كسووووووووور دكتور وهبي
Shoulder , Acromioclavicular & Elbow Dislocations
Shoulder Dislocation
Why liable?
Wide ROM
Shallow glenoid
Supportive structures
Rotator cuff
Ligaments
Labrum
The least supported is the inferior aspect
Types
Anterior 95%
Posterior 2%
Inferior (luxatio erecta)
Multidirectional
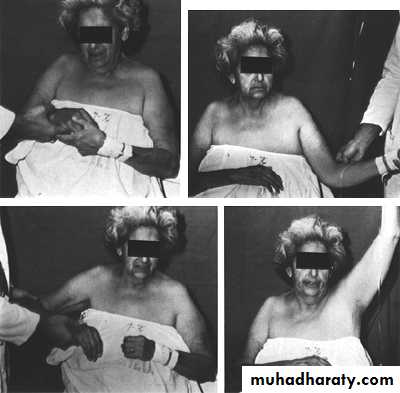
Anterior dislocation
Mechanism
Abduction + extension + external rotation
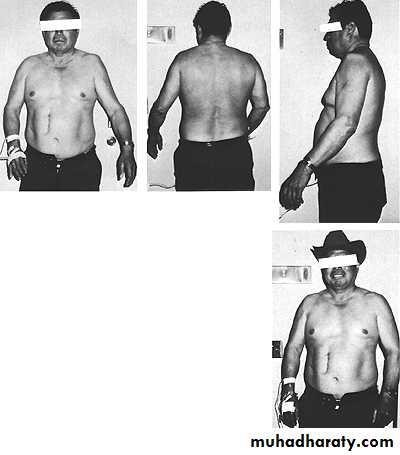
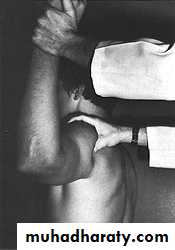
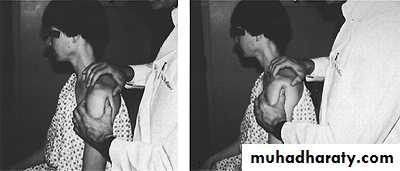
CF
The lateral outline of the shoulder is flattened
Wahby Ghalib10
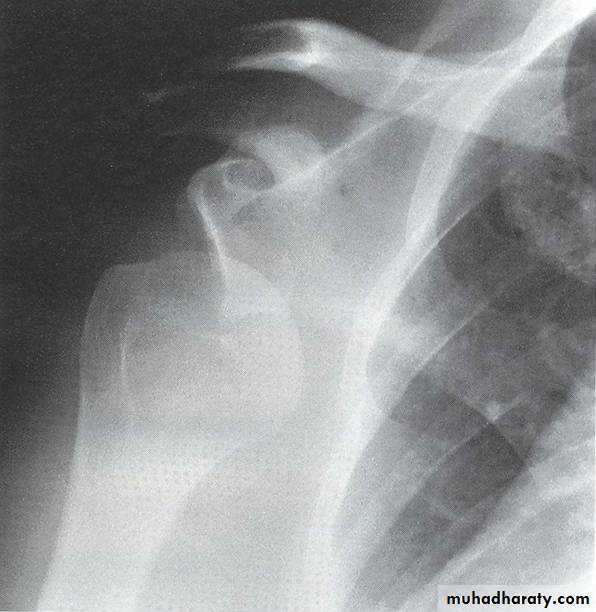
XR
AP
Scapular lateral
Axillary lateral

Reduction
Hippocratic methodStimson method
Kocher method
After reduction
XRTest active abduction
NV examination
Arm sling
Complications
Early
Rotator cuff tear
Nerve injury
Vascular injury
# dislocation
all these are more
common with ↑ age
Late
Recurrent dislocation :
commonest cx
85% < 20y , 15% > 40y
Missed dislocation
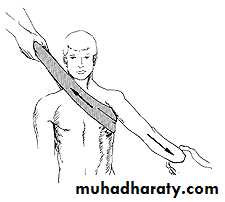
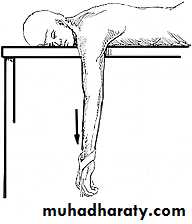
Recurrent dislocation
Apprehension test
Drawer test
Wahby Ghalib26
Recurrent dislocation
Hill – Sachs lesionBankart lesion
Recurrent dislocation
Surgery is indicated if ≥ 3 times per year
Posterior dislocation
Mechanism
Adduction + IR
Convulsion
Electric shock
CF
Arm in IR
XR
Usually missed
AP electrical bulb sign
Scapular lateral
Axillary lateral

Reduction
Traction in adduction then IRAcromioclavicular joint injury
Mechanism
Fall on the shoulder with arm adducted
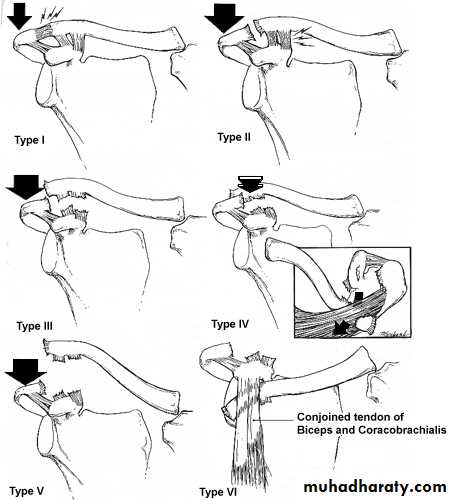
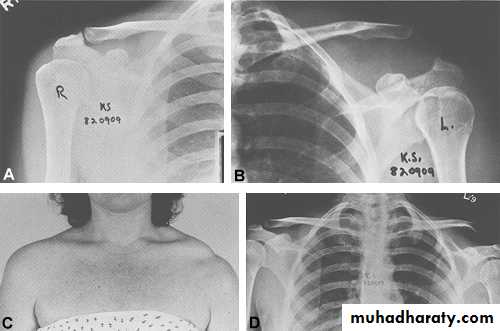
Types
I : sprain of the AC ligament
II : subluxation
III : dislocation
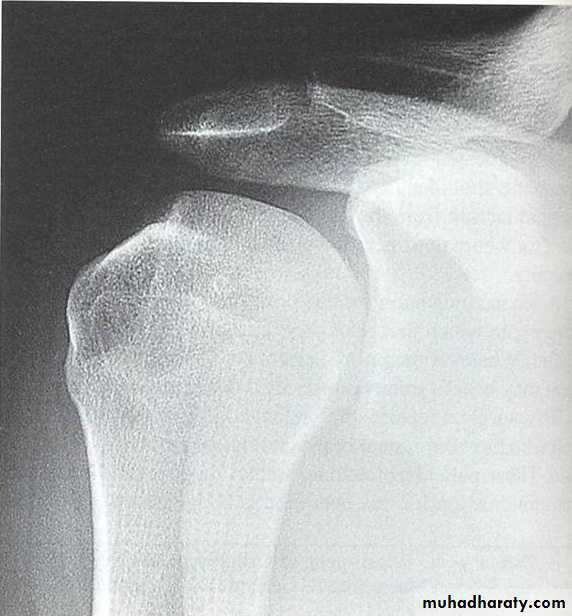
XR
AP view
AP stress view
Rx
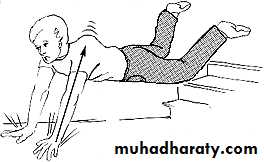
I & II : arm sling exercise
III : if pt is young or demanding occupation repair of the CC ligament + CC screw
Complications
RC syndrome
Missed dislocation
Ossification of ligaments
OA
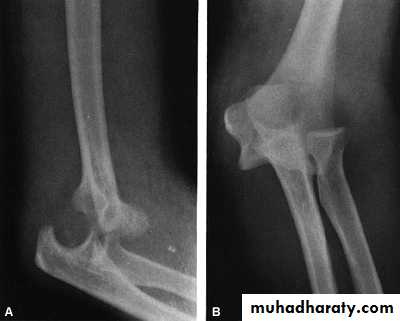
Elbow dislocation
Fall on outstretched hand
Posterior or posterolateral
Simple or complex
Reduction
TractionGradual flexion
Don`t immobilize the elbow > 3w