Fifth Stage
Orthopedics
Dr. Haider – Lecture 5
1
Late Complications of Fractures
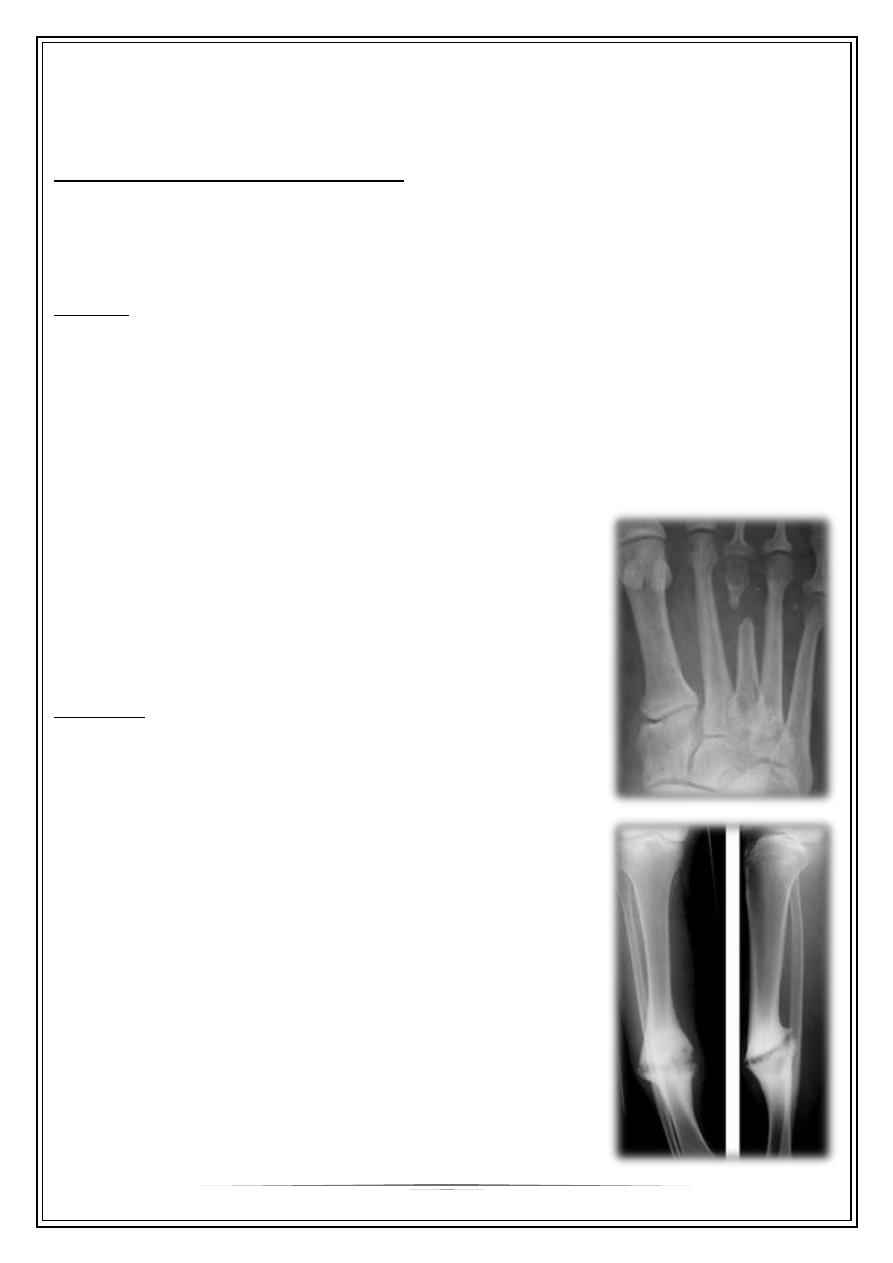
Delayed union and non union :
When the fracture takes more time than expected to unite then it is delayed union
When the fracture fail to unite . For diagnosis of non union , 6 months of follow up
should pass without clinical and\or radiological signs of union.
Causes :
—
Biological : - inadequate blood supply
- severe soft tissue damage
- excessive periosteal stripping
- infection
—
Biomechanical : - inadeqaute reduction
- unstable fixation
- infection
—
Patient related : - medical conditions like DM
- non compliant patient
Diagnosis:
Delayed union : fracture tenderness persist , fracture
line in the xray with very little or no callus
Non union : pain diminished , movement in the
fracture site (pseudarthrosis or pseudojoint ) , xray show
atrophic or hypertrophic bone ends
Treatment :
Delayed union : look for and treat the cause .
Non union : treated mainly by surgical fixation with
bone graft ( in Atrophic non union or without bone
graft in cased of hypertrophic Non union.
2
Malunion:
When the fragments join in an unsatisfactory position (unacceptable angulation,
rotation or shortening) the fracture is said to be malunited.
Causes are failure to reduce a fracture adequately, failure to hold reduction while
healing proceeds
Treatment of malunited fracture:
In adults, Angulation of more than 10–15 degrees in a long bone or a noticeable
rotational deformity may need correction by re- manipulation, or by osteotomy and
fixation .
In children, angular deformities near the bone ends (and especially if the
deformity is in the same plane as that of movement of the nearby joint) will usually
remodel with time; rotational deformities will not
Shortening malunion may be treated by bone lengthening procedure.
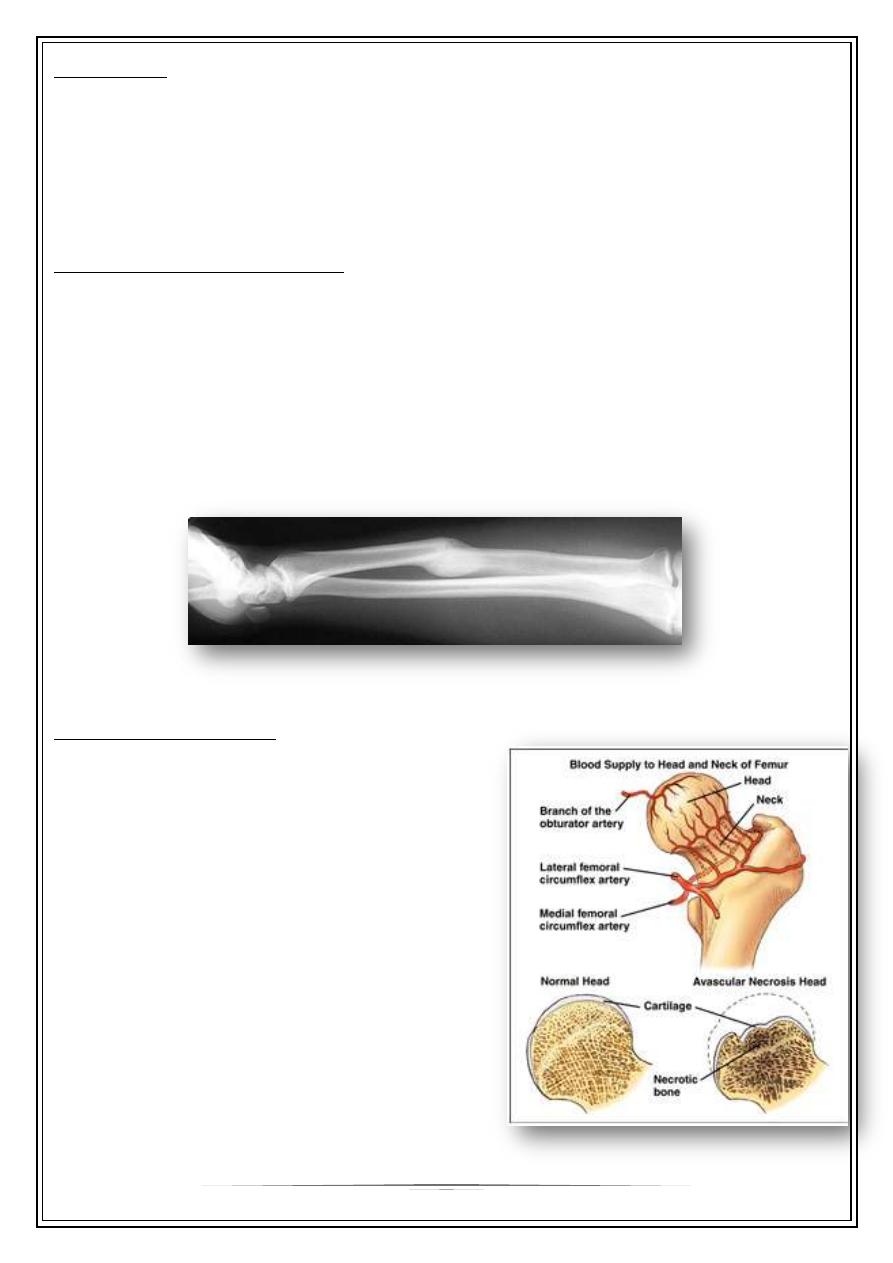
Avascular necrosis:
Certain regions are problematic for their
tendency to develop ischemia and bone
necrosis after injury.
They are:
- the head of the femur (after fracture of the
femoral neck or dislocation of the hip);
- the proximal part of the scaphoid (after
fracture through its waist);
- the body of the talus (after fracture of its
neck).
—
Accurately speaking, this is an early
complication of bone injury, because
ischemia occurs during the first few
hours following fracture or dislocation.
3
However, the clinical and radiological effects
are not seen until weeks or even months
later.
Clinical features of AVN :
-
Pain
-
Increased bone density in the radiography
Treatment :
-
Femoral head AVN – total hip arthroplasty
or arthrodesis
-
Scaphoid or talus – conservative treatment or joint arthrodesis
Joint stiffness :
—
Commonly occurs in the knee, elbow, shoulder and (worst of all) small joints of the
hand.
—
Due to oedema and fibrosis of the capsule, ligaments and muscles around the
joint, or adhesions of the soft tissues to each other or to the underlying bone.
—
Made worse by prolonged immobilization
—
What is important is to prevent stiffness and to insist on skilled physiotherapy
until normal function is restored.
Treatment of joint stiffness :
-
Extensive physiotherapy
-
Arthroscopic release of adhesions
-
Open surgical release of adhesions ( ex. Stiff knee )
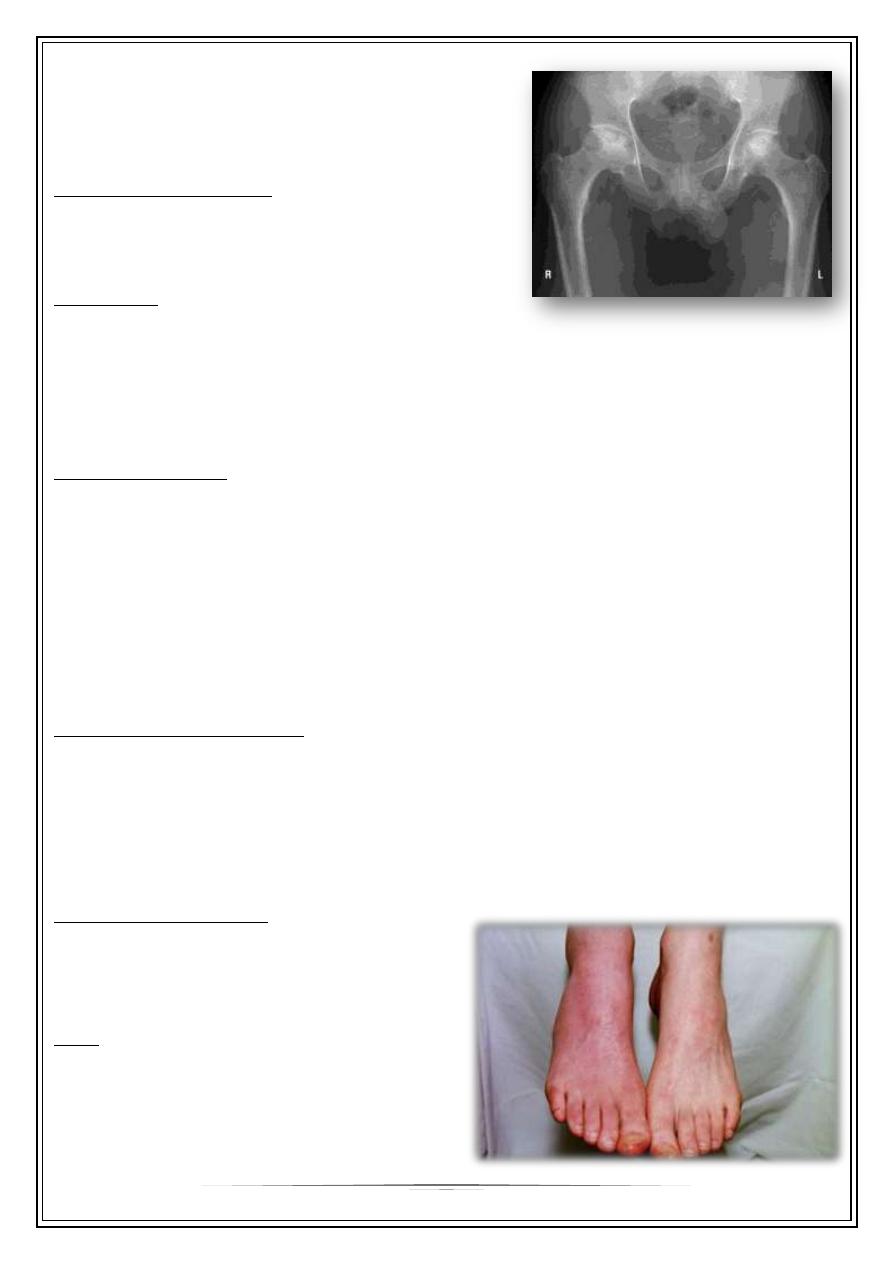
Sudeck’s atrophy :
Algodystrophy , reflex sympathetic
dystrophy , complex pain regional syndrome
( all refer to same entity )
C.F. :
—
Continuous ‘ burning ‘ pain. local
swelling, redness and warmth, and
tenderness.
4
—
After few weeks the skin becomes pale
and atrophic, movements are
increasingly restricted.
—
X-rays characteristically show patchy
rarefaction of the bone.
Treatment :
- Elevation and active exercises are
essential to prevent and to treat CRPS.
- antiinflammatory drugs and adequate
analgesia are helpful.
- use of drugs like amitriptyline,
carbamazepine , gabapentin and
calcium channel blockers may help.
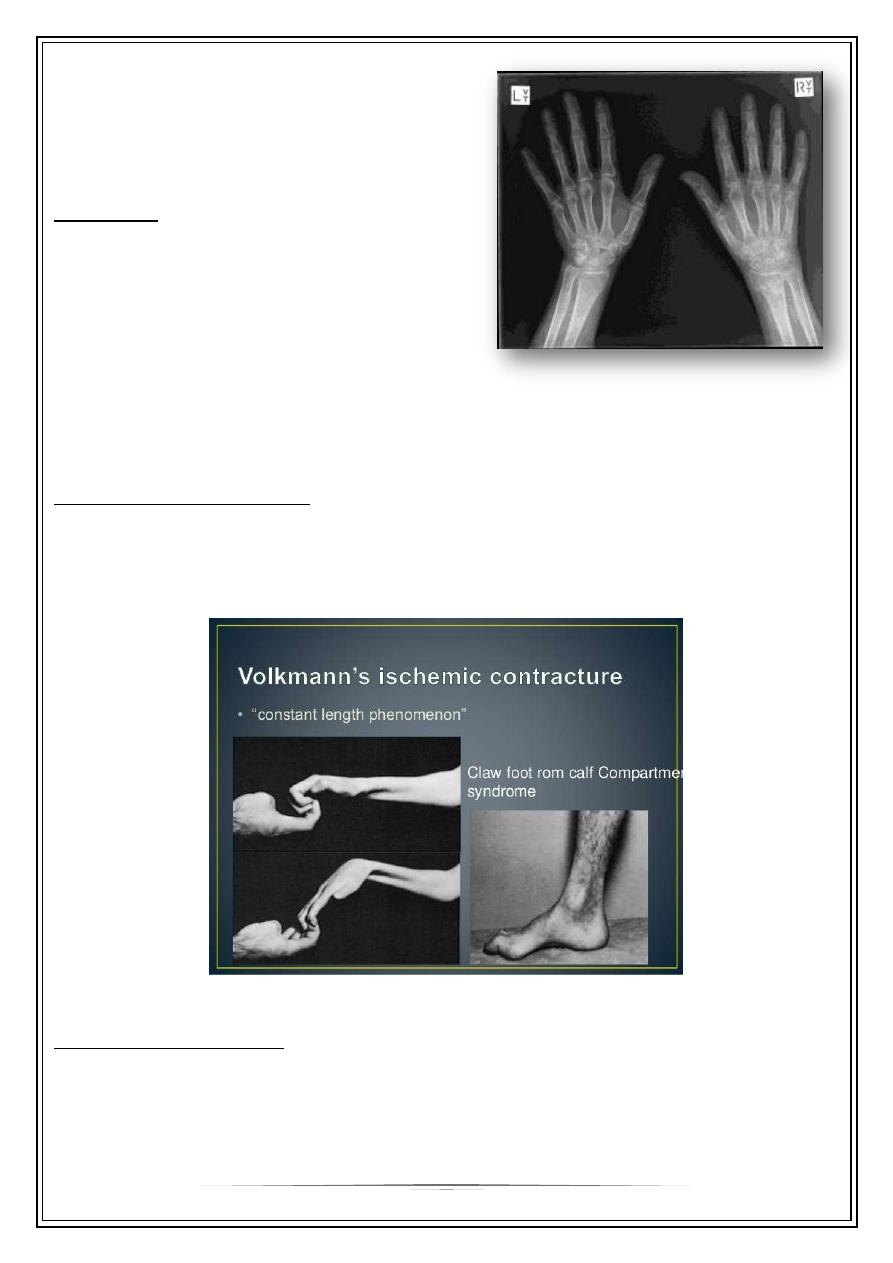
Ischemic contracture :
Following arterial injury or compartment syndrome, the patient may develop
ischaemic contractures of the affected muscles (Volkmann’s ischaemic contracture).
The sites most commonly affected are the forearm and hand, leg and foot.
Myositis ossificans :
—
Heterotopic ossification in the muscles
—
Common sites : elbow or a blow to the brachialis, deltoid or quadriceps. especially
in unconscious or paraplegic patients
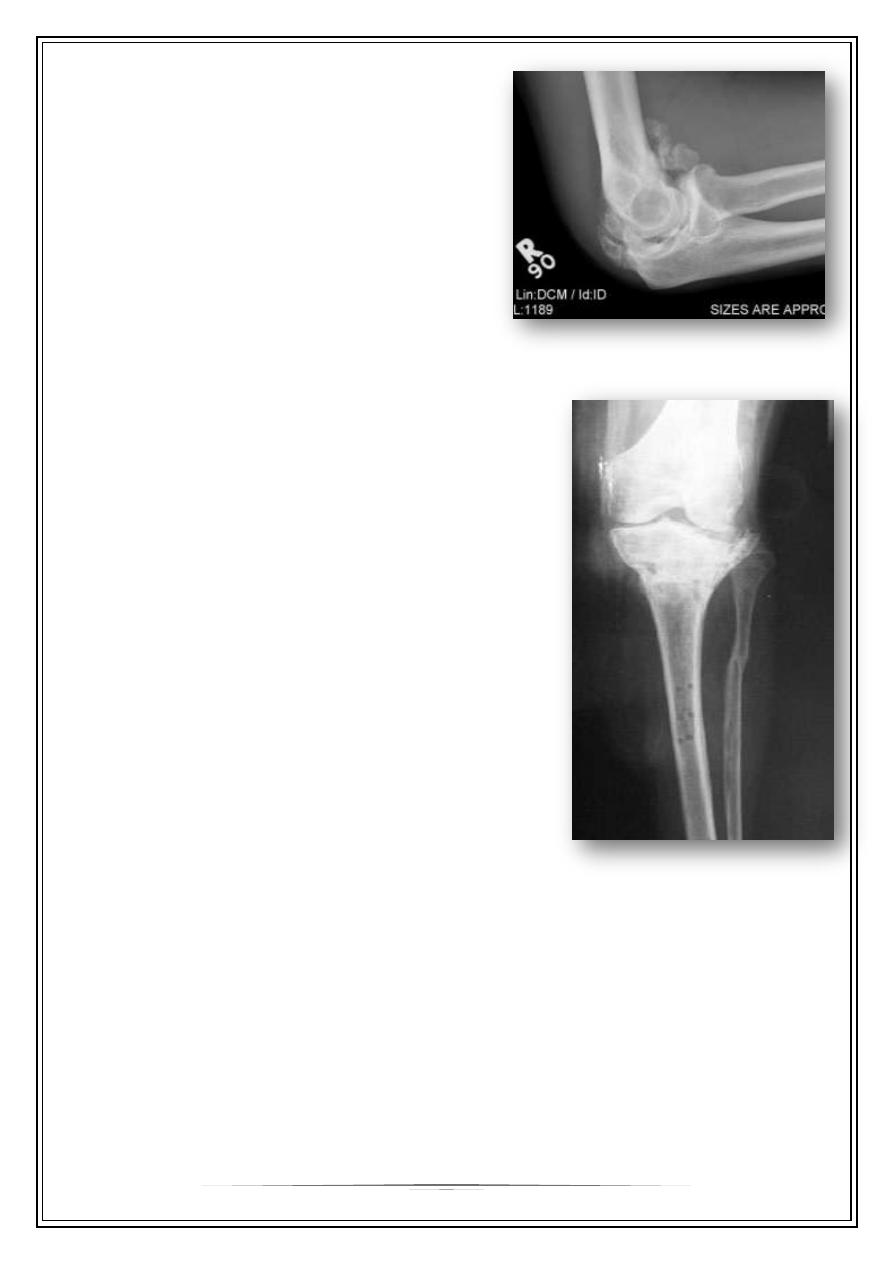
5
—
x-ray may show fluffy calcification in the
soft tissues.
—
The joint should be rested in the position
of function until pain subsides; gentle
active movements are then begun.
—
Months later, when the condition has
stabilized, it may be helpful to excise the
bony mass.
—
Indomethacin or radiotherapy should be
given to help prevent a recurrence.
Degenerative arthritis (osteoarthritis ) :
A fracture involving a joint may severely damage
the articular cartilage and give rise to post-traumatic
osteoarthritis.
Even if the cartilage heals, irregularity of the joint
surface may cause localized stress and so predispose
to secondary osteoarthritis years later..
Thank You,,,