Bone imaging
lecture (2)
5
TH
stage
By
Dr. Firas Abdullah
Thiqar college of medicine
Aims of our lecture:
To know the different radiological techniques used in
bone imaging, and what are their advantages and
disadvantages.
To know different bone pathologies.
To differentiate benign from malignant nature of a bony
lesion.
See some examples of bony lesions
Primary
Malignant Bony tumor
❖
Metastatic malignant tumors are by far the
commonest bone neoplasm
❖
Radionuclide bone scans show substantially increased
activity in the lesion.
❖
MRI is the most accurate technique for showing the
extension into both the medullary cavity and the soft
tissues can be accurately defined, as can the
relationship to important nerves and blood vessels.
MRI provides this information better than CT
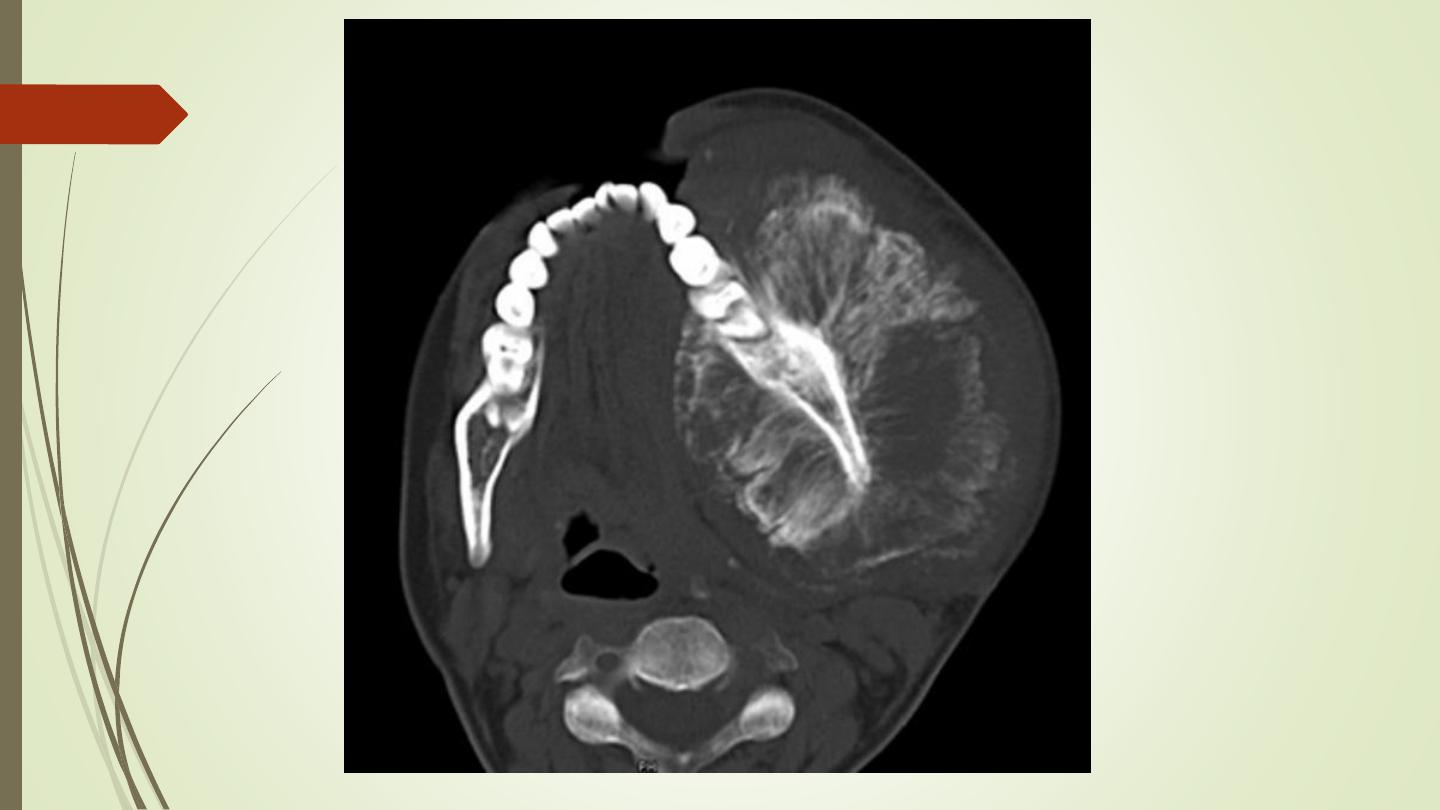
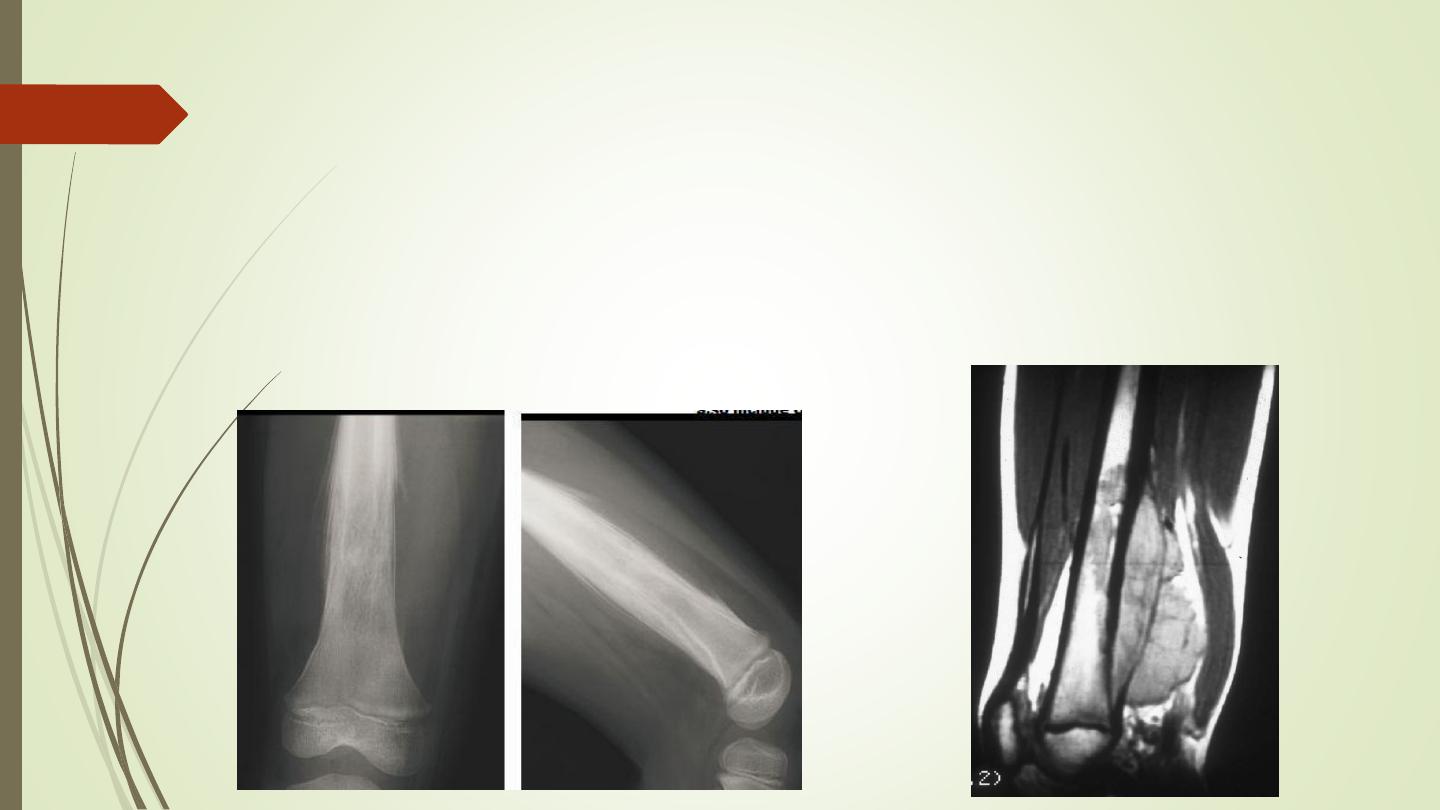
Osteosarcoma (osteogenic sarcoma)
❖
Occurs mainly in the
5–20-year
-old age group, but is
also seen in the elderly following malignant change in
Paget’s disease.
❖
The tumour often arises in a
metaphysis
, most
commonly around the
knee
.
❖
Florid spiculated periosteal reaction is present, the so-
called
sunray appearance
❖
The tumour may elevate the periosteum to form a
Codman’s triangle

Osteosarcoma (osteogenic sarcoma)
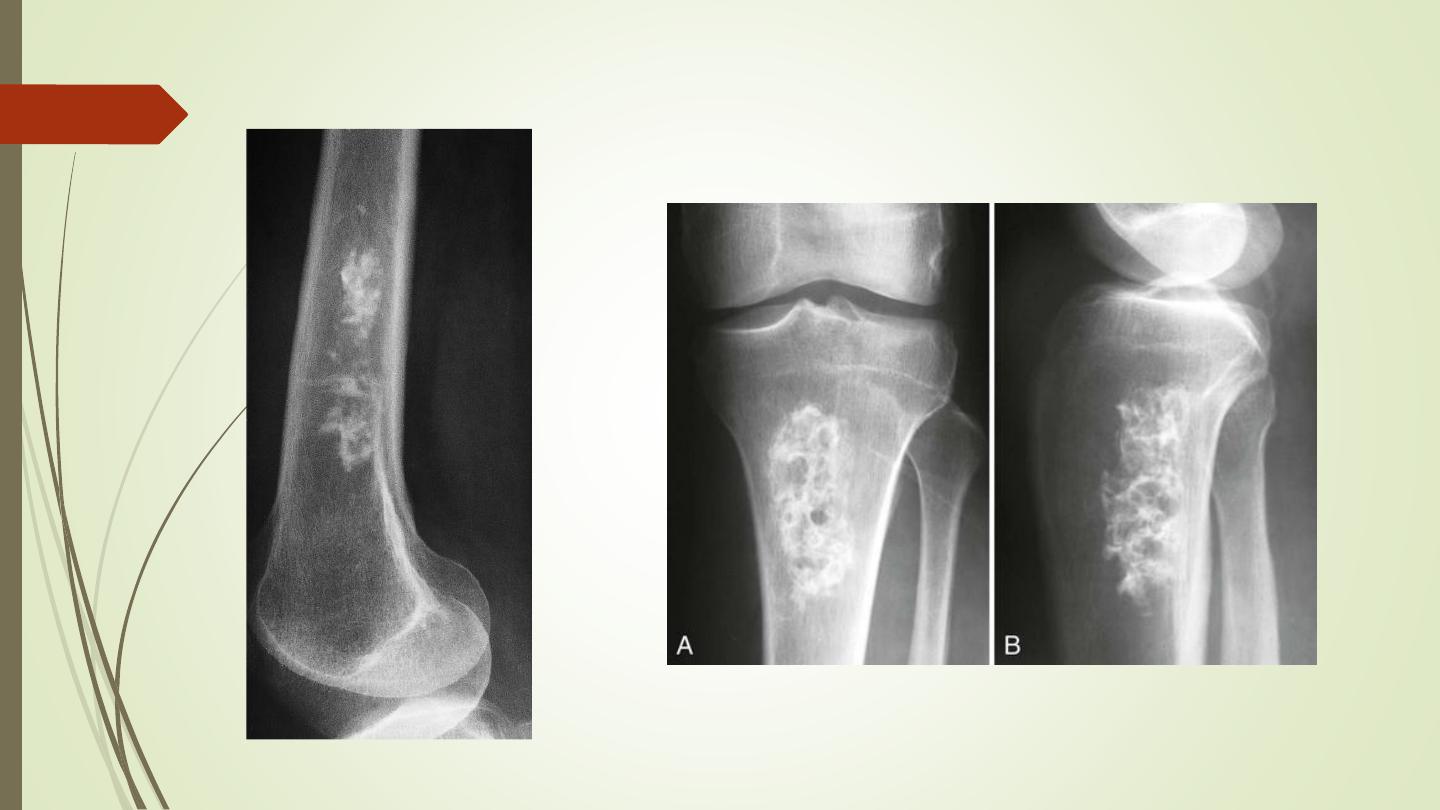
Chondrosarcoma
❖
30–50-year-
old age group
❖
Most commonly in the pelvic bones, scapulae, humeri and
femora.
❖
A chondrosarcoma produces a lytic expanding lesion
containing flecks of calcium.
❖
It can be difficult to distinguish from enchondroma, but it is
usually less well defined and may show a periosteal reaction.
❖
A chondrosarcoma may arise from malignant degeneration of a
benign cartilaginous tumour
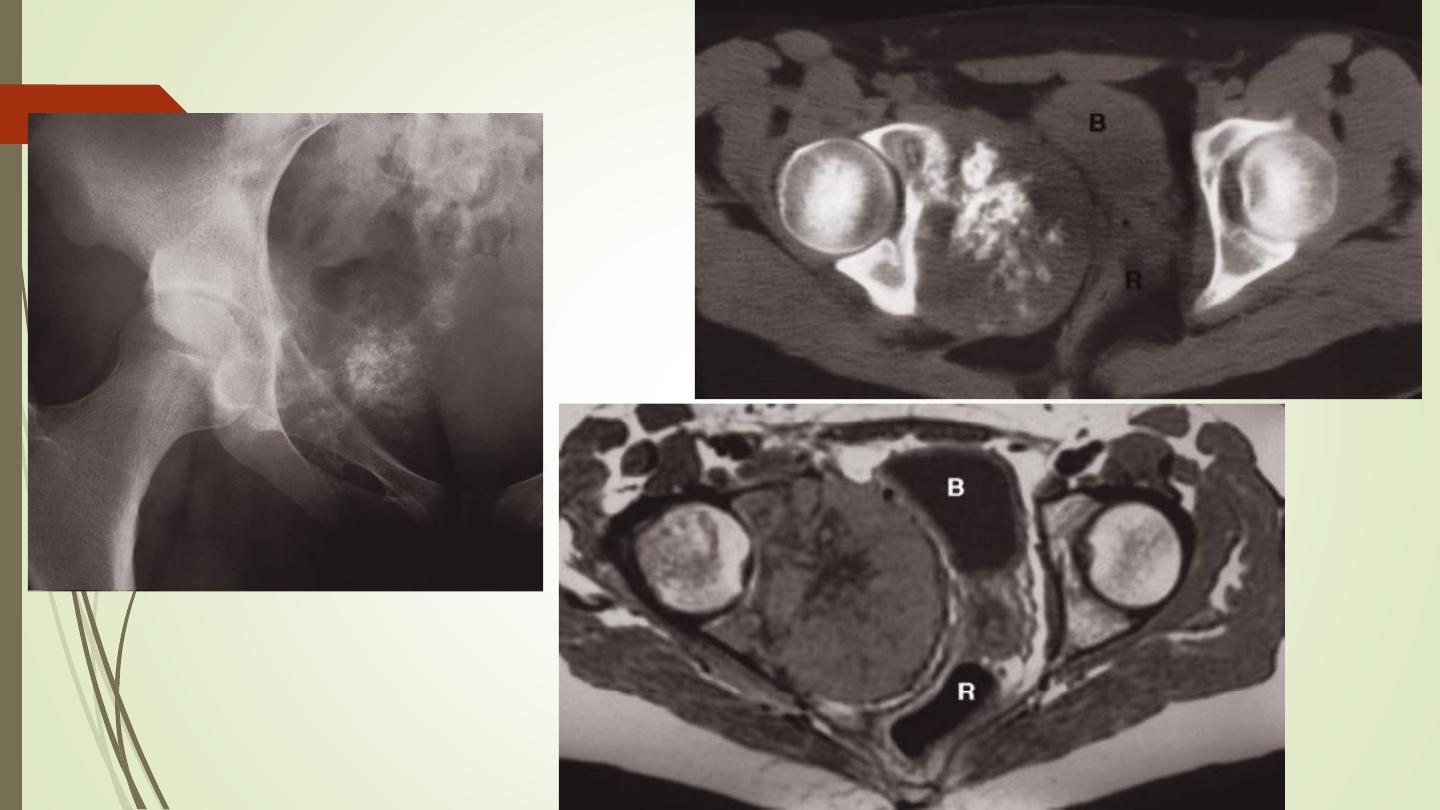
Chondrosarcoma
Ewing’s sarcoma
A highly malignant tumour, commonest in children
Arising in the shaft of long bones.
It produces ill-defined bone destruction with periosteal reaction
that is typically
‘onion skin’
in type
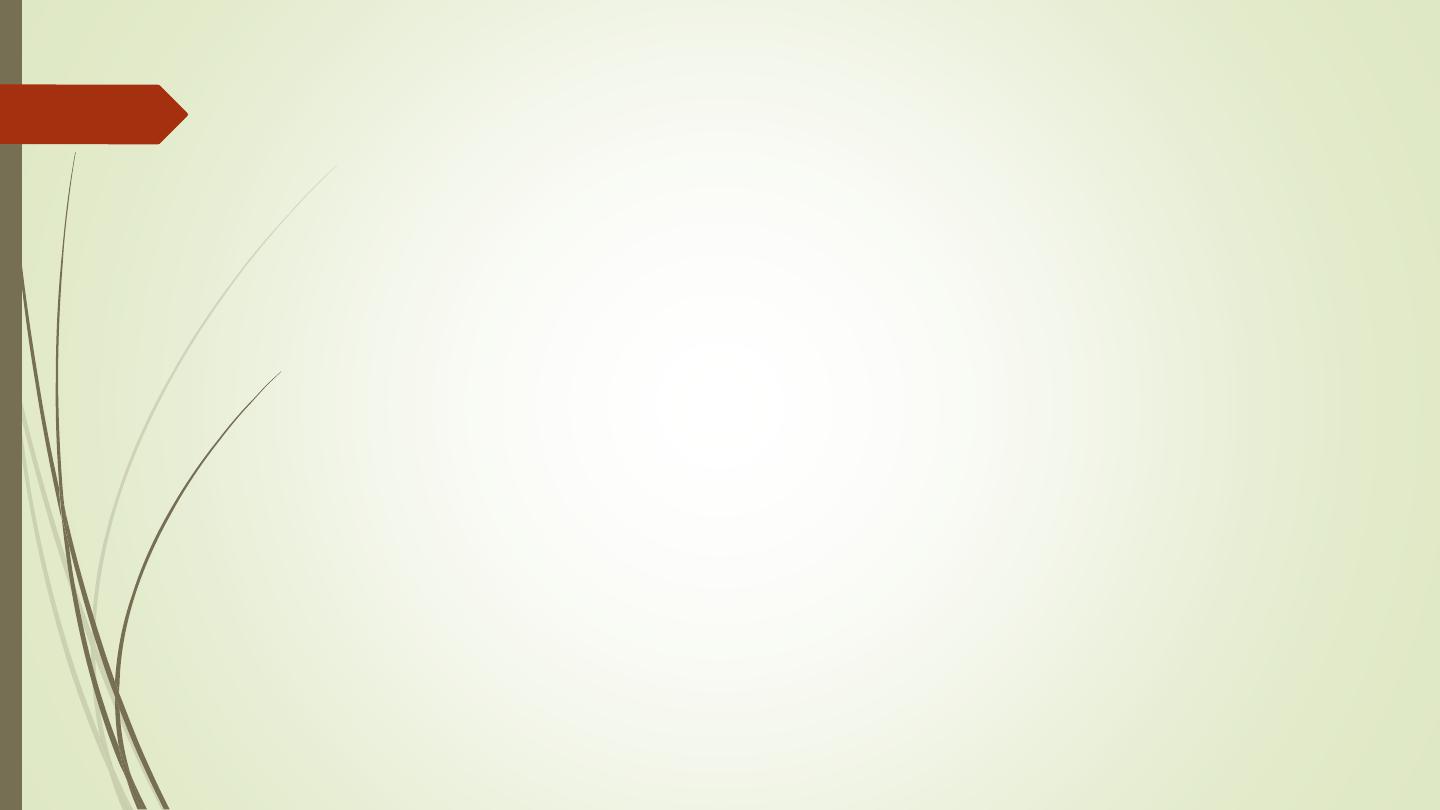
Giant cell tumour
❖
Has features of both malignant and benign tumours.
❖
It is locally invasive but rarely metastasizes.
❖
It occurs most commonly around the knee and at the
wrist after the epiphyses have fused. It is an expanding
destructive lesion, which is
subarticular in position

Giant cell tumour
Primary lymphoma
❖
Bone involvement is
rare
❖
Most osseous malignant lymphoma is associated with
generalized lymph node disease.
❖
When solitary primary lymphomas are encountered they may
produce
sclerotic or lytic
bone lesions
❖
Indistinguishable on imaging grounds from other malignant
tumor
Primary lymphoma
Benign tumours and tumour-like conditions
❖
In general, benign lesions have an edge which is well
demarcated from the normal bone by a sclerotic rim.
❖
They cause expansion but rarely breach the cortex.
❖
There is no soft tissue mass and a periosteal reaction is
unusual unless there has been a fracture through the
lesion.
❖
Radionuclide scans in benign tumours usually show little or
no increase in activity, provided no fracture has
occurred.
Enchondromas:
❖
Are seen as lytic expanding lesions most commonly in the
bones of the hand.
❖
They often contain a few flecks of calcium and frequently
present as a pathological fracture.
Fibrous cortical defects (non-ossifying fibromas):
❖
Are common chance findings in children and young
adults.
❖
They produce well-defined lucent areas in the cortex of
long Bones
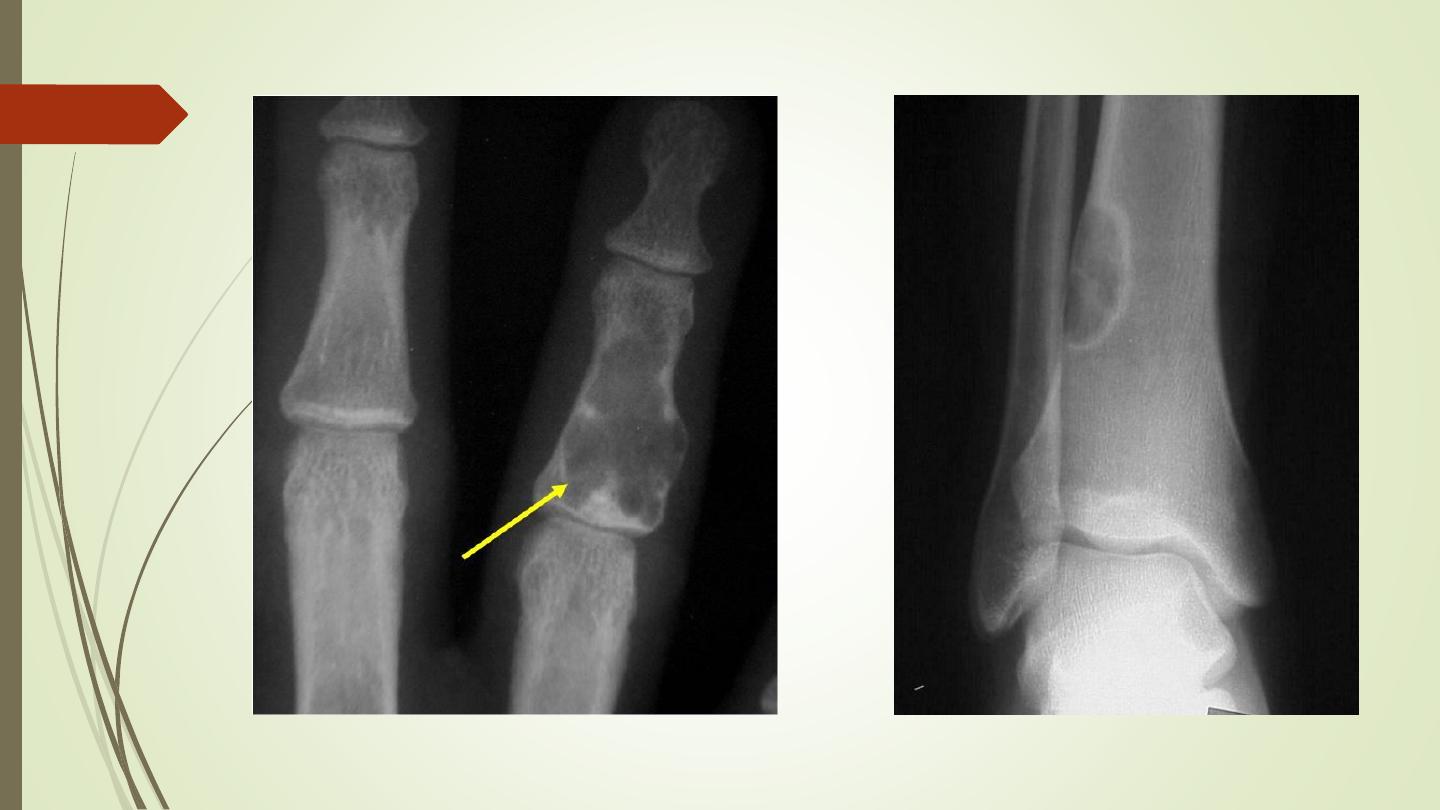
Enchondroma
Fibrous cortical defects
Fibrous dysplasia
❖
May affect one or several bones.
❖
Affects the long bones and ribs as a well defined lytic lesion
and may expand the bone.
❖
There may be a sclerotic rim around the lesion.
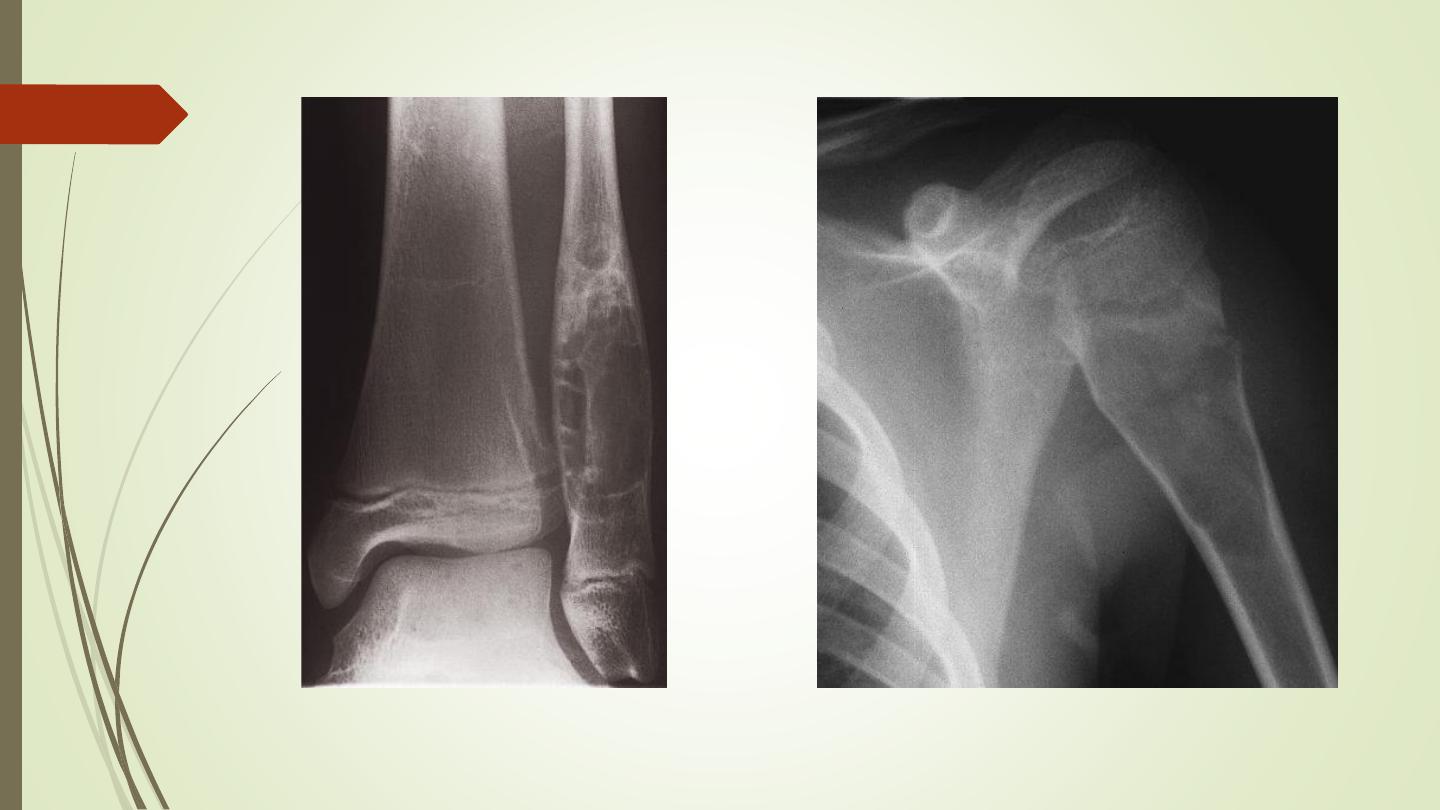
Simple bone cyst
❖
Has a wall of fibrous tissue and is filled with fluid.
❖
It occurs in children and young adults, most commonly in
the humerus and femur.
❖
The cortex may be thin and the bone expanded.
❖
Pathological fracture.
Fibrous dysplasia
Simple bone cyst

Aneurysmal bone cysts
❖
Mostly they are seen in children and young adults
❖
Affects the spine, long bones or pelvis.
❖
These lesions are
purely lytic and cause massive expansion of
the cortex
, hence the name ‘
aneurysmal
’. They may grow
quickly and appear very aggressive but are, nevertheless,
benign lesions.
❖
Computed tomography and MRI may show the
blood-fluid
level within the cyst.
❖
The major differential diagnosis is from giant-cell tumour.
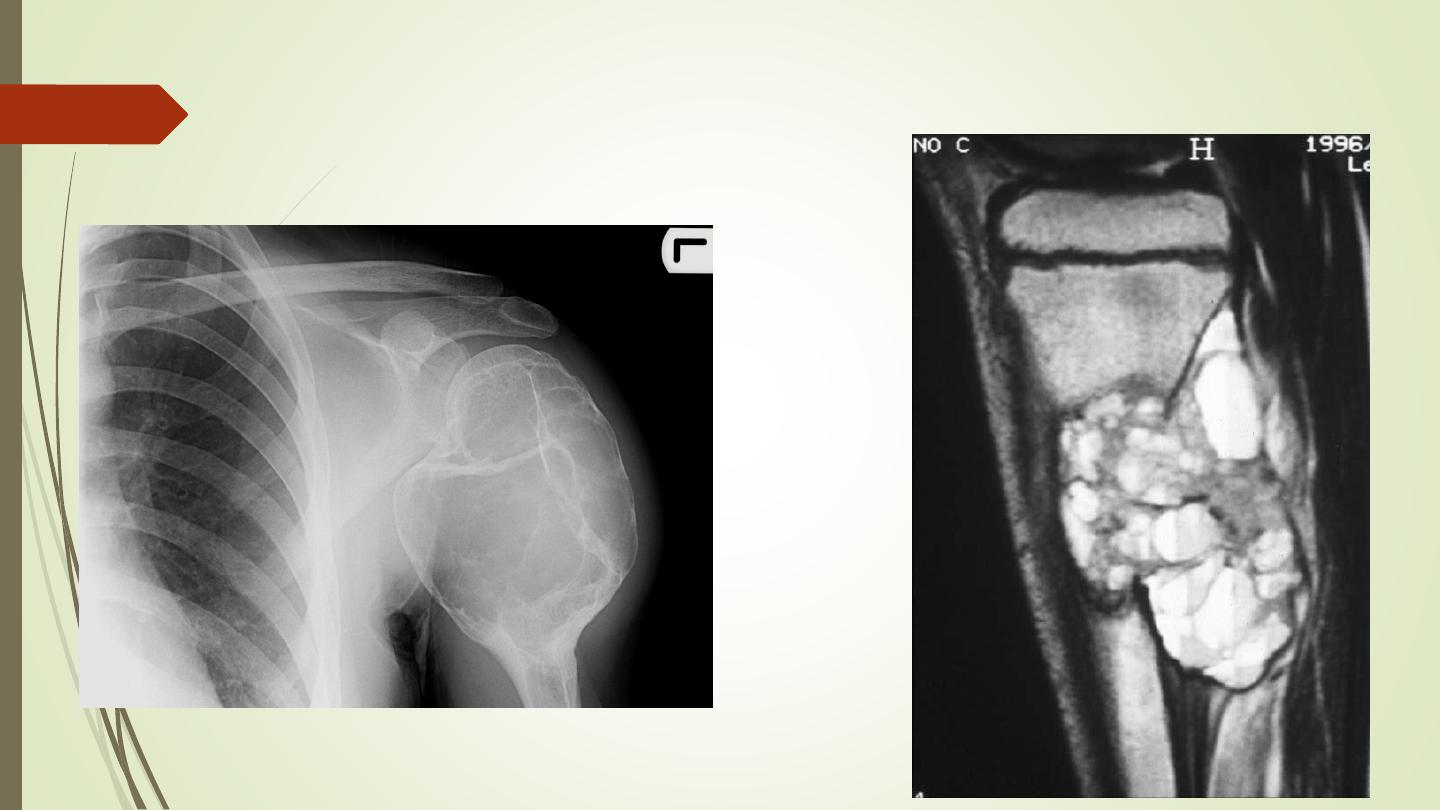
Aneurysmal bone cysts
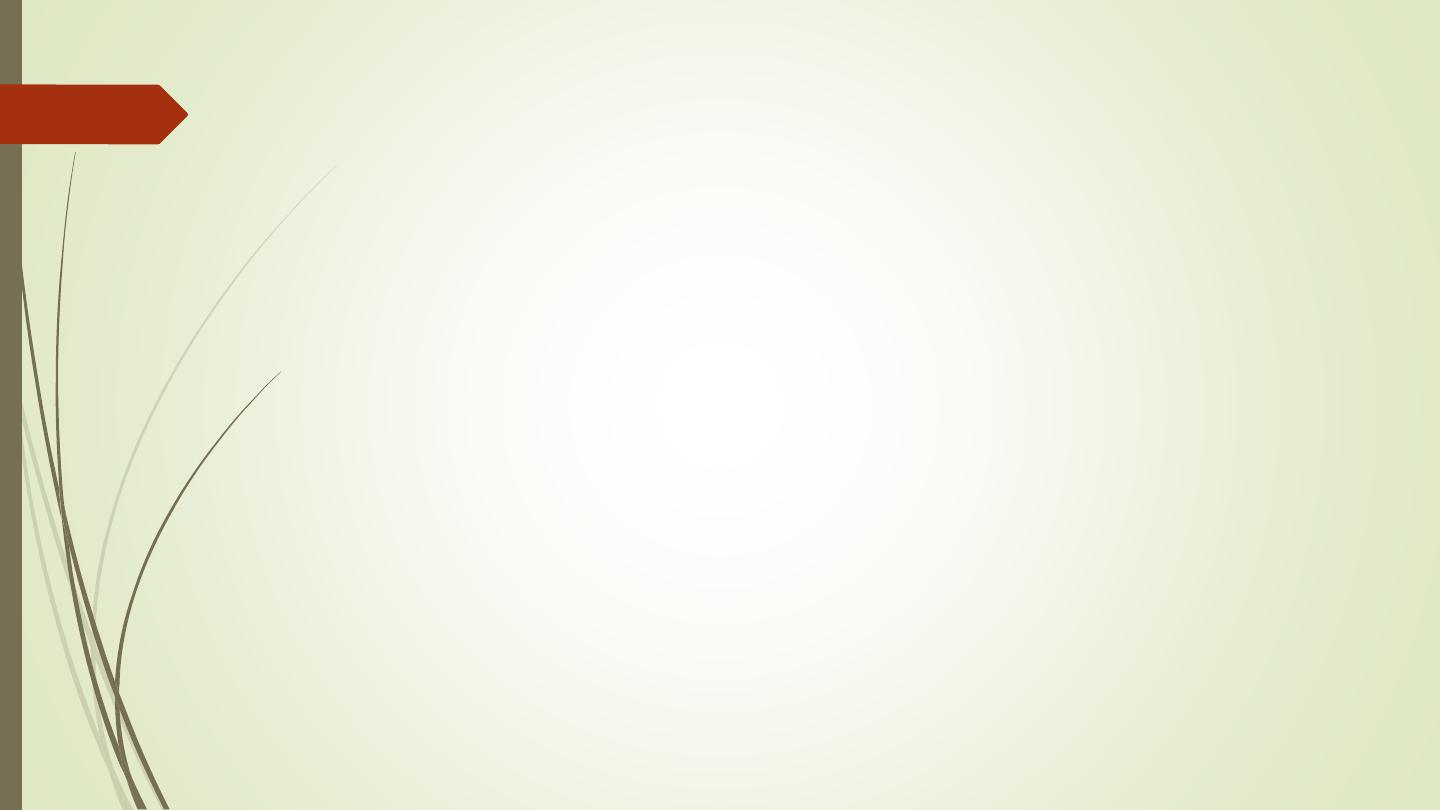
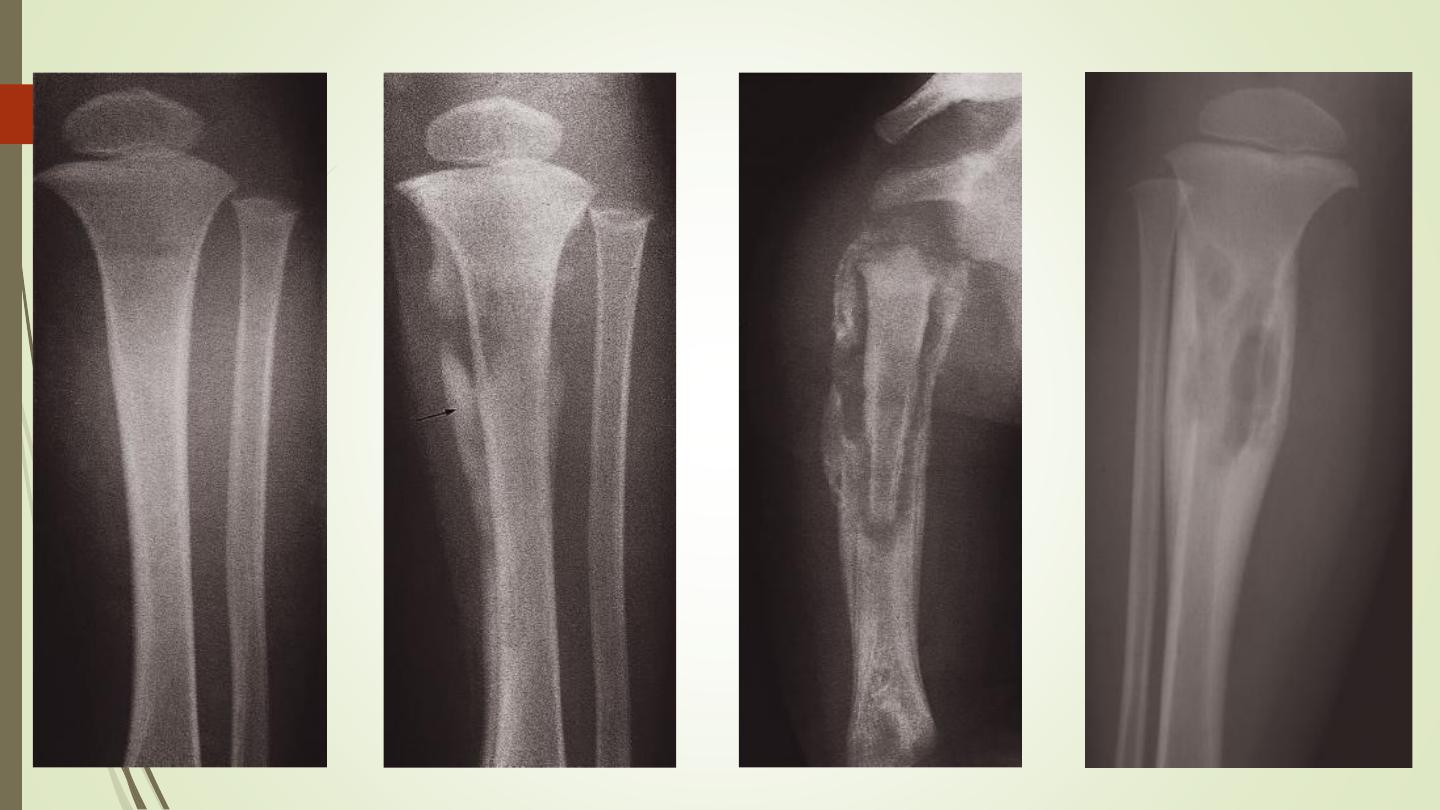
Osteoid osteoma
❖
Is a painful condition found most commonly in the femur and
tibia in young adults.
❖
Characteristic radiological appearance: a small lucency,
sometimes with central specks of calcification, known as a
nidus
, surrounded by
dense sclerotic rim.
❖
A periosteal reaction may also be present.
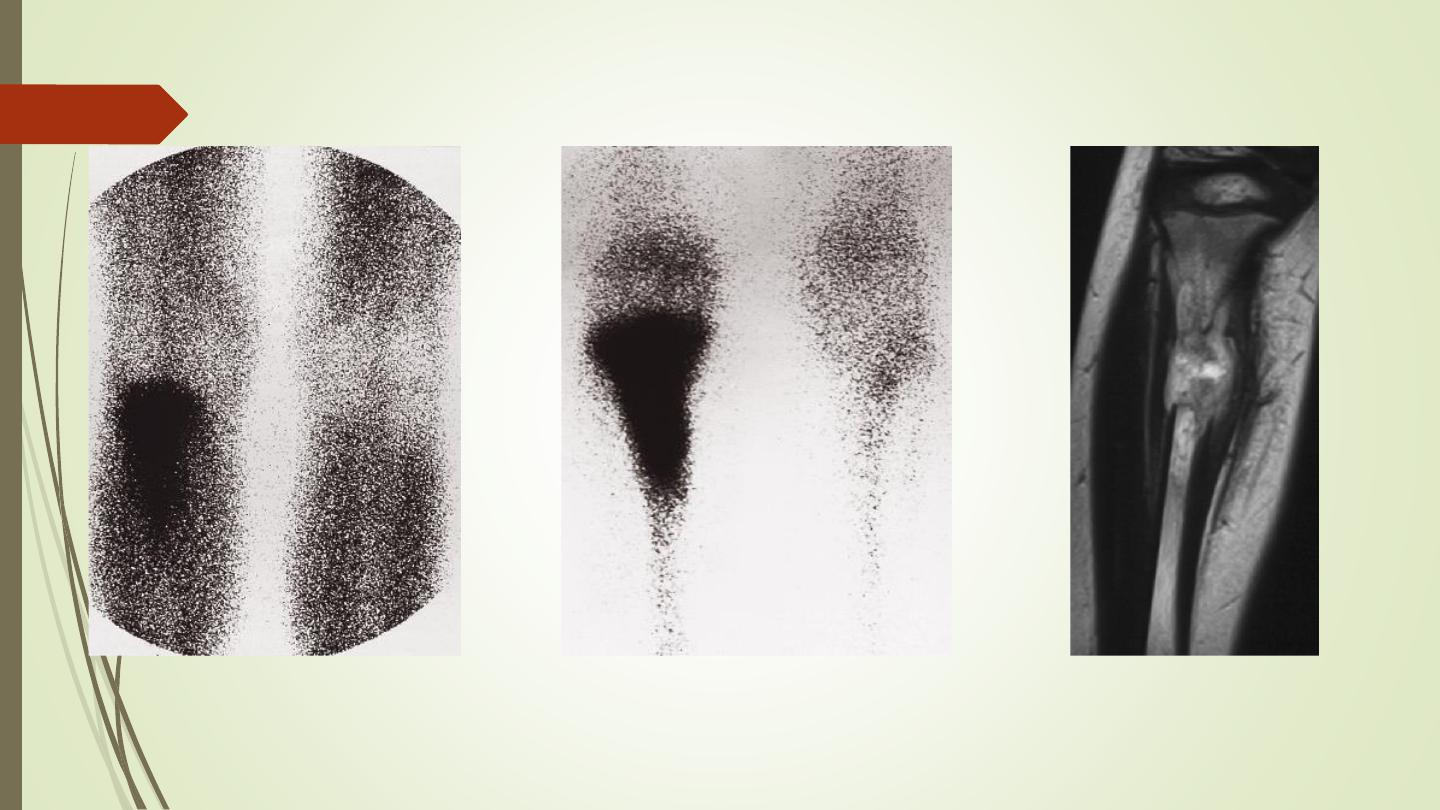
❖
Radionuclide bone scanning: shows marked focal increased
activity.
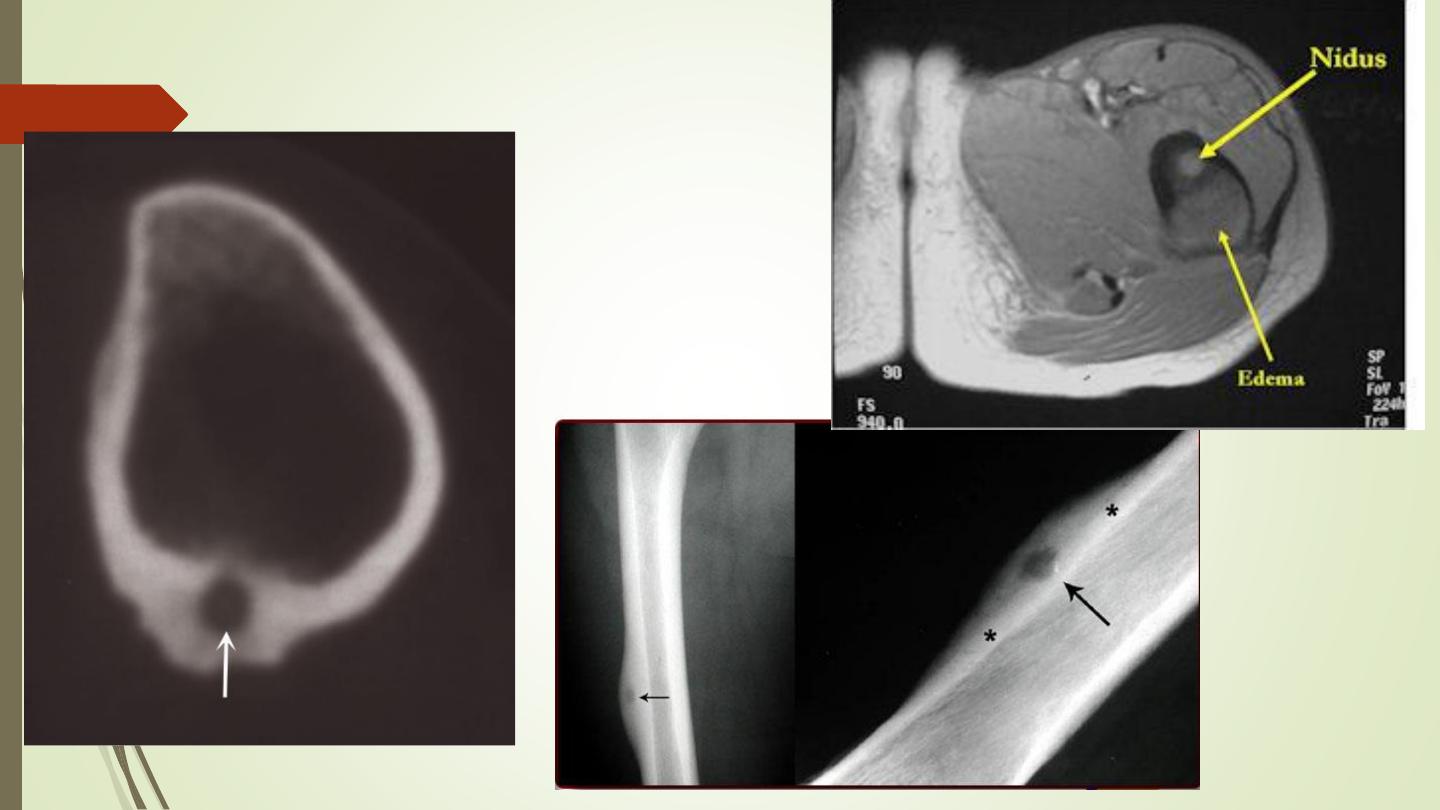
Osteoid osteoma
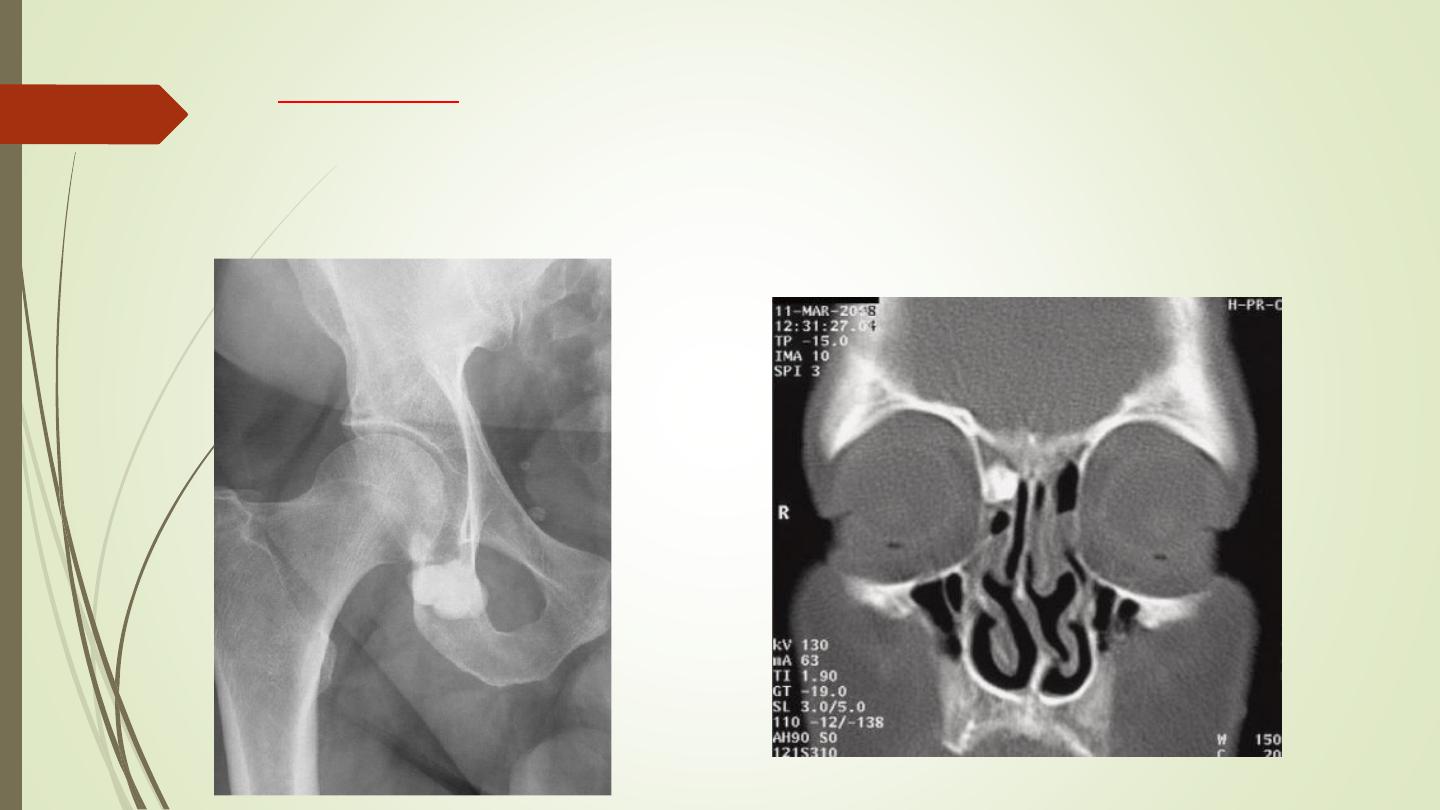
osteoma
An is a benign tumour consisting of dense bone. They
may occur in the paranasal sinuses.
Eosinophil granuloma
Is the mildest and most frequent form of Langerhans
histiocytosis.
It occurs in children and young adults
Lytic lesions which may be single or multiple, most frequently in
the skull, pelvis, femur and ribs.
May have the features of an aggressive lesion, or well defined
and may have a sclerotic rim.
A periosteal reaction is sometimes seen.
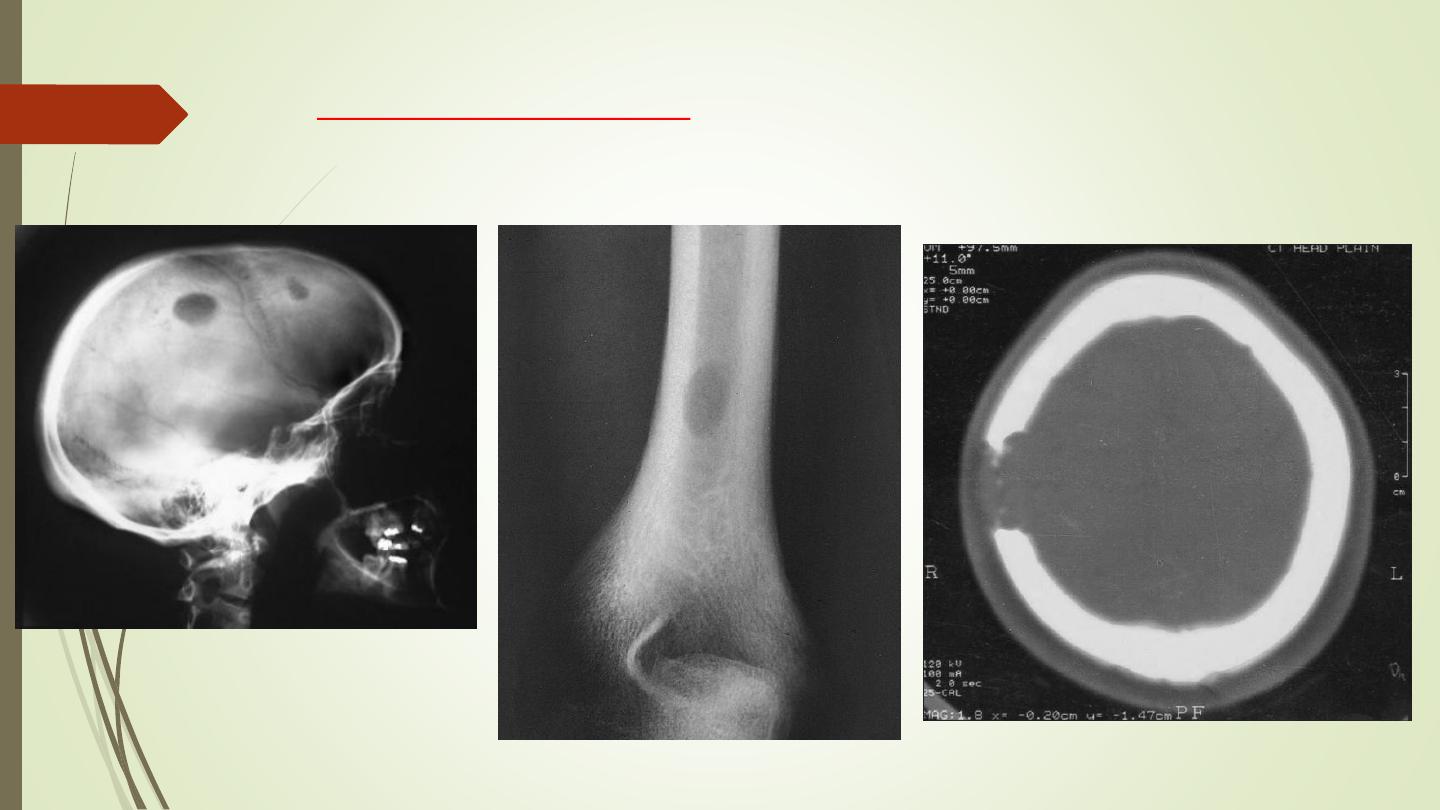
Eosinophil granuloma
Osteomyelitis
Most often caused by
Staphylococcus aureus
and usually affects infants
and children.
The
initial radiographs
are normal as bone changes are not visible until
10–14 days
after the onset of the infection, but the 99mTc radionuclide
bone scan and MRI show changes much earlier in the course of the
disease within a day or two.
Typically, acute osteomyelitis affects the metaphysis of a long bone,
usually the femur or tibia.
The earliest signs on plain radiographs are soft tissue swelling and bone
destruction in the metaphysis, with a periosteal reaction that eventually
may become very extensive and surround the bone to form an
involucrum
.
A part of the original bone may die and form a separate dense
fragment known as a
sequestrum
.
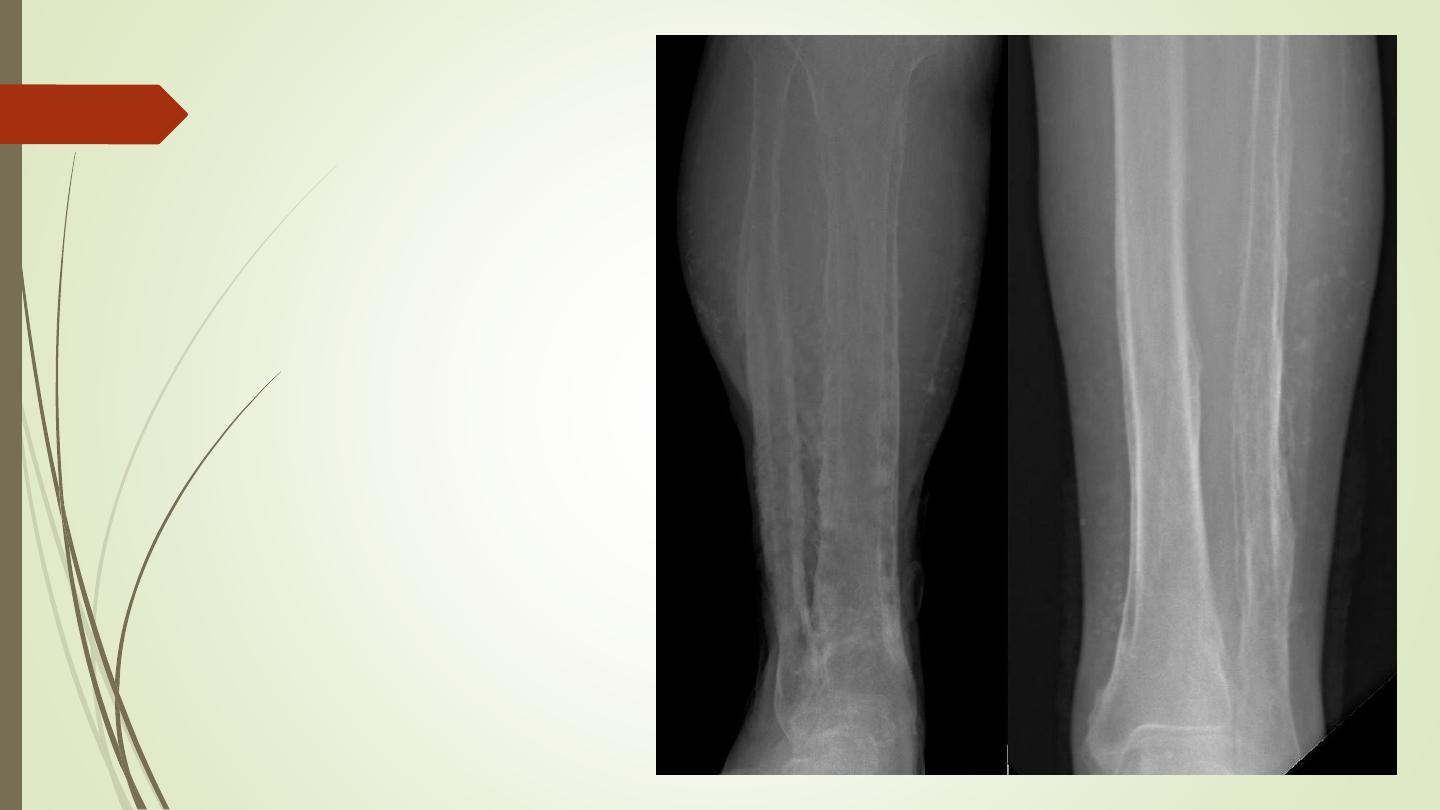
Osteomyelitis
In
chronic osteomyelitis
, the bone becomes thickened and sclerotic with
loss of differentiation between the cortex and the medulla. And may
produce well defined lytic lesion within the bone known as a
Brodie’s
abscess
Tuberculous osteomyelitis
is a particular problem in African and Asian
populations and patients with AIDS.
The spine is the most frequent site of infection, followed by the large
joints, but any bone may be affected. The disease is relatively indolent
and produces large areas of bone destruction which, unlike pyogenic
osteomyelitis, may be relatively asymptomatic in the early stages.
Bone infarction
Causes
: caisson disease, sickle cell disease or following
radiation therapy or seen in elderly people without known
cause
Once healed, they appear as irregular calcification in the
medulla of a long bone
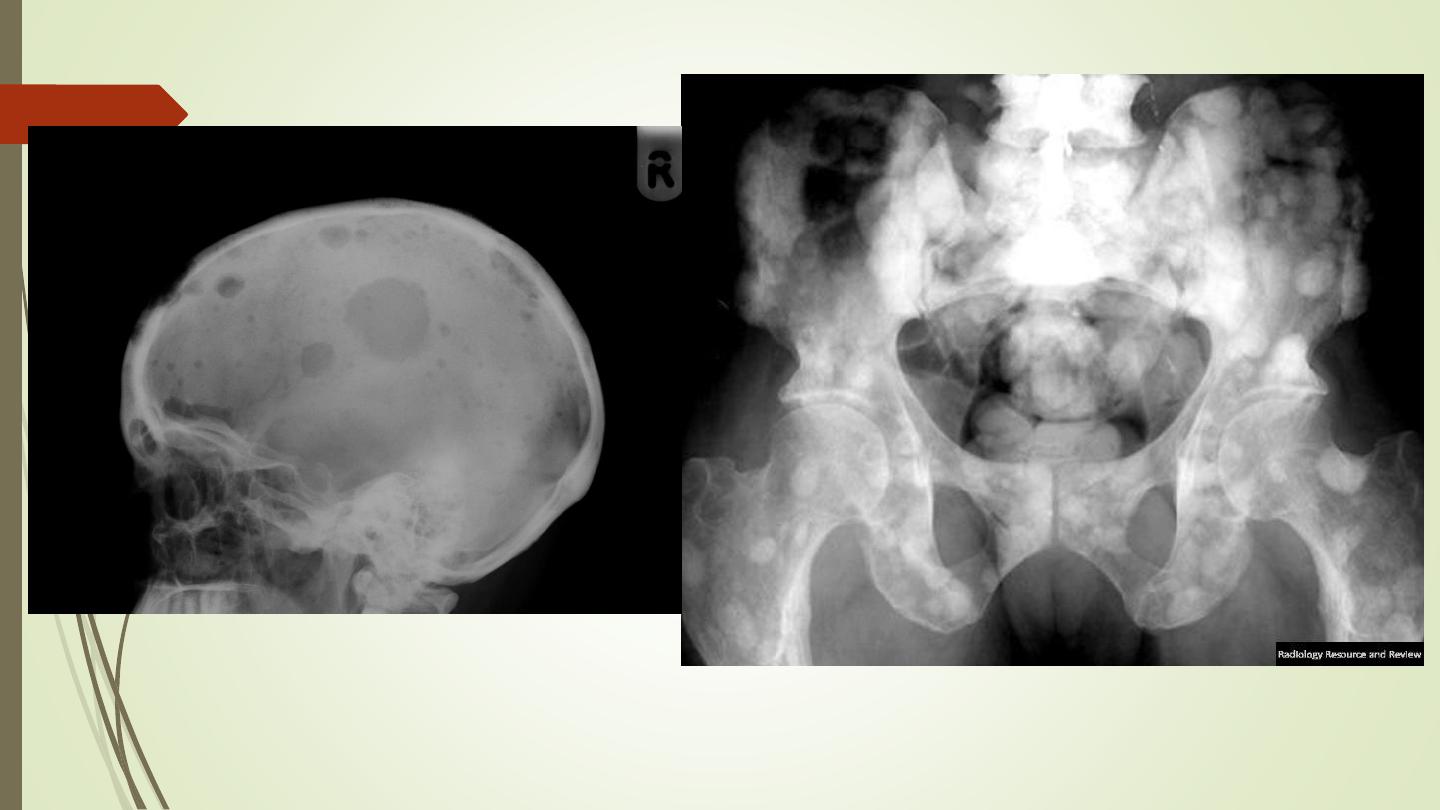
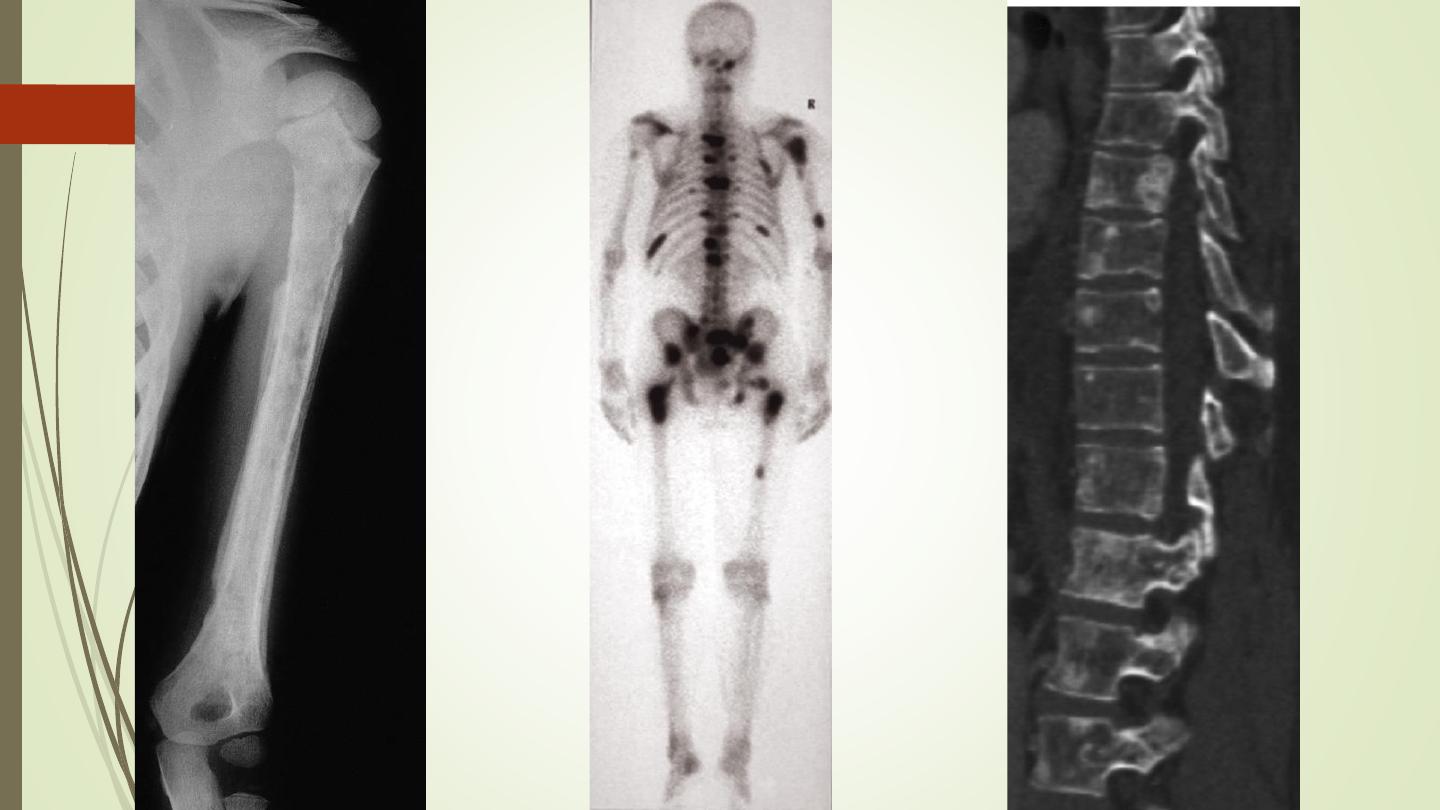
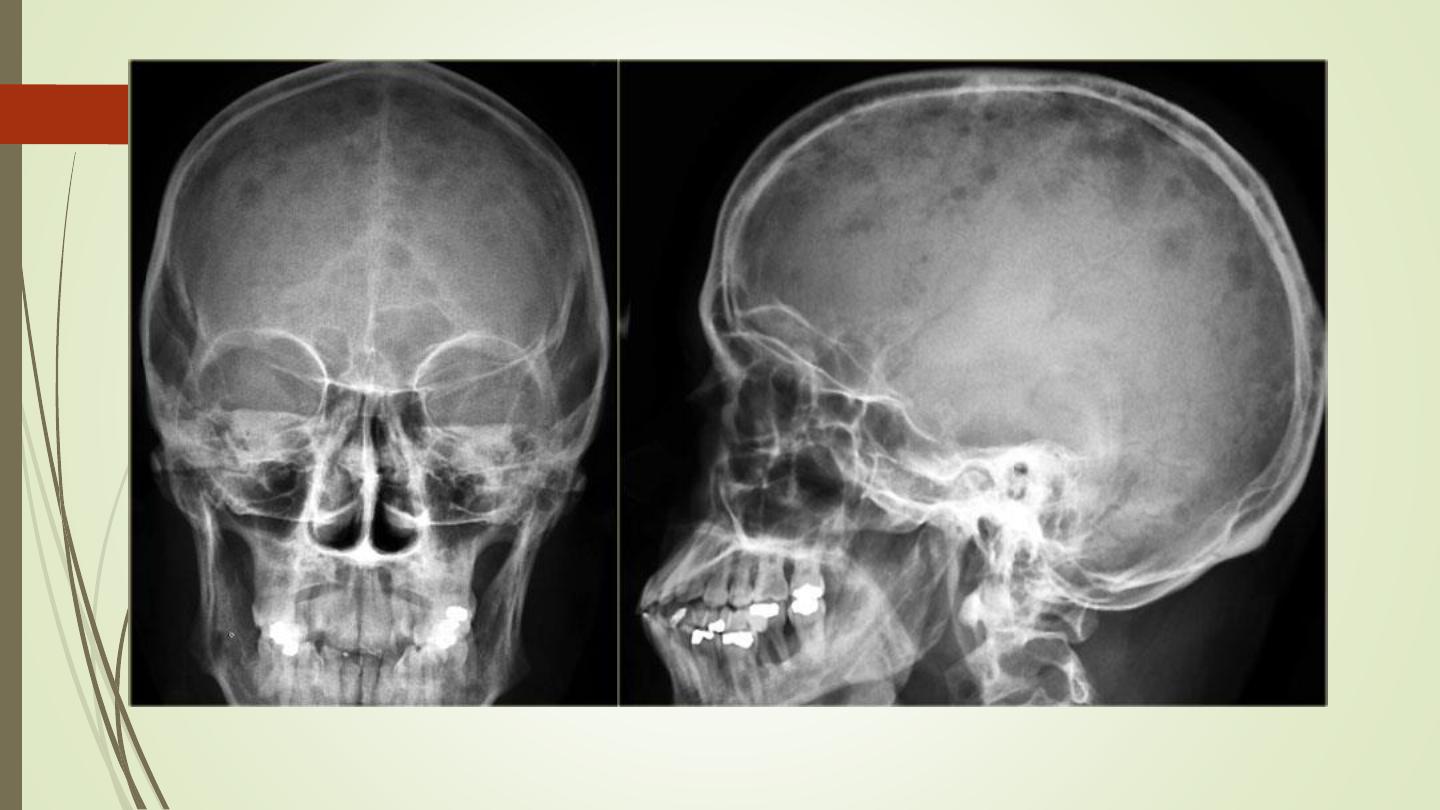
Multiple focal lesions
1.
Metastases:
Commonest malignant bone tumour
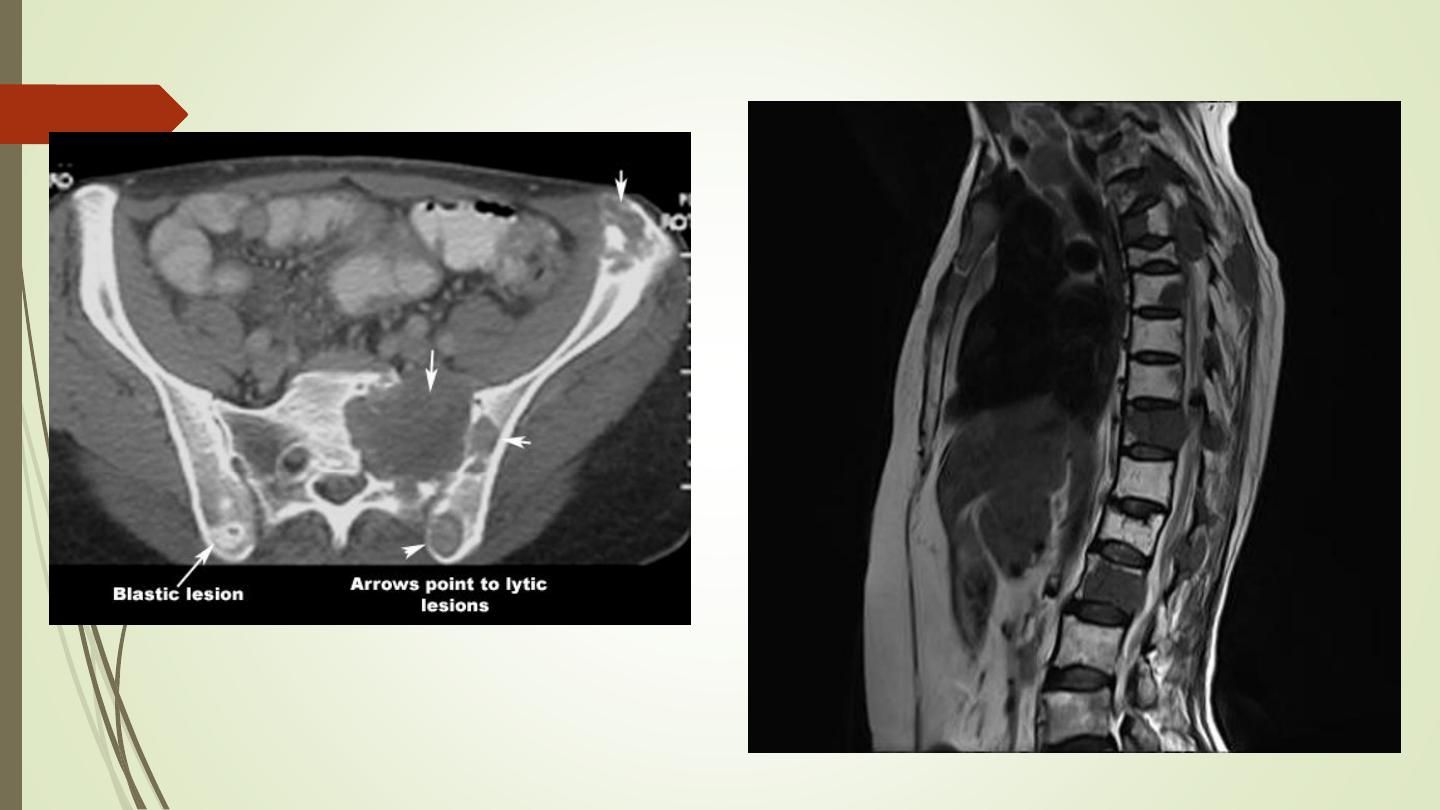
Metastases may be sclerotic, lytic or a mixed.
Bones mostly affected are those containing red marrow:
the spine, skull, ribs, pelvis, humeri and femora.
Most of metastases are lytic
Metastases and myeloma are virtually the only causes of
multiple obvious lytic lesions in bone.
Sclerotic metastases: mainly from prostate CA in male
and breast CA in female
Mixed lytic – sclerotic metastasis are mainly from breast
CA.
Metastases with bone expansion occur in primary
tumours of the kidney and thyroid.
Neuroblastoma metastasis may cause periosteal
reaction
Radionuclide bone scan: best modality, reveals 30% of
lesions that are not evident on X ray.
MRI: better sensitivity than radionuclide.
Disadvantage
?
CT scan: less sensitive than MRI, need bone window
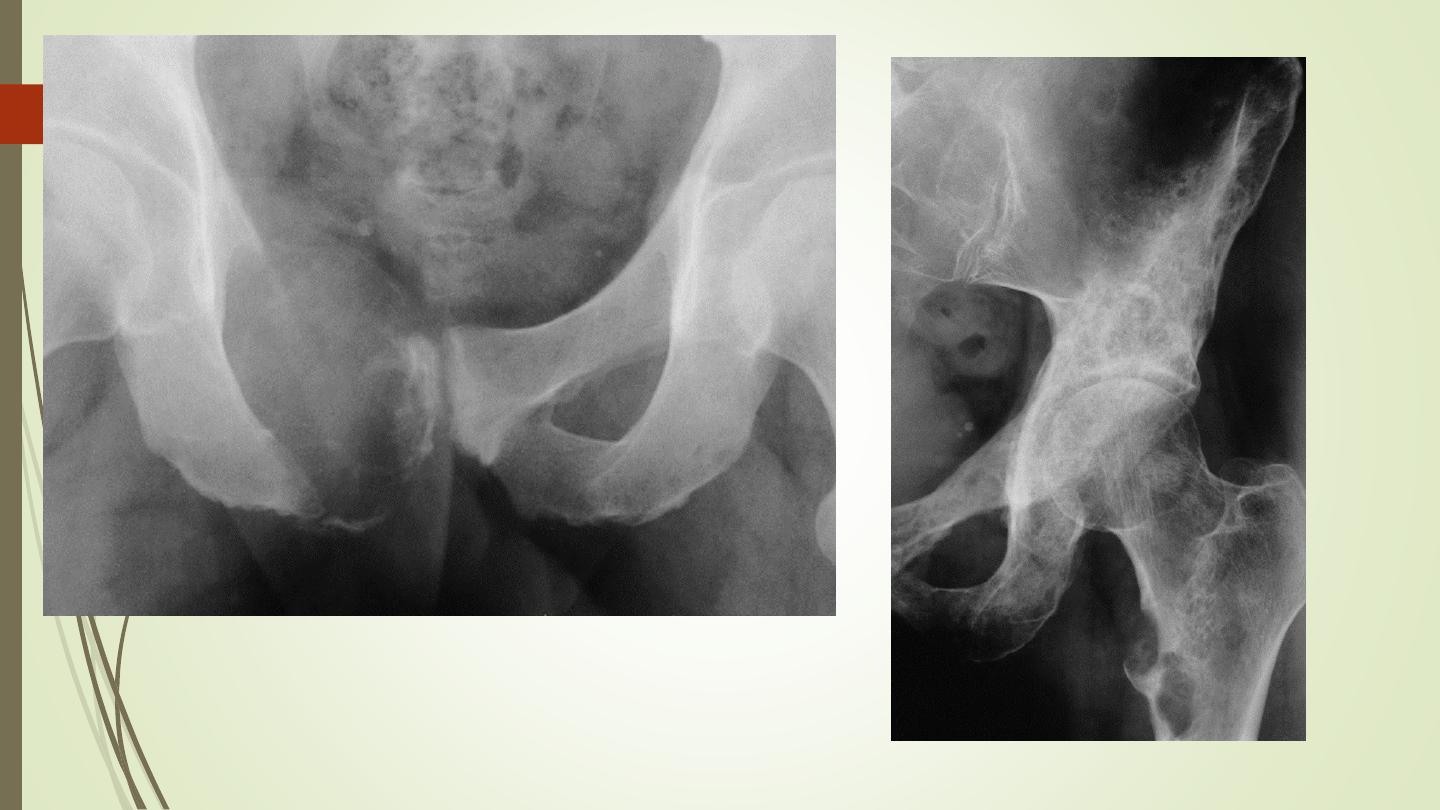
2- Multiple myeloma:
Most frequently seen in bones with active haemopoiesis.
The bone lesions may resemble lytic metastases in every
way, but are often better defined and may cause
expansion of the bone
Diffuse marrow involvement may give rise to generalized
loss of bone density, producing a picture similar to that of
osteoporosis

Multiple periosteal reactions
1)
Non-accidental injury
2)
Widespread bone infection, e.g. congenital syphilis,
neonates with infected intravenous catheters
3)
Venous stasis and ulceration of the legs
4)
Hypertrophic pulmonary osteoarthropathy
5)
Scurvy
chronic venous stasis

Hypertrophic pulmonary
osteoarthropathy
Generalized decrease in bone density
(osteopenia)
osteoporosis
osteomalacia
hyperparathyroidism
multiple myeloma
Osteoporosis
Osteoporosis is the consequence of a deficiency of
protein
Osteoporosis predisposes to fractures
The changes of osteoporosis are best seen in the spine
Causes
:
❖
idiopathic, often subdivided according to age of onset, e.g.
juvenile, postmenopausal, senile.
❖
Cushing’s disease and steroid therapy
❖
disuse.
Disuse osteoporosis
Senile osteoporosis, penciled cortex
Rickets and osteomalacia
Poor mineralization of osteoid
The main causes:
❑
Dietary deficiency of vitamin D, or lack of
exposure to
sunlight.
❑
Malabsorption.
❑
Renal disease.
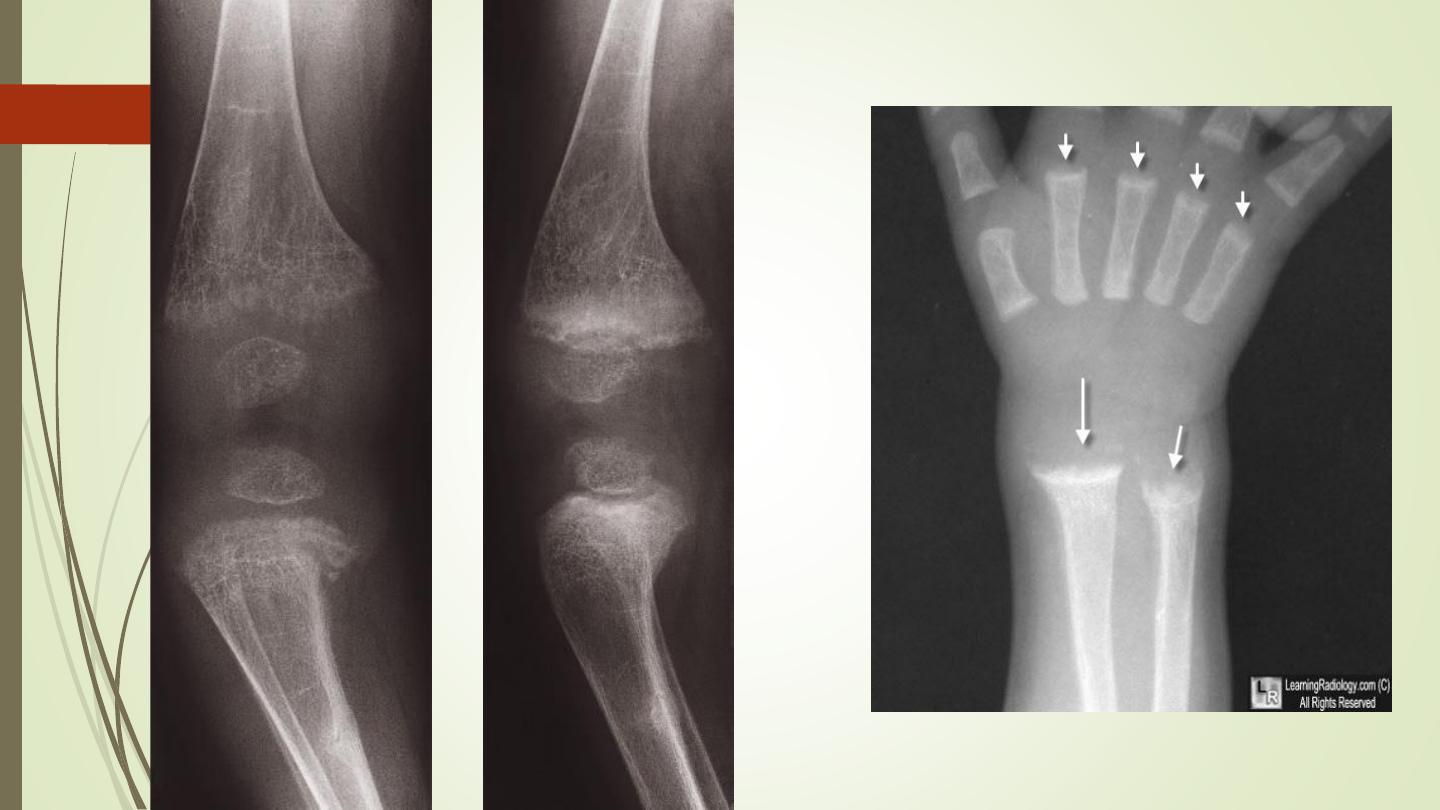
Rickets
The changes are maximal where bone growth is
occurring, so they are best seen at the knees, wrists
and ankles.
The zone of provisional calcification is deficient and
the metaphyses are irregularly mineralized, widened
and cupped
Widened growth plate
Generalized decrease in bone density
Deformities of the bones
Greenstick fractures are common.
Osteomalacia
Loss of bone density
Thinning of trabeculae and cortex
Looser`s zones (pseudofractures): commonest in the
scapulae, medial aspects of the femoral necks and
in the pubic rami.
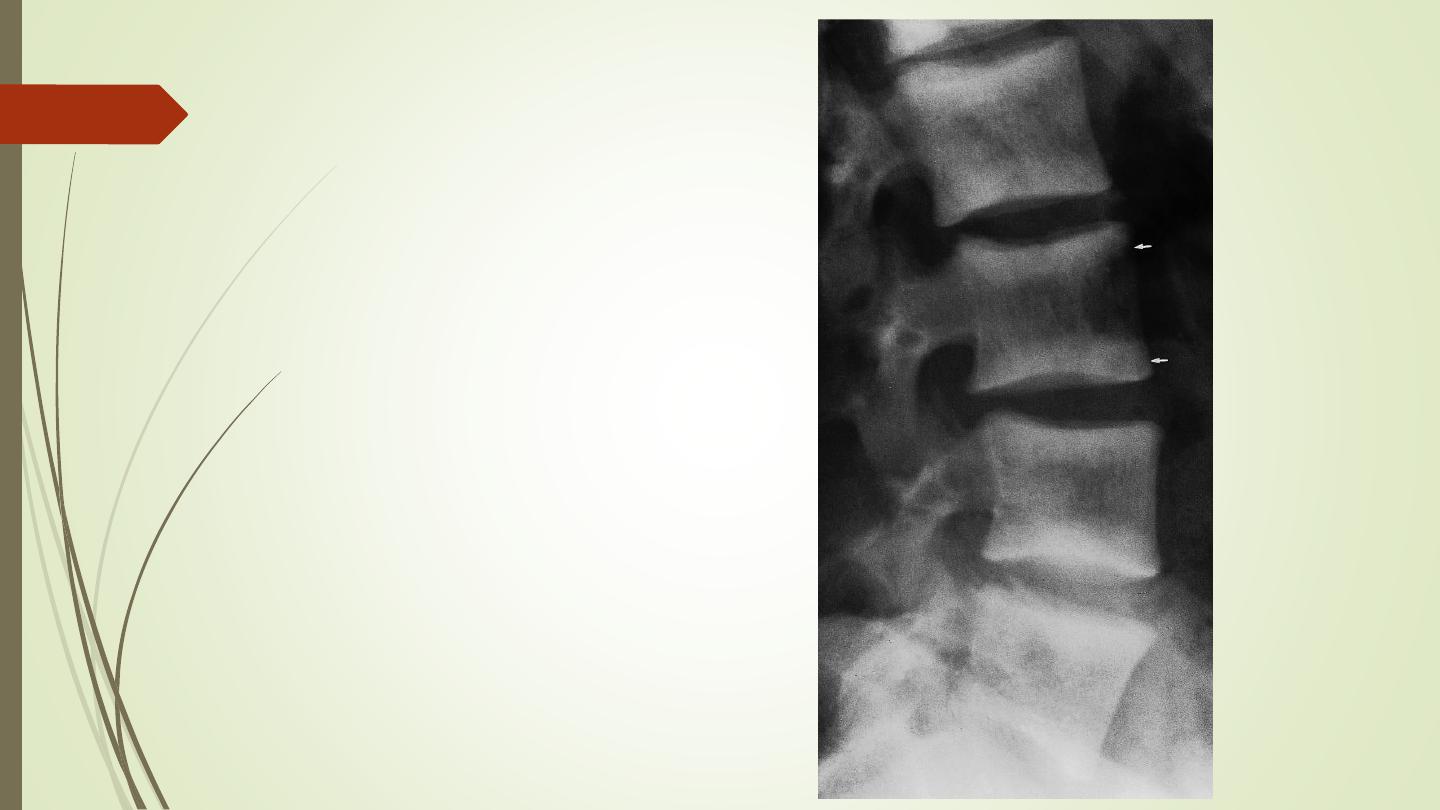
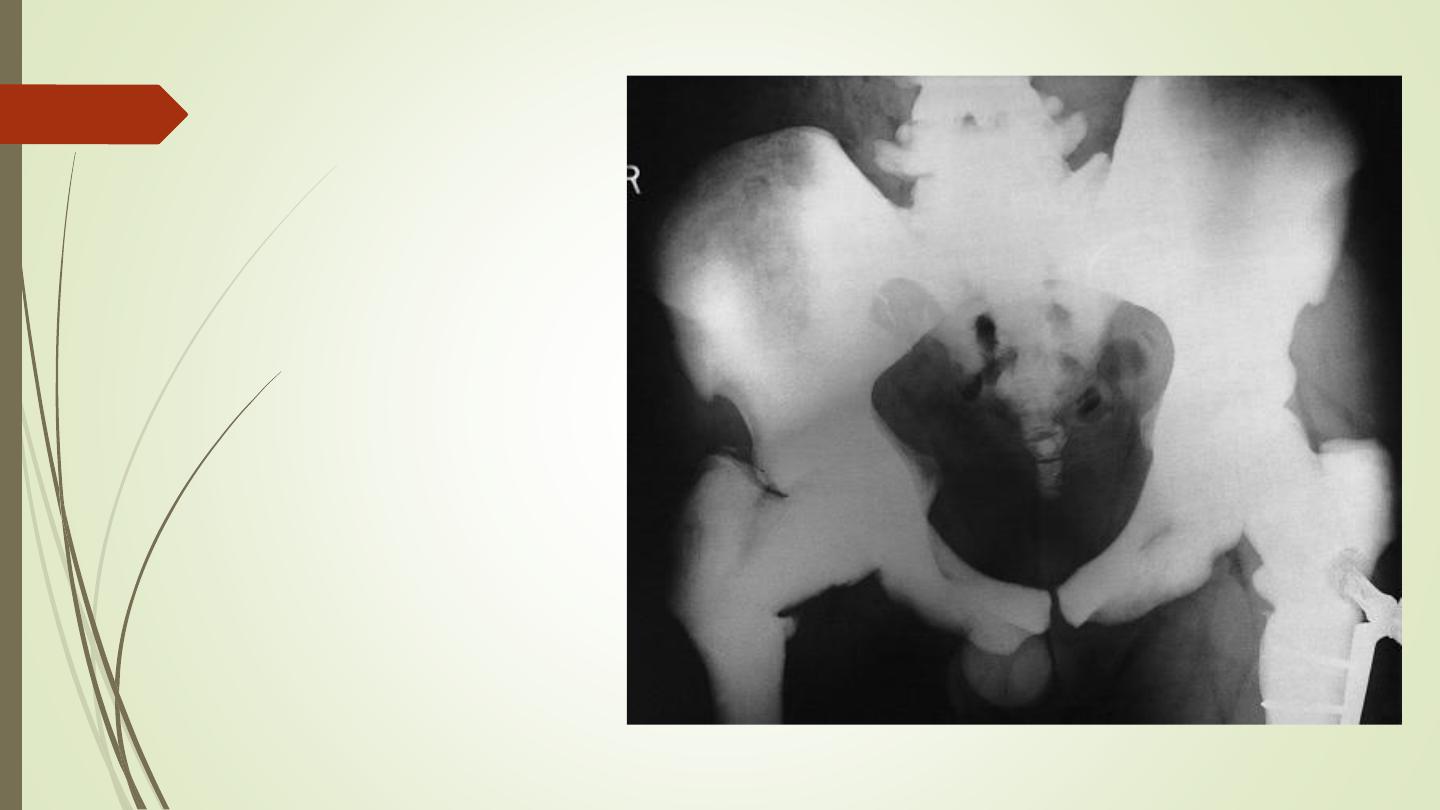
Bone deformity: biconcave vertbebra. Bowing of
long bones. Triradiate pelvis
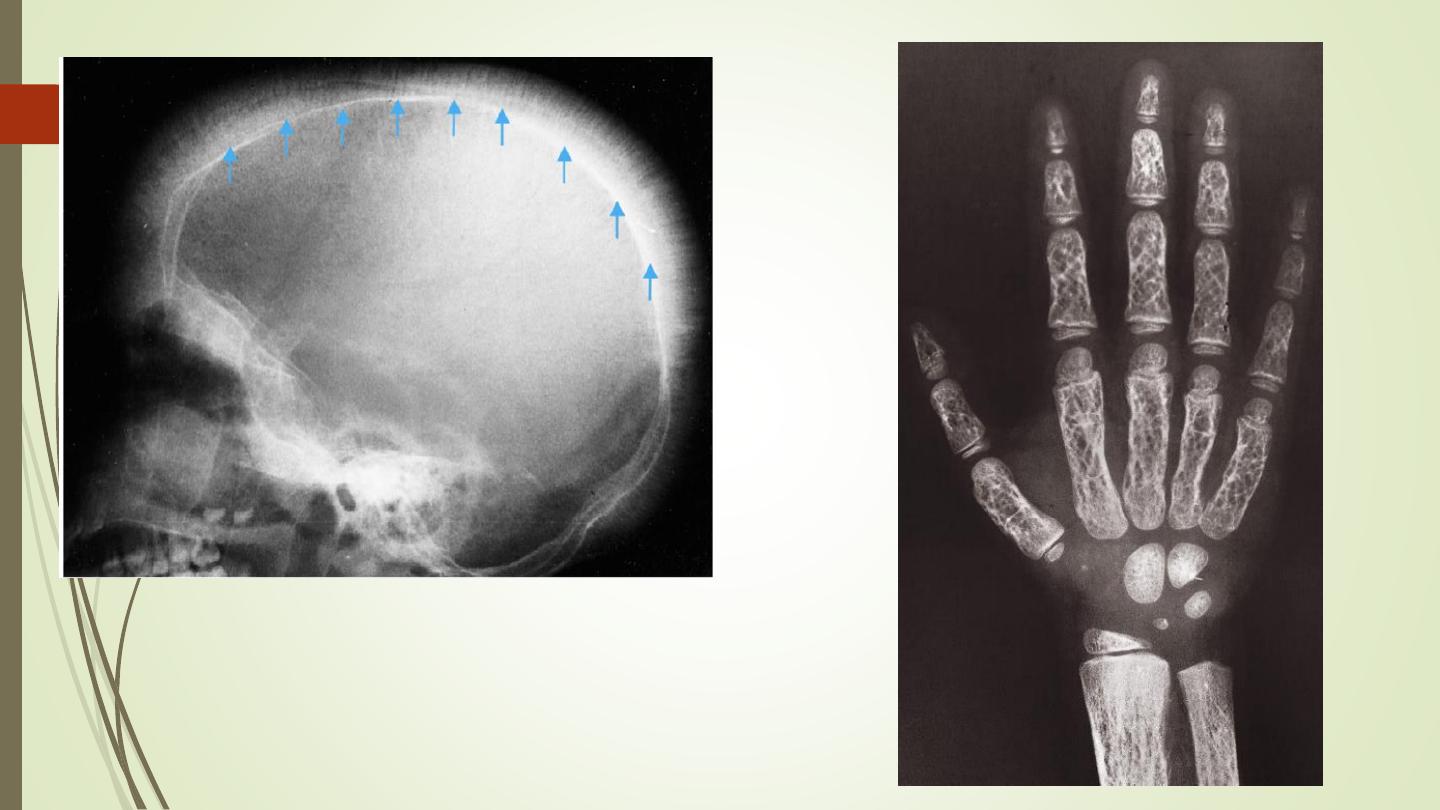
Hyperparathyroidism:
Excess parathyroid hormone secretion mobilizes
calcium from the bones, resulting in a decrease in bone
Primary: hyperplasia or a tumour of the parathyroid
glands
Secondary: chronic renal failure
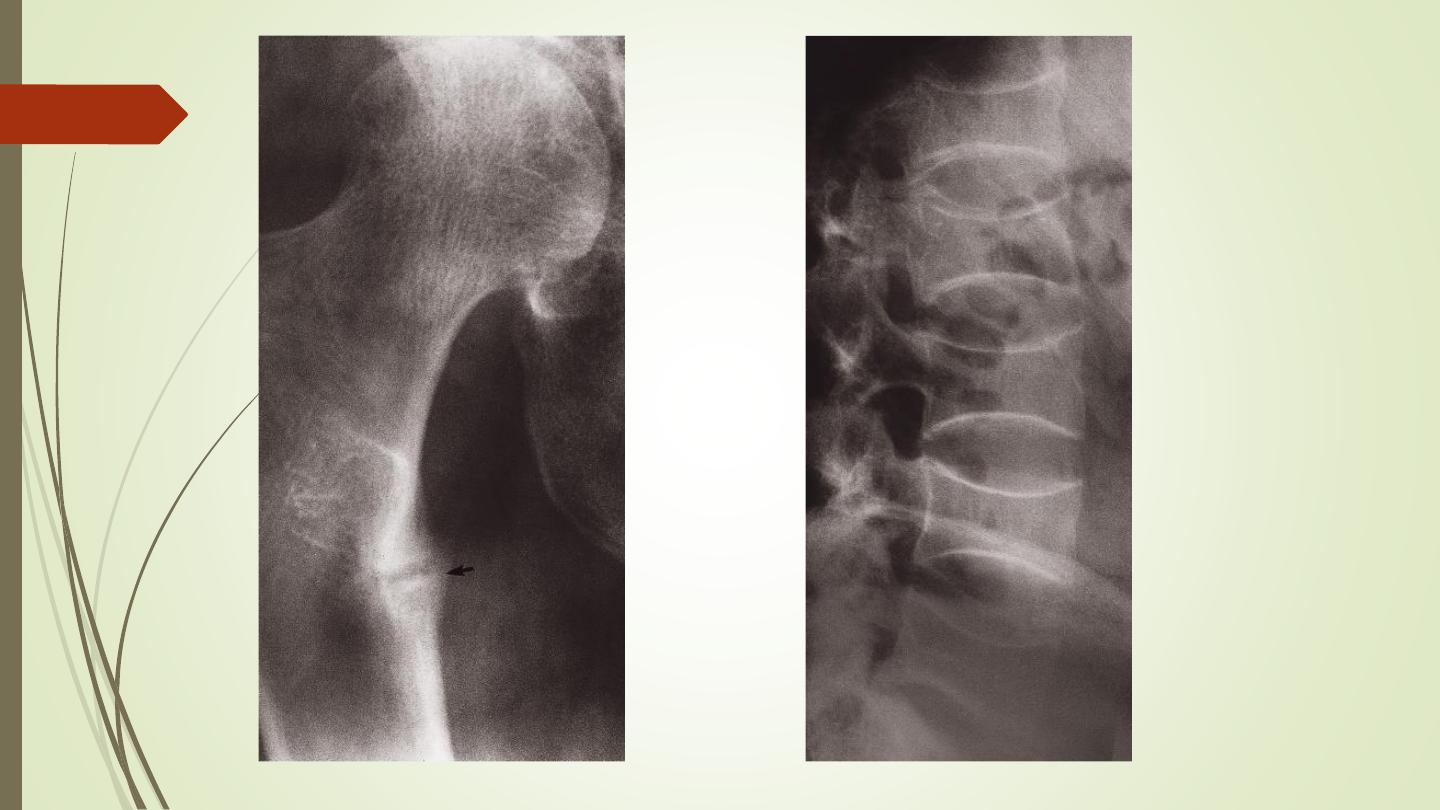
A generalized loss of bone density, with loss of the
differentiation between cortex and medulla. The
trabecular pattern may have a fine lacework
appearance. With advanced disease there may be
marked deformity of the skeleton.
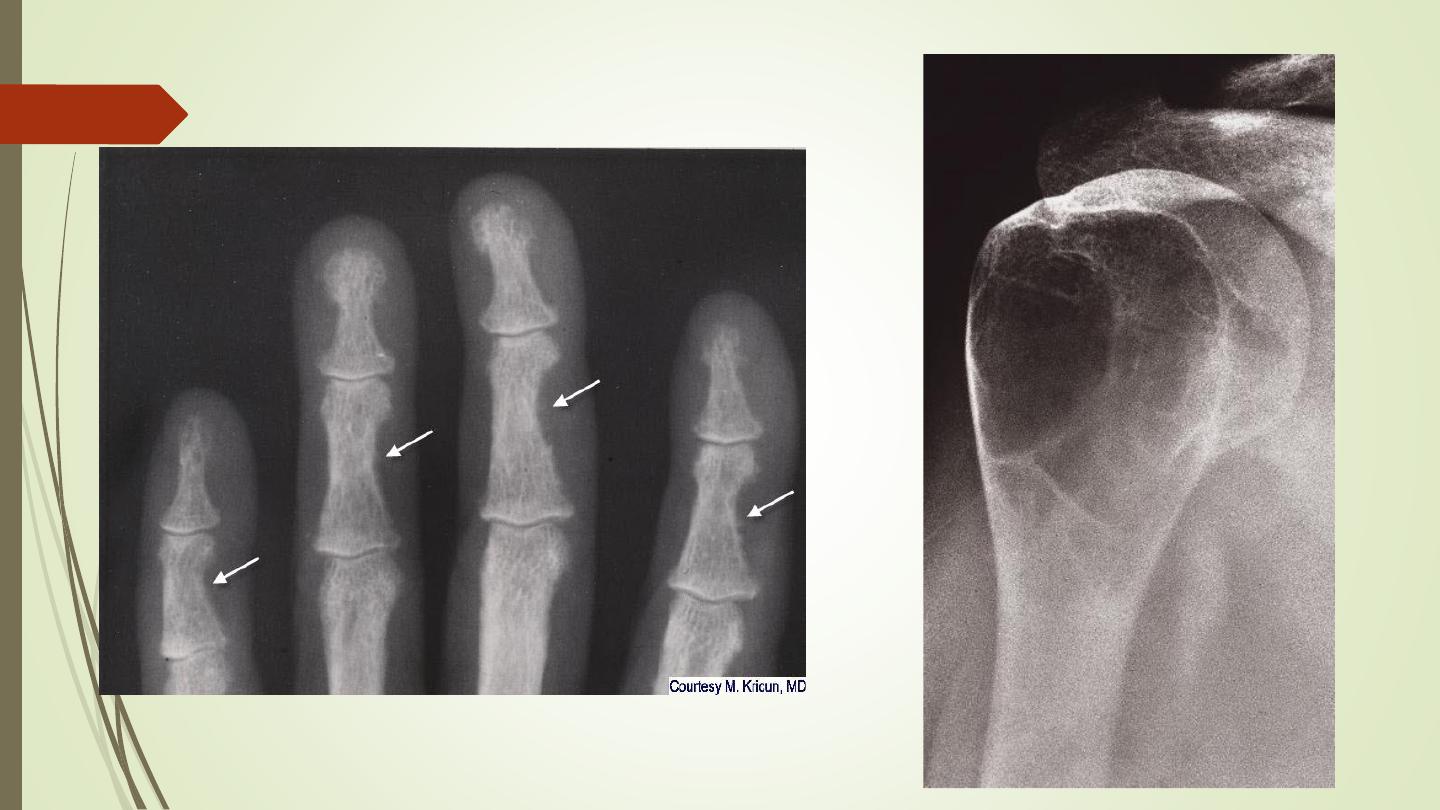
Hyperparathyroidism:
The hallmark of hyperparathyroidism is subperiosteal
bone resorption, particularly at the radial side of the
middle phalanges and at the tips of the terminal
phalanges.
There may also be resorption of the outer ends of the
clavicles.
Soft tissue calcification, vascular calcification and
chondrocalcinosis: more in the secondary type
Brown tumours: seen more in primary type. Lytic lesions,
single or multiple, of varying size and may be expensile.
They occur most commonly in the mandible and pelvis.
Renal osteodystrophy
Three distinct pattern of bony involvement:
❑
Osteomalacia in adults; rickets in children
❑
Hyperparathyroidism
❑
Sclerosis, Rugger jersey spine or sclerosis of the
metaphyses of the long bones.
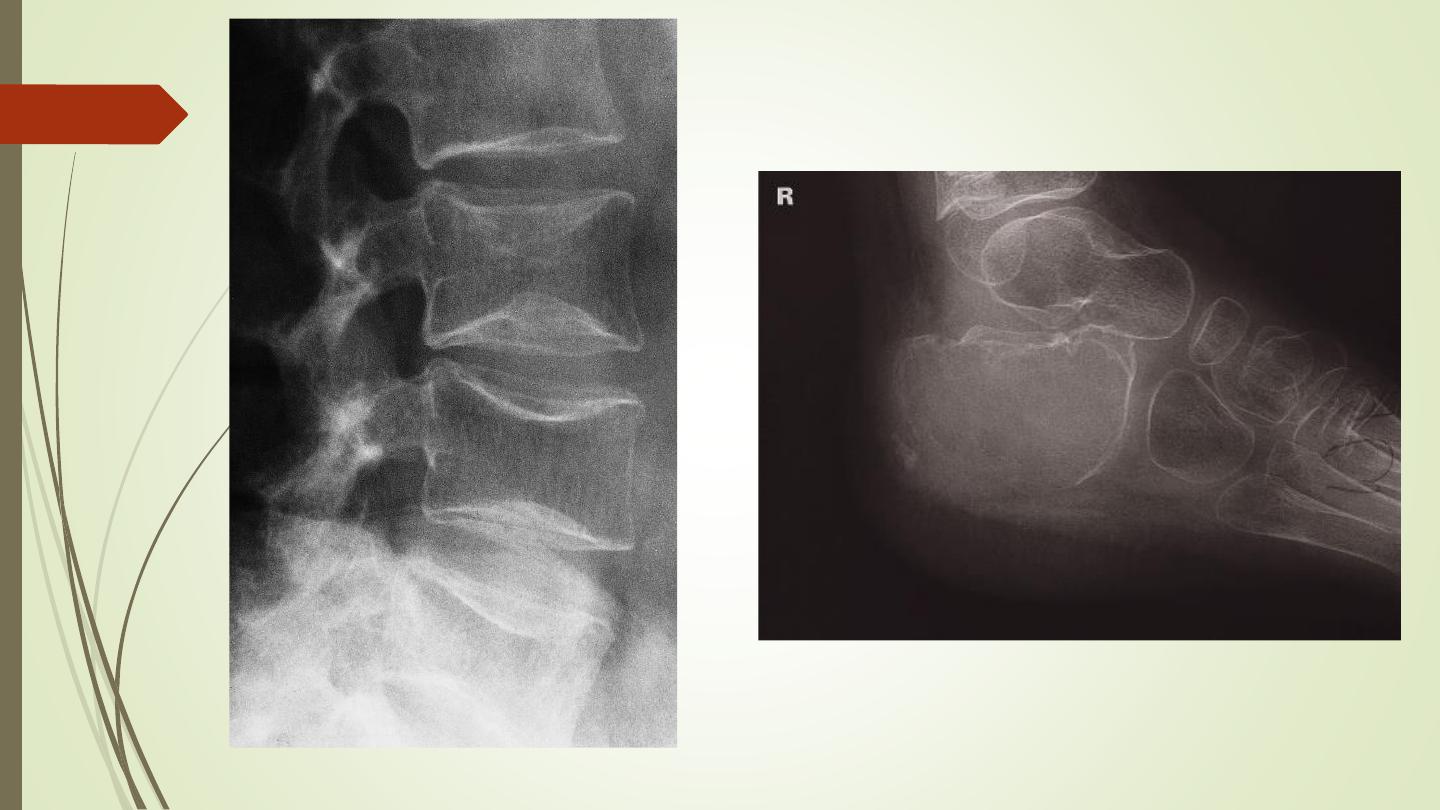
Rugger jersey spine
(Renal osteodystrophy)
Generalized increase in bone density
Sclerotic metastases
Osteopetrosis (marble bone disease):
congenital disease.
Myelosclerosis: is a form of myelofibrosis,
replacement of bone marrow by fibrous tissue.
Splenomegally.
Osteopetrosis
Alteration of trabecular pattern and
change in shape
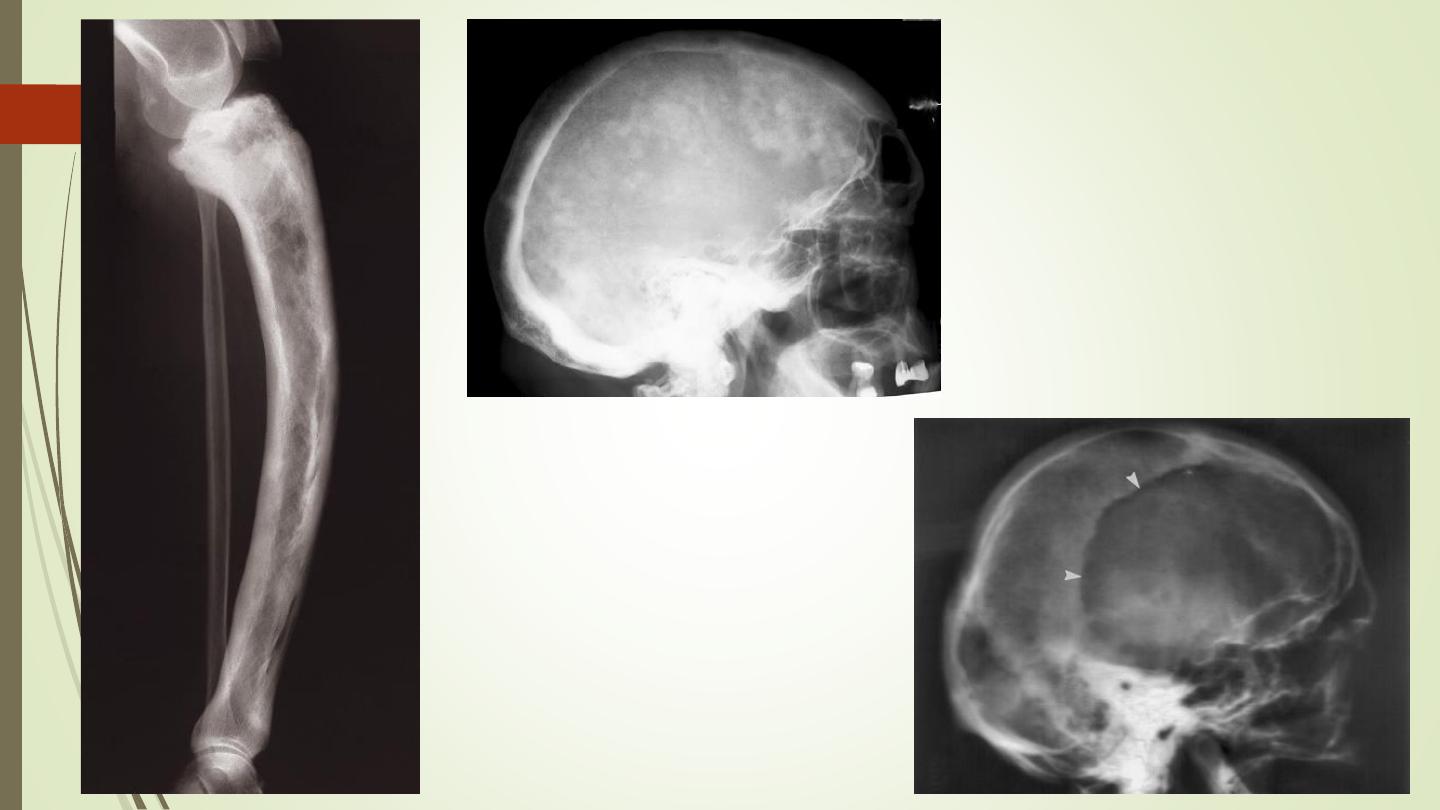
Paget disease:
Elderly
Thickening of trabecula. Enlargement of affected
bone, loss of CM differentiation.
Thickened calvarium with cotton wool appearance.
One form is lytic: osteoporosis circumscripta of skull.
Risk of malignant changes
Alteration of trabecular pattern and
change in shape
Hemolytic anemia:
Marrow hyperplasia: phalanges, skull: hair on end
Infarction and infection

Thank you