Fifth Stage
E.N.T
Dr. Mushtaq – Lecture 6
1
Vertigo
Definition:
•
Illusion of movement
•
Disorder of orientation in space
•
Disagreeable sensation of movement
Anatomy & physiology of balance
The balance depends on the three integrated inputs:
1- vision 70%
2- proprioceptive inputs / joints, skin & muscles. 15%
3- vestibular system 15%
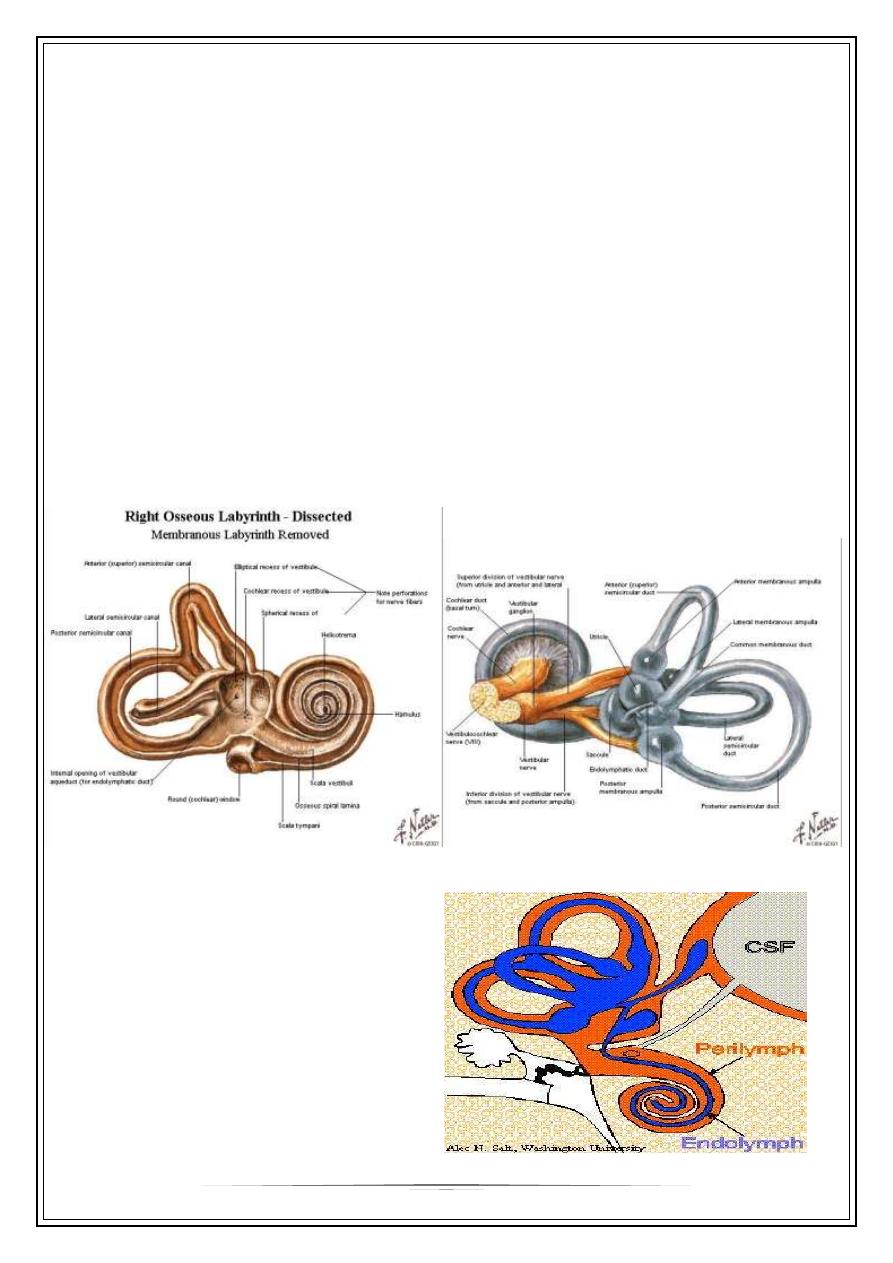
Vestibular anatomy
bony & membranous labyrinths
2
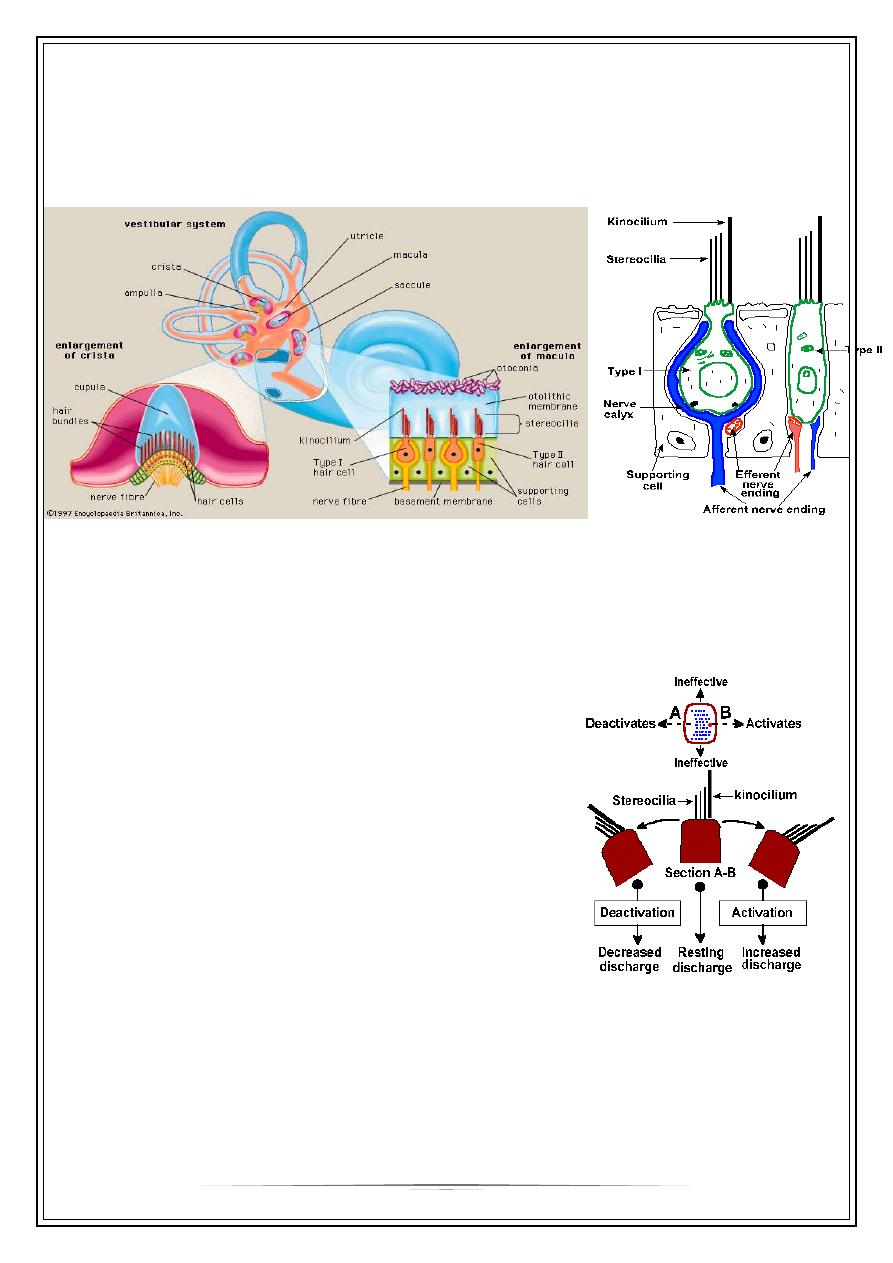
Sensory epithelial cells
1. The sensory epithelium of the utricle, the
utricular macula
,
2. The sensory epithelium of saccule , the
saccular macula
3. s.c.c
crista ampullaris
Macula &crista
Vestibular sensory cells
Vestibular physiology
Utricular macula signals position of head& linear acceleration
Saccule / exact function is not known
S.c.c. angular rotation
Movement of the cilia to kinocillium side results in a
de polarization of the hair cell, a receptor potential
that in turn releases a transmitter substance that
finally depolarizes (the generator potential) the
afferent fibers that contact it .
Vertiginous pts. can be subdivided into :
1-Positional vertigo
2-Vertigo as an isolated symptom
3-Vertigo with deafness & tinnitus
4-Vertigo with other signs of neurological diseases
3
Positional vertigo
A- benign paroxysmal positional vertigo
- brief, sudden attacks of vertigo precipitated by head movement
- horizontal fatigable nystagmus after latent period
- no other aural symptom
- +ve positional test
- normal hearing assessment
Rx: rest , avoid sudden movement & labrynthine sedatives //cinnirizine
B- disequilibrium of ageing
•
Degenerative changes in the maculae & cristae
•
Cervical spondylosis can exacerbate the symptoms
C- Malignant positional vertigo
•
Coarse variable nystagmus , no latent period
•
Non-fatigable
•
e,g; disseminated sclerosis
2- Vertigo as an isolated vertigo
A. Vestibular neuronitis
* frequently preceded by viral infection
* severe vertigo without deafness or tinnitus
* caloric test >>canal paresis on the affected ear
Rx: labr. Sedatives
B- drugs:
1) aminoglycosides e,g; streptomycin, gentamycin.
4
2) metronidazole
3) ethinyl oestrodiol
4) anti-hypertention
C- miscellaneous
•
Anaemia
•
Hypotention
•
D.M.
3-vertigo with deafness & tinnitus
A- Meniere`s disease
* unknown aetiology
* theoretically, an expantion of the endolymphatic compartment >>>
increasing endolymphatic Pr. >>> decreasing the mobility of the basilar
membrane >>> hearing difficulty & tinnitus.
same changes in the vestibular apparatus >>> vestibular dysfunction
Clinical features:
•
Episodes of vertigo + tinnitus & progressive sensorineural deafness
•
5
th
decade
•
Last for 1-24h
•
Nausea & vomiting
•
Normal between attacks
•
Vertiginous symptoms improve although hearing tends to deteriorate
Investigations :
•
Otoscopical ex >>> normal
•
P.T.A >>> fluctuating SNHL
•
Caloric test >>> canal pariesis
Treatment :
Medical :
•
reduce salt & fluid intake
•
reassurance
•
vestibular sedative / cinnirizine
•
vasodilator / betaserc
5
Surgical:
•
Decompression of the endolymphatic sac
•
Vestibular n. section
•
Labyrinthectomy
B. Labyrinthitis: otorrhoea & H . loss
C. Acoustic neuroma: unilateral hearing loss & tinnitus
D. Syphilis
E. Labyrinthine trauma
F. Miscellaneous conditions: wax , eust.dysf. om
4-vertigo + signs of neurological disease
•
Neoplasm involving brain stem ,cerebellum, or mid brain
•
Posterior inferior cerebellar artery thrombosis
•
Vertibrobasilar insufficency
Thank You,