and the right by the right hand in the same way .then two handle should be articulated and attached each other without difficulties .then gentle intermittent horizontal traction with each contraction until the vulva extended by the occiput then episiotomy done then the handle gradually elevated and pointed up

Complication and danger:
Maternal: trauma to birth canal (rupture uterus, cx tear, cx evulsion, multiple vaginal tear ). postpartum hemorrhage
.infection
.injury to bladder ,rectum or fistulae
.uterovaginal prolapse
Infant :trauma and death or long term morbidity, cerebral palsy, low IQ ,ICH,frature skull
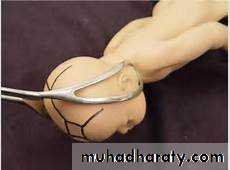
Vacum extractor (ventose )
Is that a suction cup of silastic or rigid construction of three different size 4,5,6 cm in diameter is connected via a tubing to vacume source ,either directly through the tubing or via connecting chain direct traction can then be applied to presenting part to expedite delivery

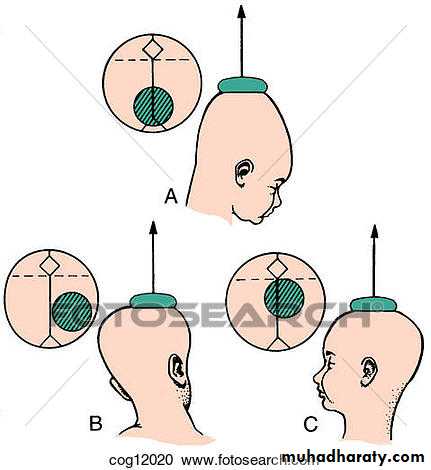
Technique: prior to application checking the patient in regard to dilation, presenting part, station and position. empty bladder, local analgesia or anesthesia. After checking the equipment for a leak the cup is placed in the vagina as closed as possible to the posterior fontanel over the sagittal suture .negative pressure of 0.2 kg\cm2 is applied and is increase gradually within 1 -2 reaching o.8 kg \cm2 traction applied in the same direction of birth canal with each uterine contraction the handle should be held perpendicular to the cup ,the thumb of the other hand is applied on the cup to counteract destruction in order to avoid cup dislodgement .the presenting part should be descend with each pull and the cup should not be dislodged more than one .if the baby is not delivered within three pulls and within 15 minute the procedure should be stopped
INDICATION
FETAL DISTRESS in the second stage of labor i.e fully dilated cervix or near fully (8 cm )
Maternal indication :physical distress ,medical disease that necessitate shortening the second stage like maternal cardiac disease
Contra indication :
. absolute cephalopelvic disproportion
.malpresentation face ,breech ,transverse lie
.cervix is insufficiently dilated
.premature fetus
.if suspected fetal coagulopathy and should be perform with care if prior scalp sample was perform during labor
Complications
Maternal :postpartum hemorrhage and genital tract laceration and injuries
Fetal :
.ICH greater incidence in premature and its related to number of pulls and duration of cup application
.cephal hematoma is commonly associated with ventose
.cerebral irritation and asphyxia
.scalp effect :scalp laceration and avulsions rarely alopecia on long term sequellae ,formation of shignon which its artificial cuput
.retinal haemorrhge
.neonatal jaundice due to degradation of large volume of blood in the cephalhaematoma
.long term morbidity :less than with forceps (neurological and intellectual development )
Episiotomy
Definition :is an incision through the perineum made to enlarge the vulval outlet and assist child birth
Types of episiotomy
.Medio lateral episiotomy extents from the fourchette laterally
Midline episiotomy :extends from the fourchette towards the anus
Indication :
.complicated vaginal delivery (breech ,shoulder dystocia ,forceps ).if there is extensive lower genital tract scarring (female genital mutilation ,poorly healed third or forth degree tears )
.when there is fetal distress
Complication :
.bleeding .haematoma .pain .infection .scarring .dyspareunia .rarely fistulae formationTechnique :
.is performed in the second stage usually when the perineum is being stretched.good analgesia if no epidural anesthesia
.incision is made mid line or Medio lateral involving skin ,perineal muscle ,vaginal wall (second degree tear )
.after delivery of the fetus and the placenta the incision is repaired in layer
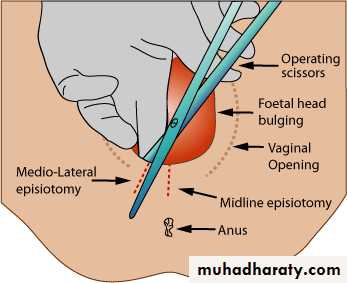
Mid line episiotomy less bleeding, rapid healing, less scaring. easy to repair but there is risk of extension to the anal sphincter and anal canal so Medio lateral episiotomy preferred
KEY POINT
.should only be used by those trained to do so.the prerequisites for an instrumental delivery must be met before forceps or ventouse be applied
.failure rate higher with soft than rigid cups and with ventose than forceps
.use of second instrument increases the risks of fetal and maternal damage.ventose safer to the mother than forceps
Forceps safer to the fetusCephalhaematoma and retinal detachment common with ventose
.forceps used in face ,after coming head in breech ,casseran section while ventose not
.ventose can be used in near fully cervix while forceps not