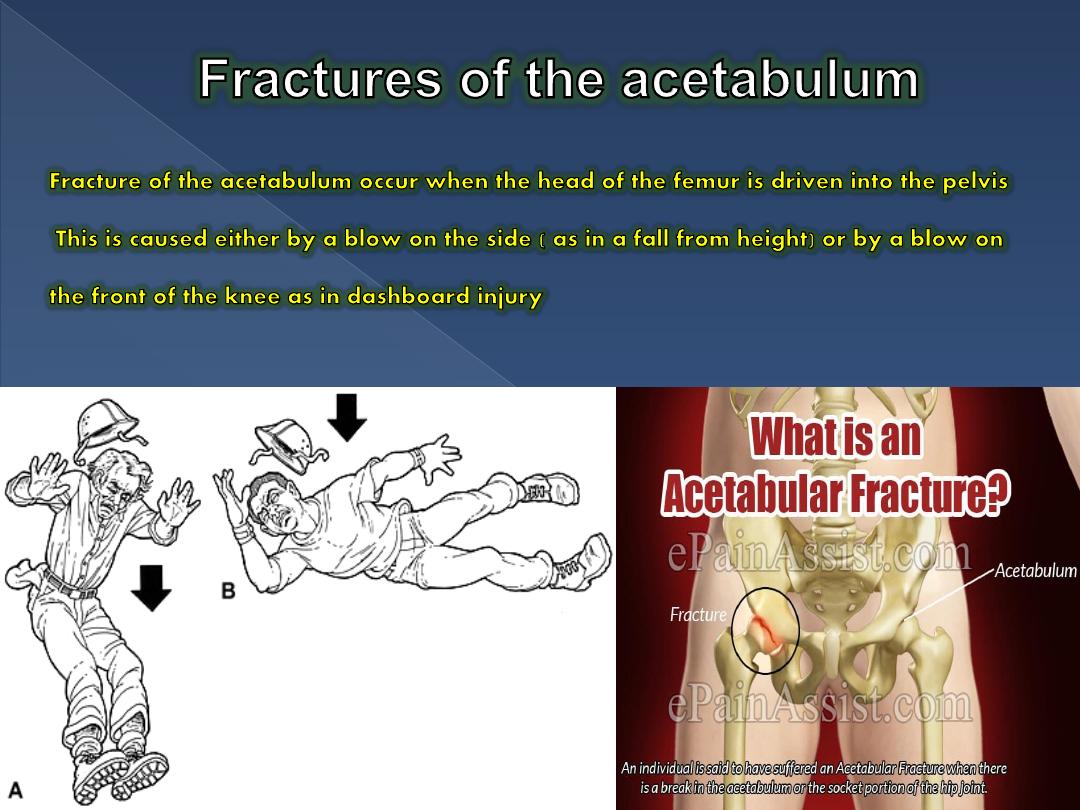
fractures of the acetabulum & injuries to the
sacrum and coccyx
Dr. Jamal Al-Saidy
M.B.Ch.B F.I.C.M.S
Assistant Professor and Consultant Orthopaedic Surgeon
Dr. Jmal Al-Saidy
Undr graduate lecture
Dr. Jmal Al-Saidy
Undr graduate lecture
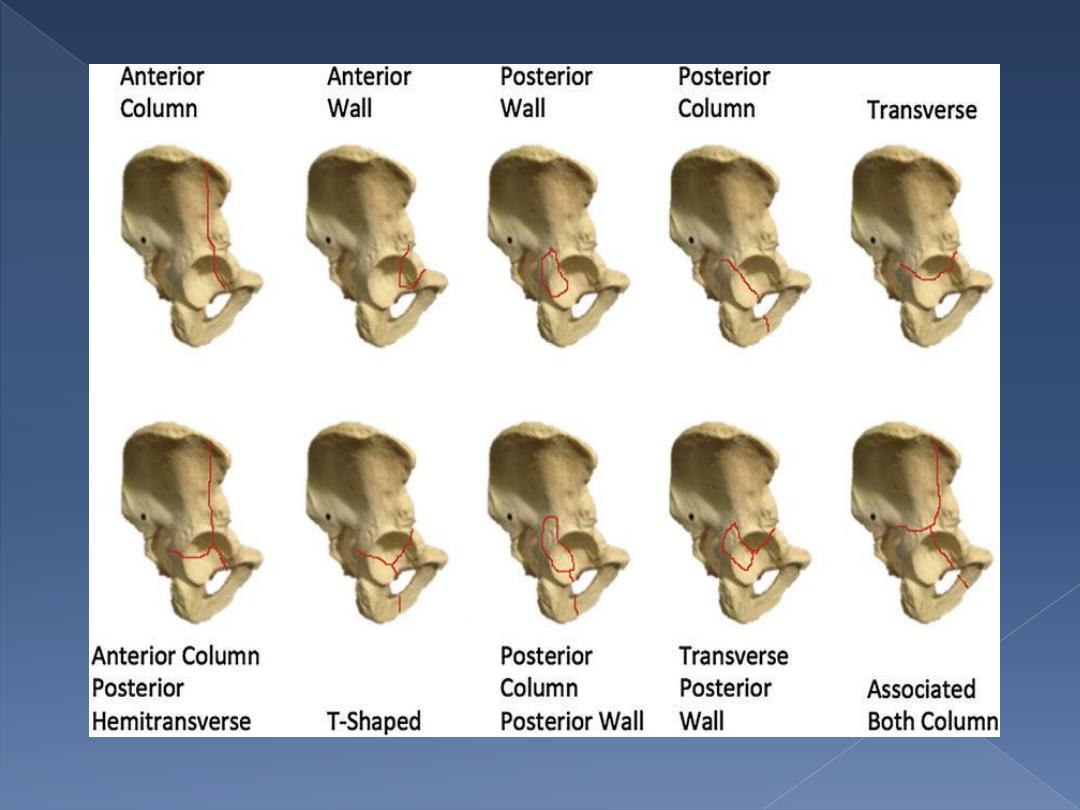
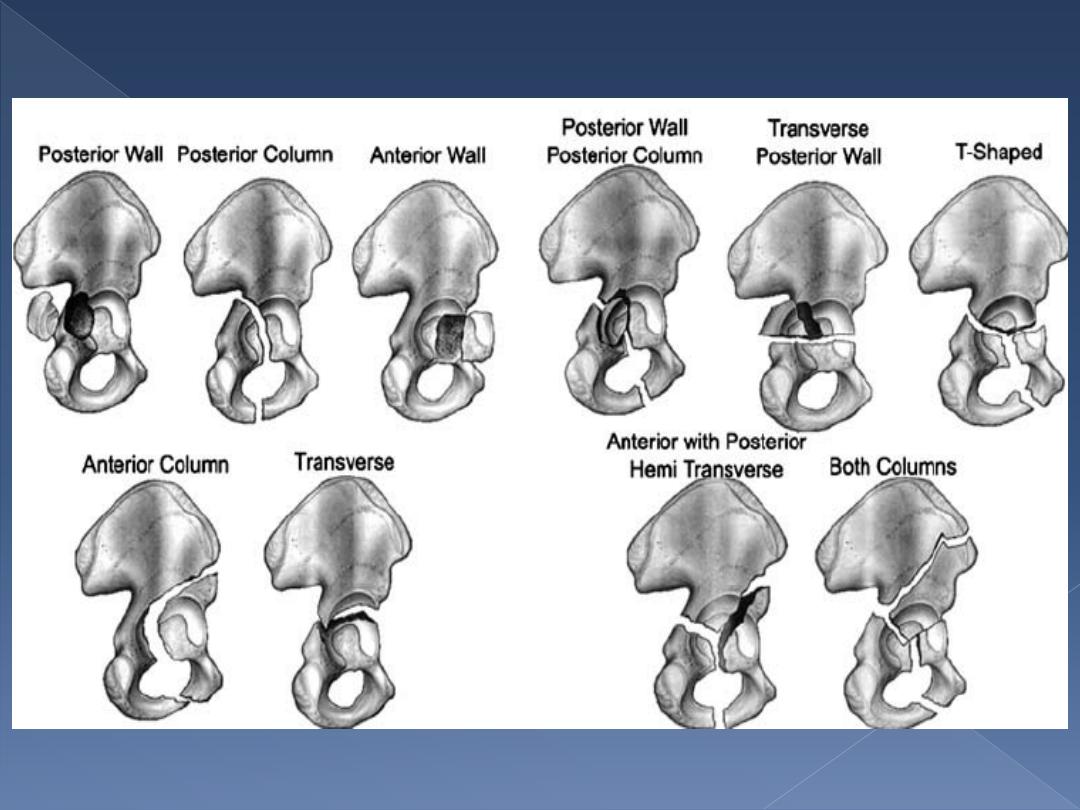
Tile's classification
:-
depend on anatomical ground.
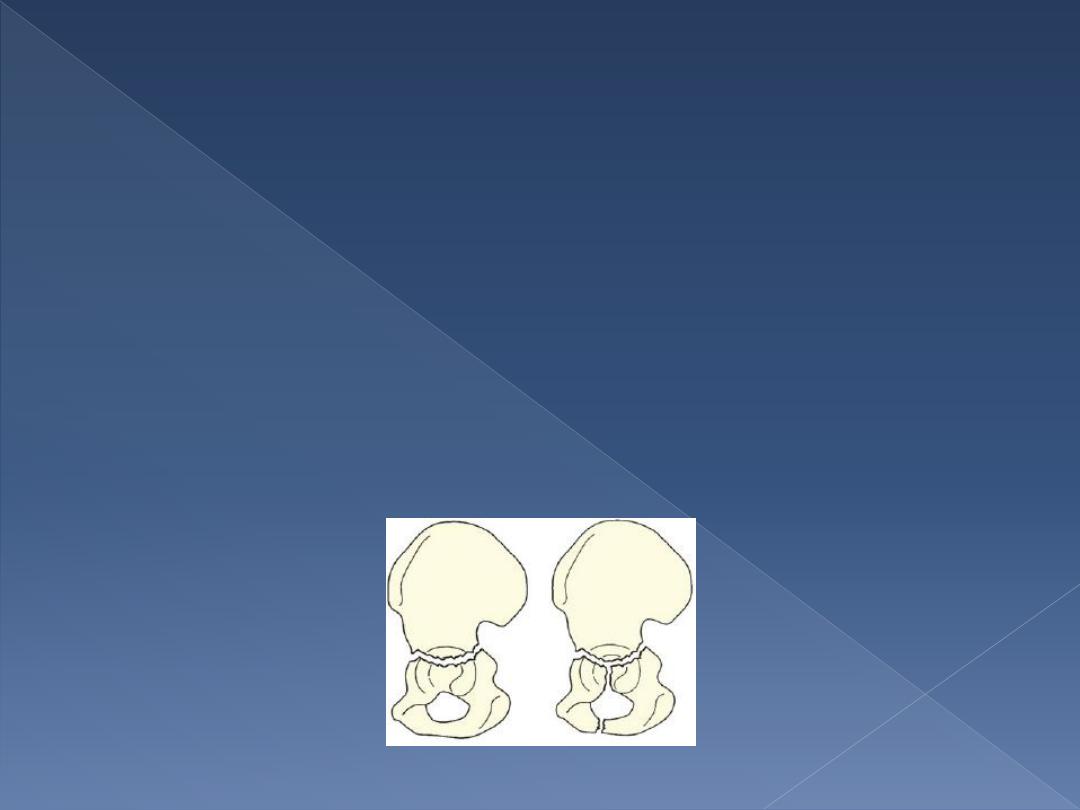
Acetabular wall(rim) fractures:-
•fractures of the anterior or posterior part of the acetabular rim(wall)
affect the depth of the socket and may lead to hip instability unless they
are properly reduced and fixed.
Dr. Jmal Al-Saidy
Undr graduate lecture
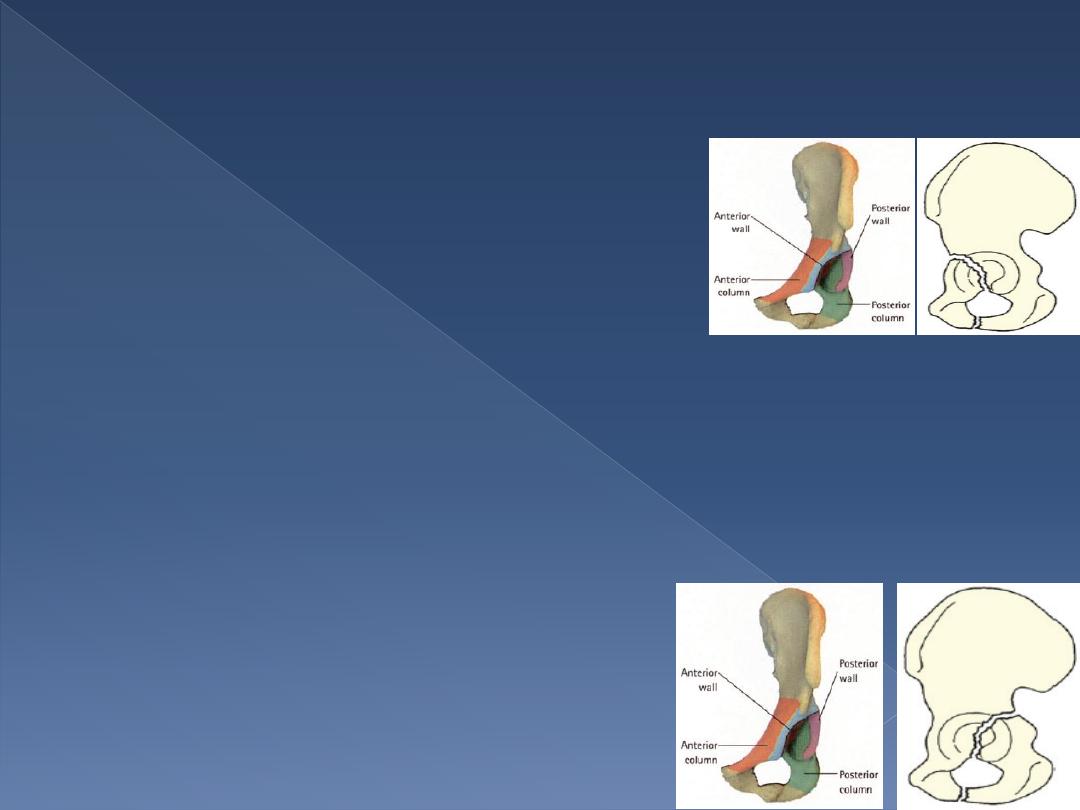
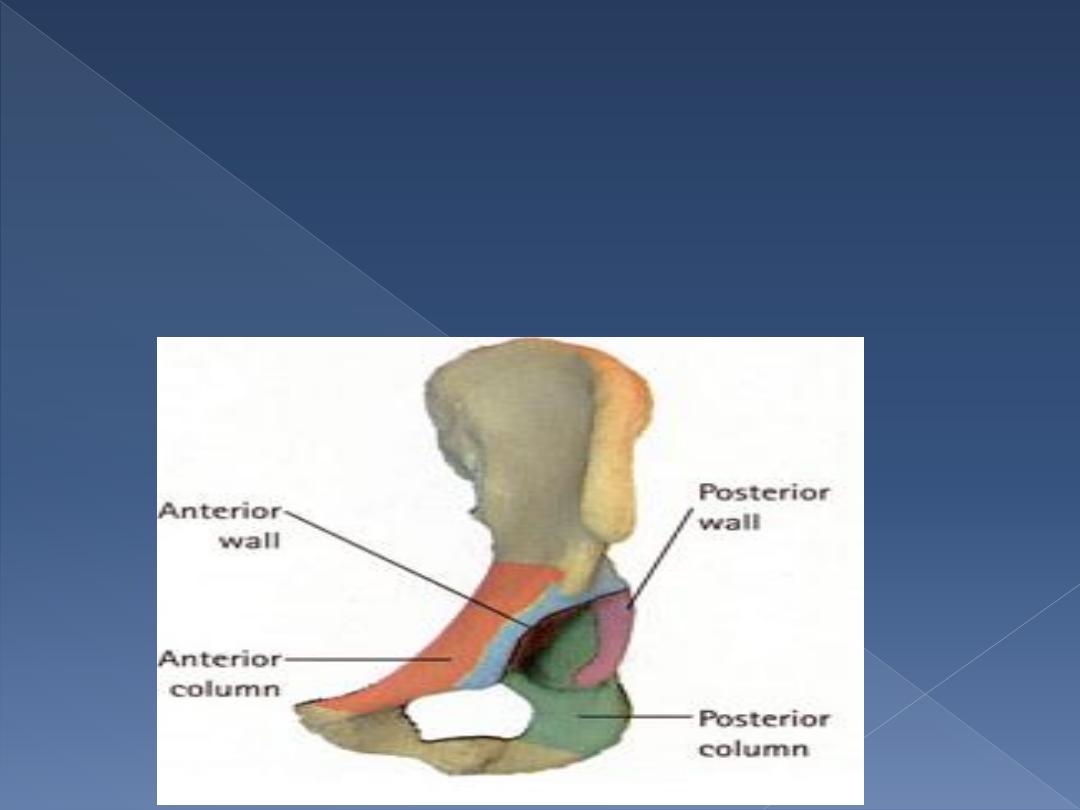
Column fractures :-
anterior
the anterior column extends from the pubic
symphysis, along the
superior pubic ramus,
across the acetabulum to the anterior part of
the ilium.
•Anterior column fractures are uncommon, do not involve the
weight-
bearing area and have a good prognosis.
posterior
The posterior column extends from the ischium, across the posterior aspect of the
acetabular socket to the sciatic notch and the posterior part of
the innominate bone.
•Breaking the weight-bearing part of the acetabulum.
•It is usually associated with a posterior dislocation of
the hip and may injure the sciatic nerve.
•Treatment is more urgent and usually involves internal
fixation to obtain a stable joint.
Dr. Jmal Al-Saidy
Undr graduate lecture
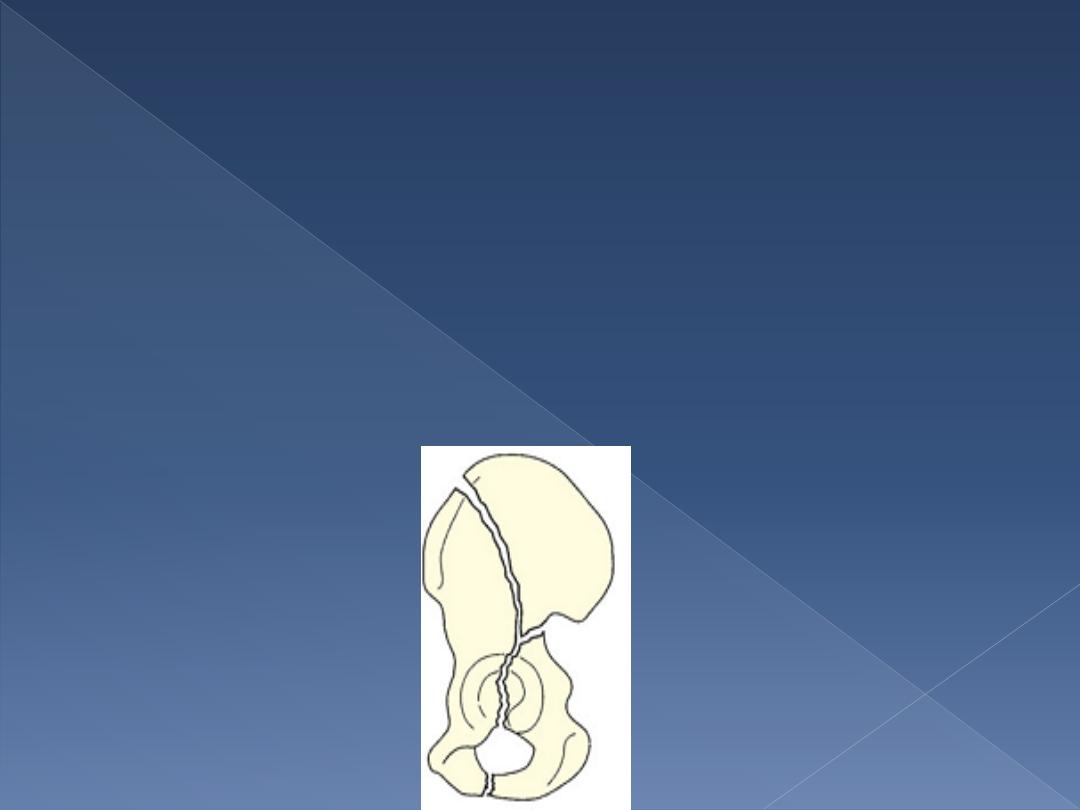
Transverse fracture:-
runs transversely through the acetabulum, involving both the anterior and posterior
columns, and separating the iliac portion above from the pubic and ischial portions
below.
•A vertical split into the obturator foramen may coexist, resulting in a T-fracture.
•Difficult to reduce and to hold reduced.
Dr. Jmal Al-Saidy
Undr graduate lecture
Complex fracture:-
•are complex injuries which damage either the anterior or the
posterior columns (or both) as well as the roof or the walls of the
acetabulum.
•the injury is severe.
•The joint surface is disrupted.
•They usually need operative reduction and internal fixation.
•The end result is likely to be less than perfect, unless surgical reduction
.
Dr. Jmal Al-Saidy
Undr graduate lecture

Clinical features
Usually a severe injury; either a traffic accident or a fall from a height.
Associated fracture:- whenever a fractured femur, severe knee injury or a fractured
calcaneum is diagnose, the hips also should be x-rayed.
May be severely shocked, and the complications associated with all pelvic fractures
should be excluded.
Rectal examination is essential.
There may be bruising around the hip and the limb may lie in internal rotation (if the
hip is dislocated).
Careful neurological examination is important, testing the function of the sciatic,
femoral, obturator and pudendal nerves.
Imaging
At least four x-ray views should be obtained in every case: a standard anteroposterior
view, the pelvic inlet view and two 45 degrees oblique views. Each view shows a
different profile of the acetabulum.
CT scans and three-dimensional re-formations are added refinements, and are
particularly helpful if surgical reconstruction is planned.
Dr. Jmal Al-Saidy
Undr graduate lecture
Treatment
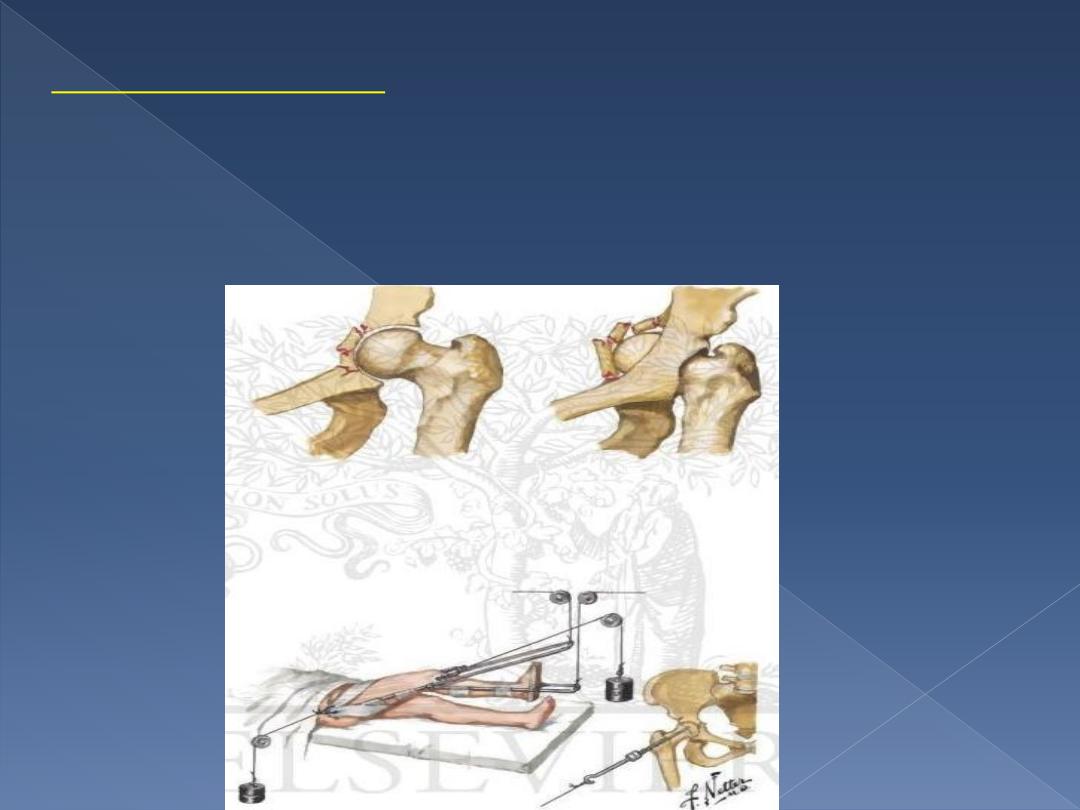
EMERGENCY TREATMENT
The first is shock and reduce a dislocation.
Skeletal traction to the distal femur (10 kg will suffice).
Occasionally, additional lateral traction through the greater trochanter is needed for central
hip dislocations.
Definitive treatment of the fracture is delayed until the patient is fit and operation facilities
are optimal.
Dr. Jmal Al-Saidy
Undr graduate lecture

NON-OPERATIVE TREATMENT
Conservative treatment :
is still preferable in certain well-defined situations:
* minimal displacement (in the weightbearing zone, less than 3 mm)
* not involve the superomedial weight bearing segment (roof) .
* a both-column fracture that retains the ball and socket congruence of the hip.
* fractures in elderly patients, where closed reduction seems feasible.
* patients with ‘medical’ contraindications, local
sepsis)
* Comminution, unless adequate facilities and expertise are available.
Non-operative treatment is more suitable for patients aged over 50 years than for adolescents and
young adults.
If there are medical contraindications to operative treatment, closed reduction under general
anaesthesia is attempted.
In all patients treated conservatively,longitudinal traction, if necessary supplemented by lateral
traction, is maintained for 6–8 weeks; this will unload the articular cartilage and will help to prevent
further displacement of the fracture.
During this period, hip movement and exercises are encouraged.
The patient is then allowed up, using crutches with minimal weightbearing for a further 6 weeks.
Dr. Jmal Al-Saidy
Undr graduate lecture
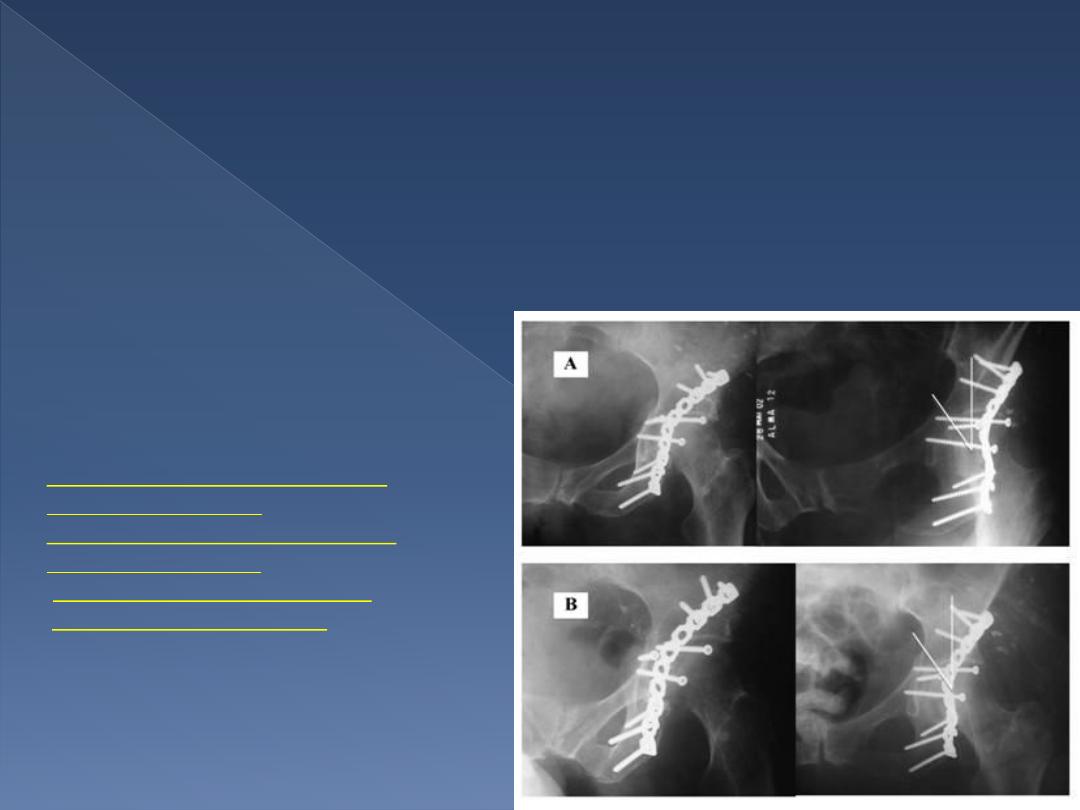
OPERATIVE TREATMENT
•
indicated for all unstable hips.
•The hip may be dislocated centrally, anteriorly or posteriorly.
•The fracture (or fractures) is fixed with lag screws or special buttressing plates.
•Prophylactic antibiotics are used.
•Postoperatively hip movements are started as soon as possible.
•Some prophylaxis against heterotopic ossification is often used, usually indomethacin.
•The patient is allowed up, partial weightbearing with crutches, after 7 days.
•Exercises continued for 3–6 months; it may take a year or longer for full function to return.
Complications
o
Iliofemoral venous thrombosis
o
Sciatic nerve injury
o
Hereterotopic bone formation
o
Avascular necrosis
o
Loss of joint movement and
secondary osteoarthritis
Dr. Jmal Al-Saidy
Undr graduate lecture
Internal fixation of fracture acetabulum
Dr. Jmal Al-Saidy
Undr graduate lecture
Dr. Jmal Al-Saidy
Undr graduate lecture
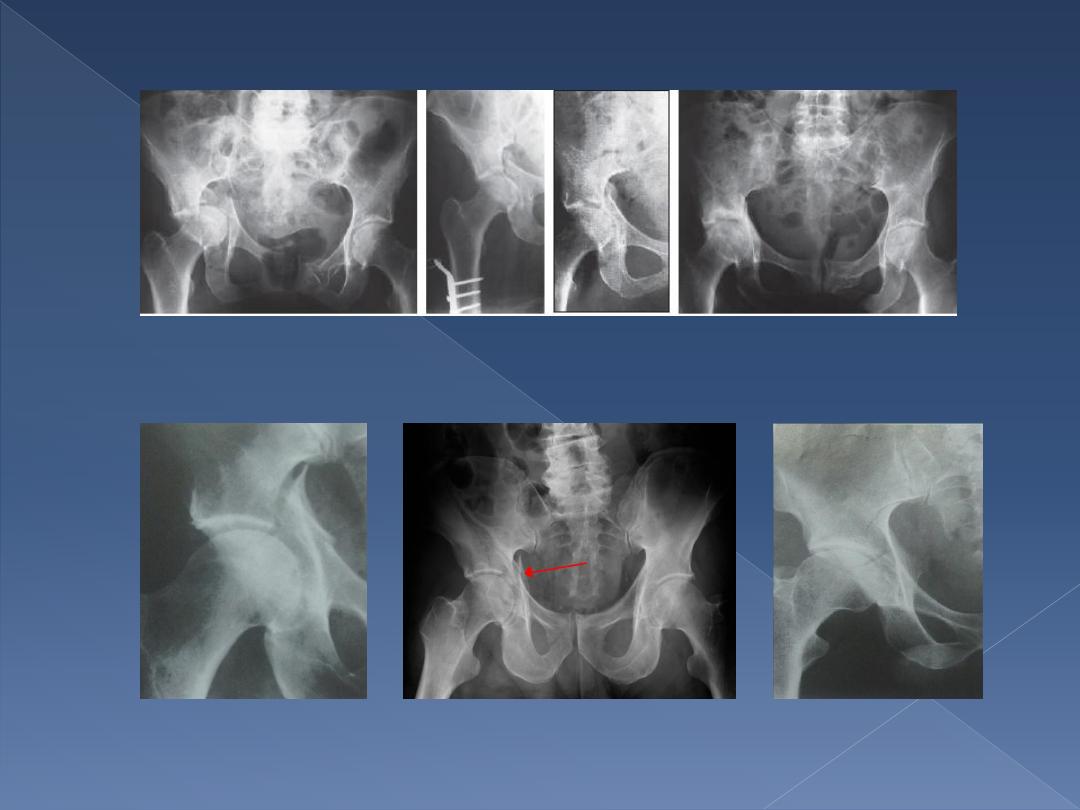
X- ray
Dr. Jmal Al-Saidy
Undr graduate lecture
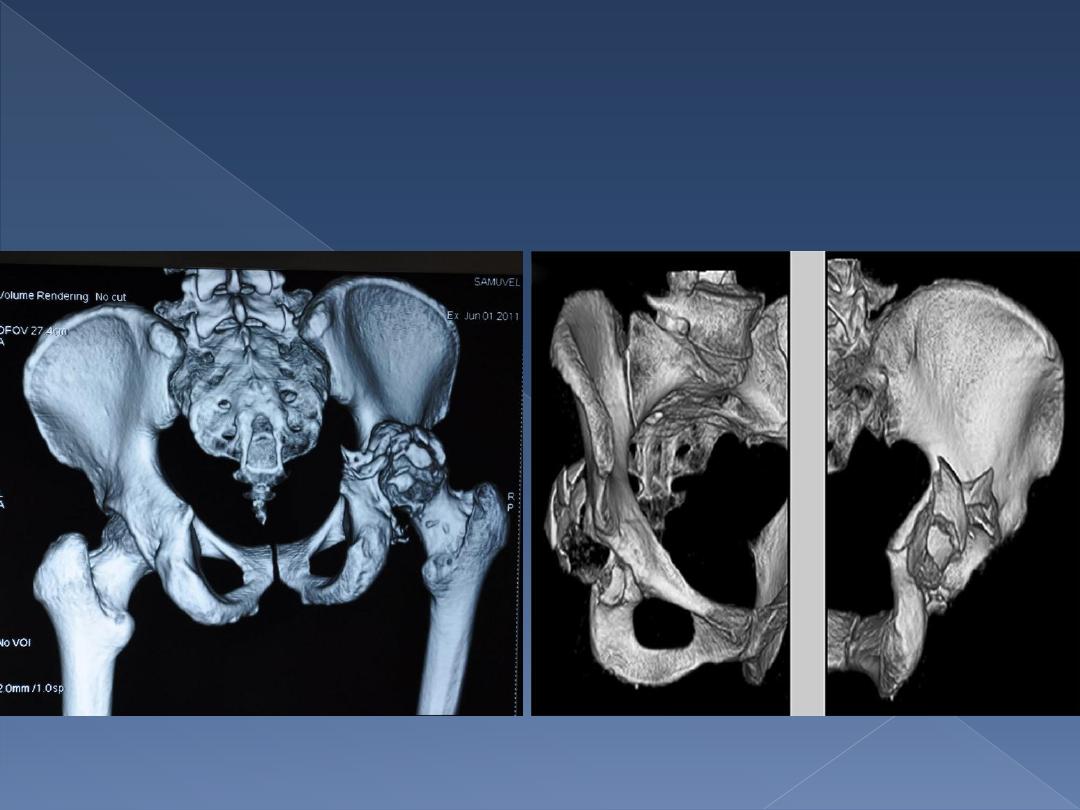
CT Scan
Dr. Jmal Al-Saidy
Undr graduate lecture
I
NJURIES TO THE SACRUM AND COCCYX
•blow from behind.
•Fall in to tail.
•Women seem to be affected more .
•Bruising.
•Tenderness.
•Sensation may be lost over sacral n.
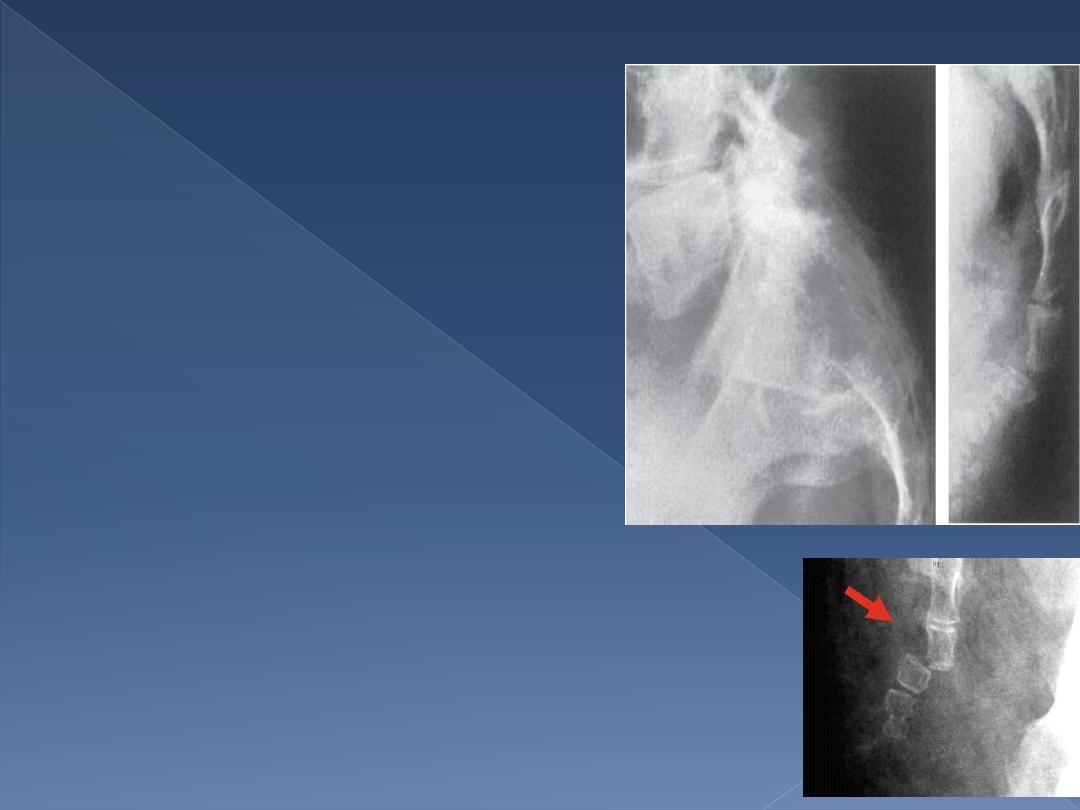
X-rays :-
1- transverse fracture of the sacrum.
2- Fractured coccyx.
3- normal appearance if the joint sprain.
Treatment :-
•reduction by a finger in the rectum.
•The reduction is stable.
•If not , advised to use a rubber-ring cushion when sitting.
•Occasionally, sacral fractures are associated with urinary
problems.
•Laminectomy.
•Persistent pain on sitting is common after coccygeal injuries.
•If the pain not relieved by the use of a cushion or by the injection
of local anesthetic into the tender area, excision of the coccyx
may be considered………………………….
Dr. Jmal Al-Saidy
Undr graduate lecture

Dr. Jmal Al-Saidy
Undr graduate lecture