


Disorders of the kidneys
AgenesisBilateral renal agenesis is extremely rare.
The children don’t survive.
One kidney may be absent (estimated incidence 1 in
450-1000 births).In some cases may be because the ureteral bud
fail to develop, or fail to reach the metanephros
The ureter and vas are abscent in 50%of affacted site
It accidantaly dignose by imagingHypoplasia
Hypoplasia implies a small kidney.differentiation from acquired atrophy( as post vesicoureteral) is difficult.
Such kidneys have small renal arteries & branches & are associated with hypertension, which is relieved
by nephractomy
.
Dysplasia & multicystic kidney
Renal dysplasia is histologic diagnosis (abnormal
metanephric differentiation) the kidney may be small or large in size & contain local ,diffuse or segmentallyarrange primitive structures, it may affect all or only part of the kidney,
Cystic dysplasia :cyst of various sizes present
Multicystic kidney when the entire kidney is dysplastic with preponderance of cystsmulticystic dysplastic kidney.
Is most common renal cystic diseaes and second cause of abdominal mass after PUJ obustraction-Usually unilateral
-nonhereditary
-the ureter is usually absent or atretic.
it may develop because of faulty union of the nephron with the collecting system.
The only finding is the discovery of irregular mass in the flank.
Diagnosis by U/S
if the physician feel that the proper diagnosis has been made, no treatment is necessary.
If there is doubt about the diagnosis, nephrectomy is
considered the procedure of choice.Polycystic kidney disease
Classified as autosomal dominant (adult) &autosomal recessive (infantile).
When polycystic kidney disease diagnosed in neonate most often recessive type,
50% of affected new born die in the 1st few hoursor days of life, the others will apparent at childhood up to13 & rarely up to 20 yr. & is bilateral.
Autosomal dominant (adult) polycystic kidney.
Almost always bilateral(95% of the cases),symptoms not appear until after age 40 yr.
cysts of the liver, spleen, or pancreas may be noted
The kidneys are larger than normal
Etiology &pathogenesis
The evidence suggest that the cysts occur becausethe defects in the development of the collecting, uriniferous tubules & in the mechanism of their joining.
As the cysts enlarge, they compress adjacent
parenchyma, destroy it by ischemia, & occlude normal tubules.The result is progressive functional impairment.
Clinical findings
Symptomsdrag pain by the heavy kidneys
obstruction
infection
hemorrhage into a cyst.
Colicy pain due to stones or clots
Gross or microscopic hematuria may occur.
abdominal mass.
Infection (chills, fever, renal pain)
Symptums of renal failure
Signs
one or both kidneys are usually palpable.-If infected they may be tender.
Hypertension is found in 60-70% of these patients.
Fever may be present if pyelonephritis exists or if cysts have become infected.
In the stage of uremia, anemia or loss of weight may be evident.
Laboratory finding
Anemia may be noted.Proteinuria & microscopic or gross hematuria are the rule. Pyuria & bacteriuria are common.
About one-third of patients are uremic when first seen.
x-ray findingBy IVP the renal masses are usually enlarged & (spider leg deformity).
Ultrasound is superior to excretory urographyCT scanning 95% of cases give an accurate diagnosis.
Treatment
conservative & supportive (proflactive).low protein diet
Good fluid intake
Physical activity is permitted but strenuous exercise is contraindicated.
Hypertension should be controlled.
Renal failure should be treated by dialysis or renal
transplant.
A large cyst compressing upper ureter causing
obstruction should be excised or aspirated.
Simple (solitary) cyst
Simple cyst of the kidney is usually unilateral & single but may be multiple & rarely bilateral.Whether its congenital or acquired is not clear.
Pain in the flank or back, usually intermittent and dull,is not uncommon
Renal ultrasonography is noninvasive diagnosticTechnique
CT scan is diagnostic
.
Clinical finding
Pain in the flank or back, usually intermittent & dull.cyst is usully symptmatic if it is 10cm and moreIf bleeding occur pain may come on abruptly & be sever.
The patient may discover mass in the abdomen,
If cyst become infected patient usually complain of pain in the flank malaise & fever.
Physical examination is usually normal, although aflank mass may be palpated or percussed.
Tenderness in the flank may be noted if the cysts
become infected.
Laboratory finding
Urinalysis is usually normal.Renal function tests are normal.
CT scan
Appear to be the most accurate means of differentiating renal cyst & tumor.Differential diagnosis.
Simple cyst should be differentiate from
-carcinoma of the kidney,-polycystic kidney disease,
-renal carbuncle,
-hydronephrosis,
Treatment
If the diagnosis can be clearly established, treatment is follow up by ultrasonography..
If the diagnosis is suspicious renal angiography or
needle aspiration of the cyst may be necessary.
Aspiration of the cyst or surgical excision of extrarenal part may be indicated in cases of complication like
obstruction , or infection.
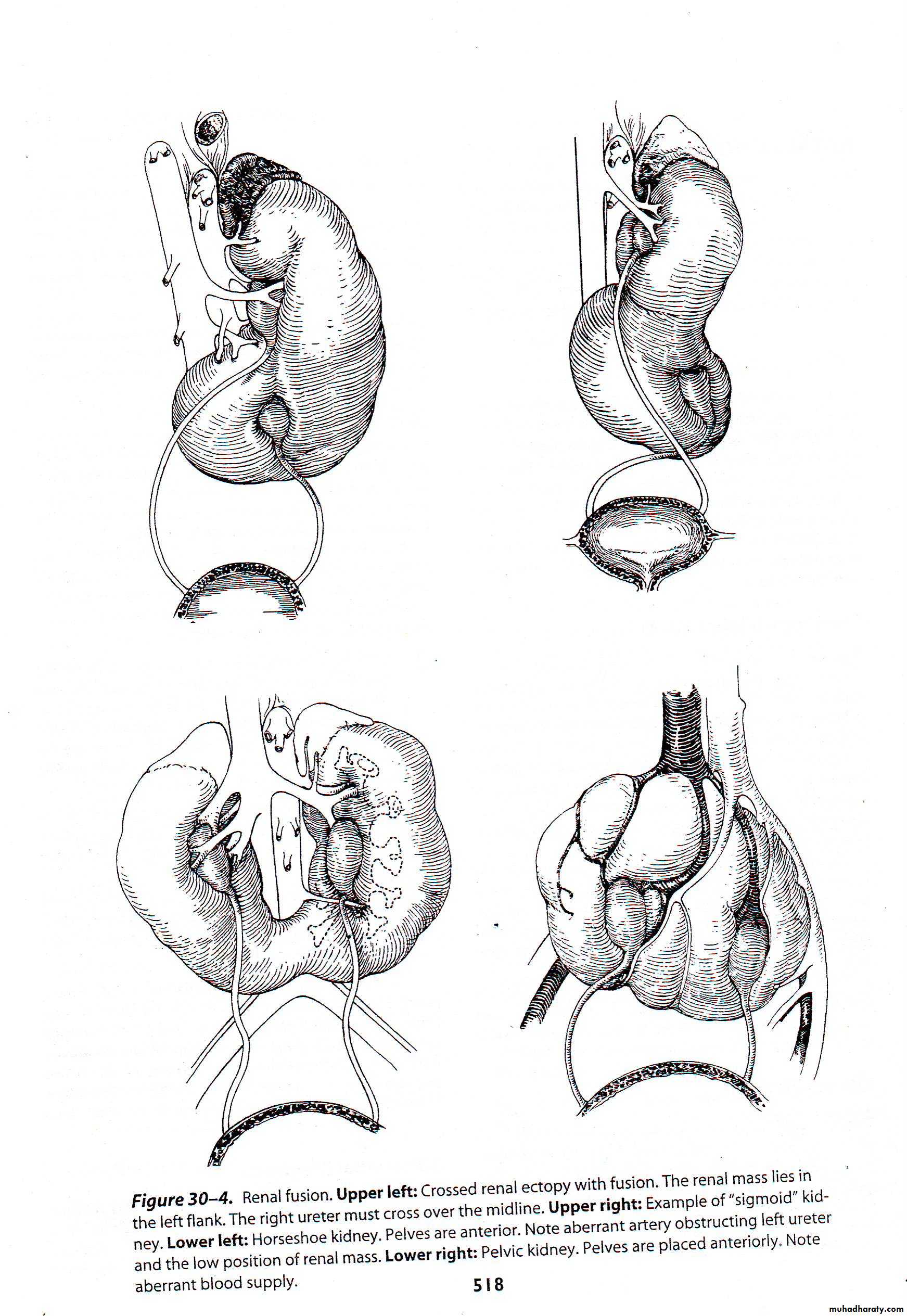
Renal fusion
About 1 in 1000 individuals has some type of renal fusion,
the most common being the horseshoe kidney.
The fused renal mass almost always contain 2 excretory systems & therefore 2 ureters.
the renal tissue may be divided equally between the 2
flanks, or the entire mass may be on one side.Even in the later case, the 2 ureters open at their proper places in the bladder.
Etiology & pathogenesis
It appears that fusion of the 2 metanephroi occurs early in embryologic life, when the kidneys lie low in the pelvis.Horseshoe Kidney
Both kidney fused by isthmus usually through their lower polesThe pelvis lies anterior
Thus the ureter must ride over the isthmus or traverse the anterior surface of the fused kidney.Some degree of uerteral compression may arise from
this or from obstruction by blood vessels.
Clinical features
Most patients have no symptoms.Symptoms develop if there is complication like : uerteral obstruction,infection,ston.
Physical examination usually negative unless theabnormally placed mass can be felt.
x-ray finding
in case of horseshoe kidneyThe renal mass lower than normal
-the axes of the 2 kidneys are vertical andparallel
-the renal pelves lie on the anterior surfaces of the
kidney masses,
-the most valuable clue to the diagnosis of horseshoe
kidney is the presence of calyces in the region of lower pole point medially & lie medial to the ureter.
CT seldom necessary for the diagnosis.
Complications.
-Obstruction,-hydronephrosis,
-stone
-infection
-tumour
Treatment.
No treatment is necessary unless obstruction or
infection is present.
Drainage may be improved by division of isthmus
If one pole is badly damaged it may require surgical resection
Ectopic kidney
Congenital ectopic kidney usually cause no symptomsunless complications such as
uerteral obstruction or infection develop.
Simple ectopy
Refer to low kidney on the proper side that fail to ascend normally.
It may lie over the pelvic brim or in the pelvis.
rarely it may find in the chest.