
Valvular heart diseases:-
It's either congenital or acquired lesions, some occur in isolation and other in
association with other heart diseases.
The abnormal cardiac valves cause disease by two major mechanisms:-
1-They impose a major homodynamic burden on the cardiac chambers by
causing obstruction (stenosis) or regurgitation (incompetence) or sometimes
combination of two.
2- The abnormal valves are more susceptible to infections and its
complications.
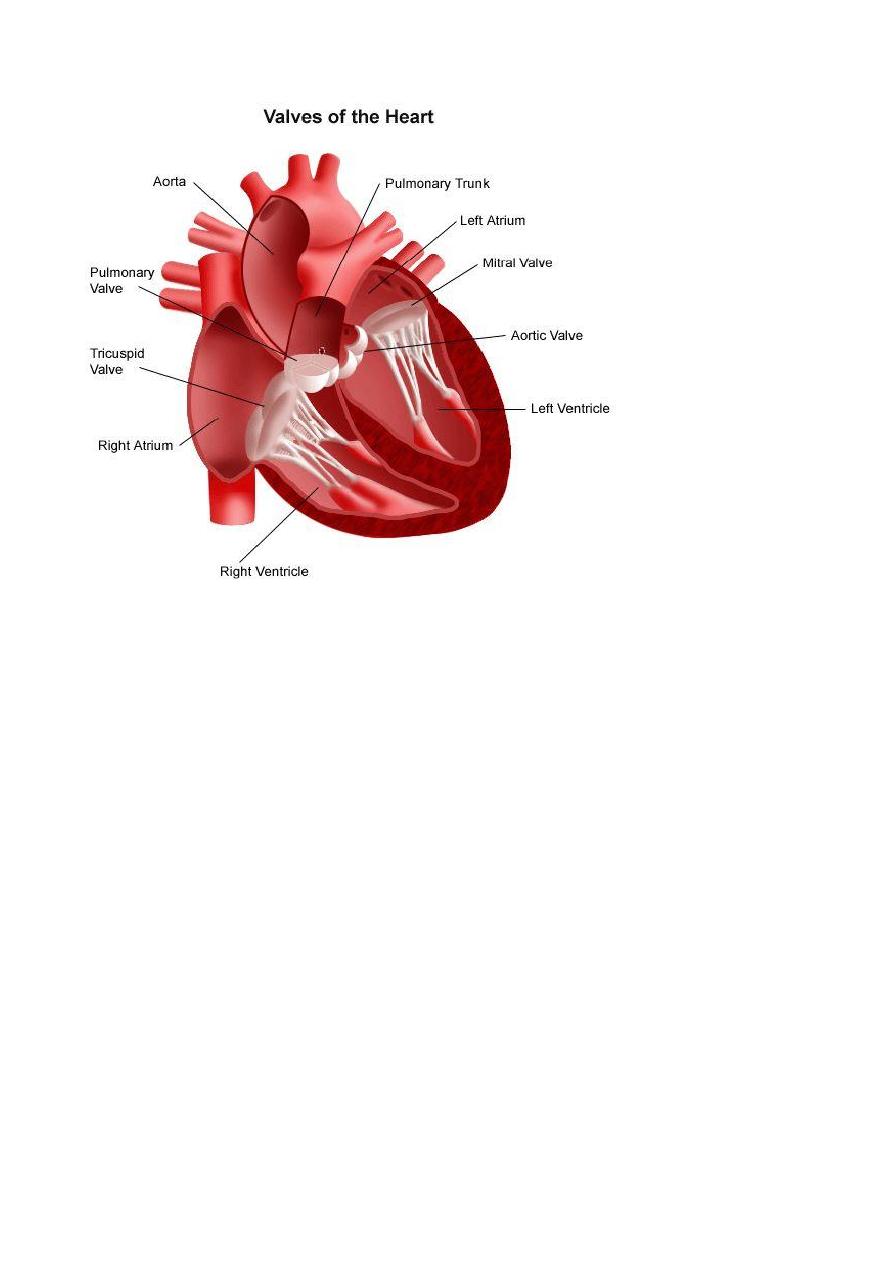
Mitral and aortic valves diseases are more common than lesions of tricuspid
and pulmonic valves.
Rheumatic fever and heart diseases:
Rheumatic fever: is an acute, immunologically mediated, multi-system
inflammatory disease that follows, after a few weeks and episodes of group
A streptococcal pharyngitis.
Rheumatic fever may cause heart disease during:
1- Acute phase (acute rheumatic carditis).
2- Chronic valvular deformities which's become manifested after many years
of acute disease.
Rheumatic fever occur in only about 3/1 of patients with group A
streptococcal pharyngitis.
Pathogenesis:-
Acute rheumatic fever is a hypersensitivity reaction induced by group A
streptococci, the antibodies directed against the M proteins of certain strains
of streptococci cross react with tissue glycoproteins in the heart, joints and
other tissues, the onset of symptoms 2 to 3 weeks after infection and the
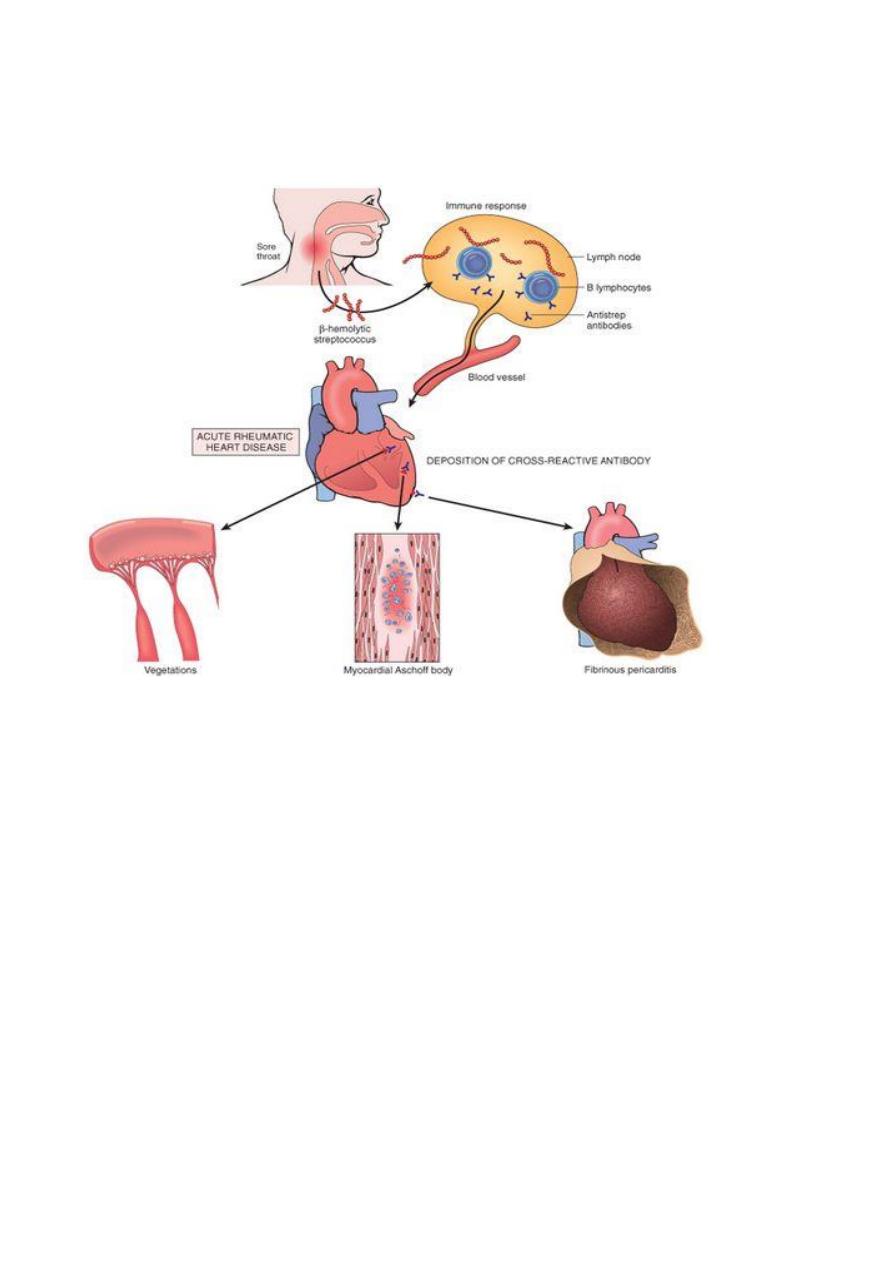
absence of streptococci from the lesions support the concept that R.F result
from immune response against the bacteria.
Morphology:
-
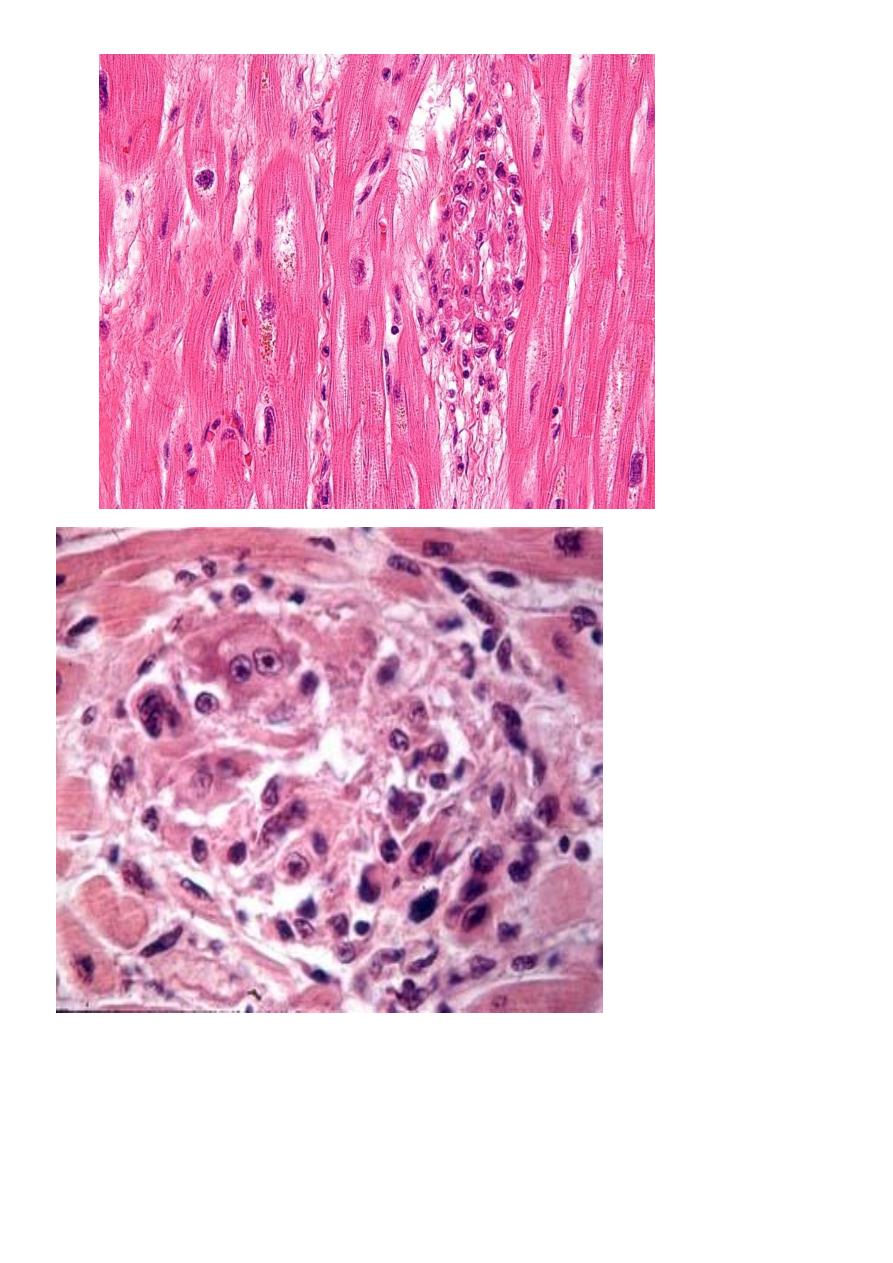
Acute rheumatic carditis is characterized by inflammatory changes in all 3
layers of the heart, so it's designated a pancarditis, it's characterized by
multiple foci of inflammation within connective tissue of the heart called
Aschoff bodies: a granuloma which contains a central focus of fibrinoid
necrosis, surrounded by a chronic mononuclear inflammatory cells and some
large histeocytes with prominent nucleoli in myocardium in addition to
presence of Aschoff bodies, there are diffuse interstitial inflammatory
infiltrates and in severe myocarditis may cause generalized dilation of cardiac
chambers.
In endocardium involvement is common and usually affect any valve but
mitral and aortic valves are common.
The valve is edematous, thickened and show foci of fibrinoid necrosis but
Aschoff nodules are not common.
The acute inflammation of valve predispose to the formation of small
vegetation seen as wart-like projections particularly along the lines of valves
closure, these acute changes may resolve without squeals or progress to
chronic scarring and valvular deformities.
Chronic rheumatic heart disease is characterized by irreversible deformity of
one or more cardiac valves, scarring of the valve leaflets may cause:-
1- Reduction in the diameters of valve orifice (stenosis).
2- Prevent proper closure of valve leaflets resulting in regurgitation of blood
during diastole.
3- Both stenosis and regurgitation.
Complications of rheumatic heart diseases:
1- Valvular stenosis and regurgitation increase the demands on the
myocardium because of increase pressure load or volume load or both and
cause heart failure.
2- Damage to the valves predispose to infective endocaridtis.
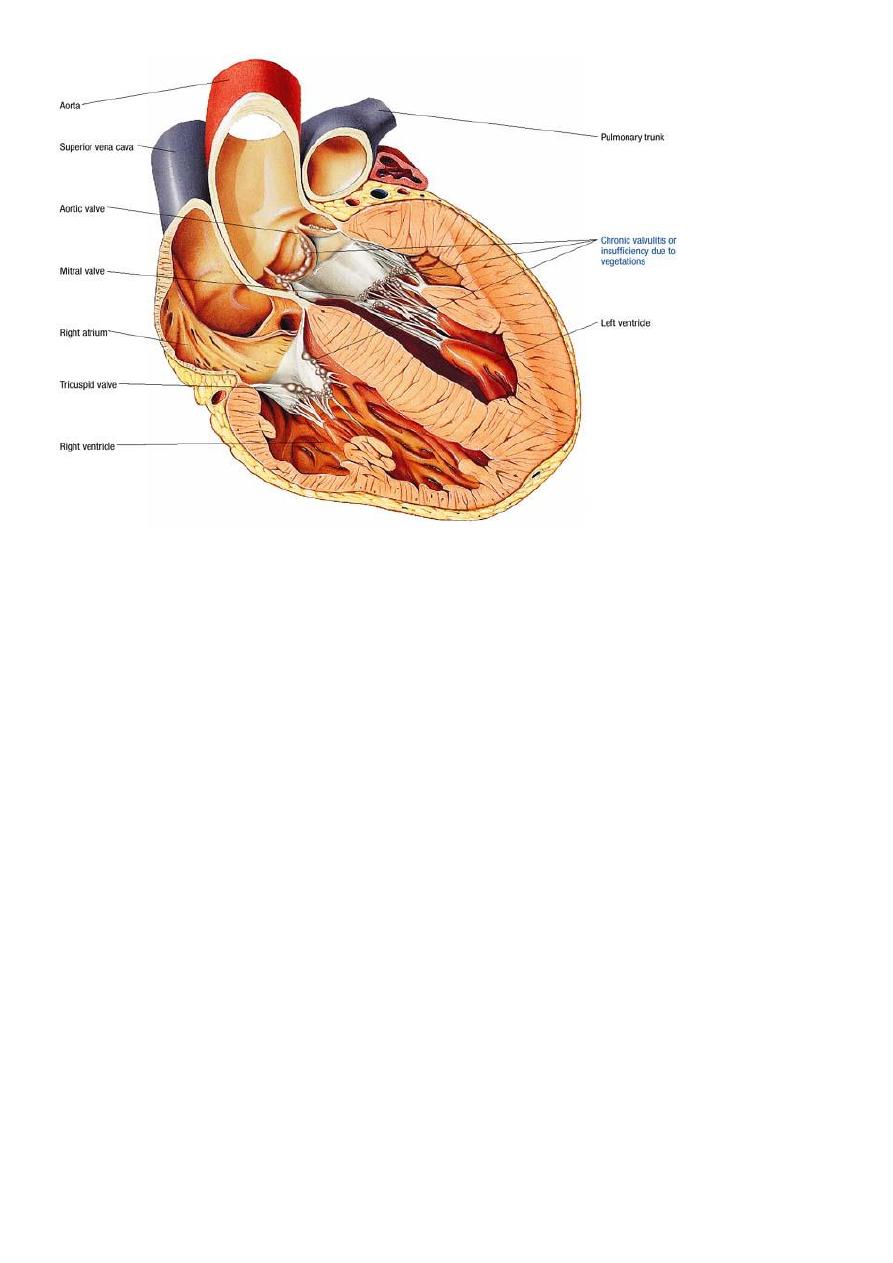
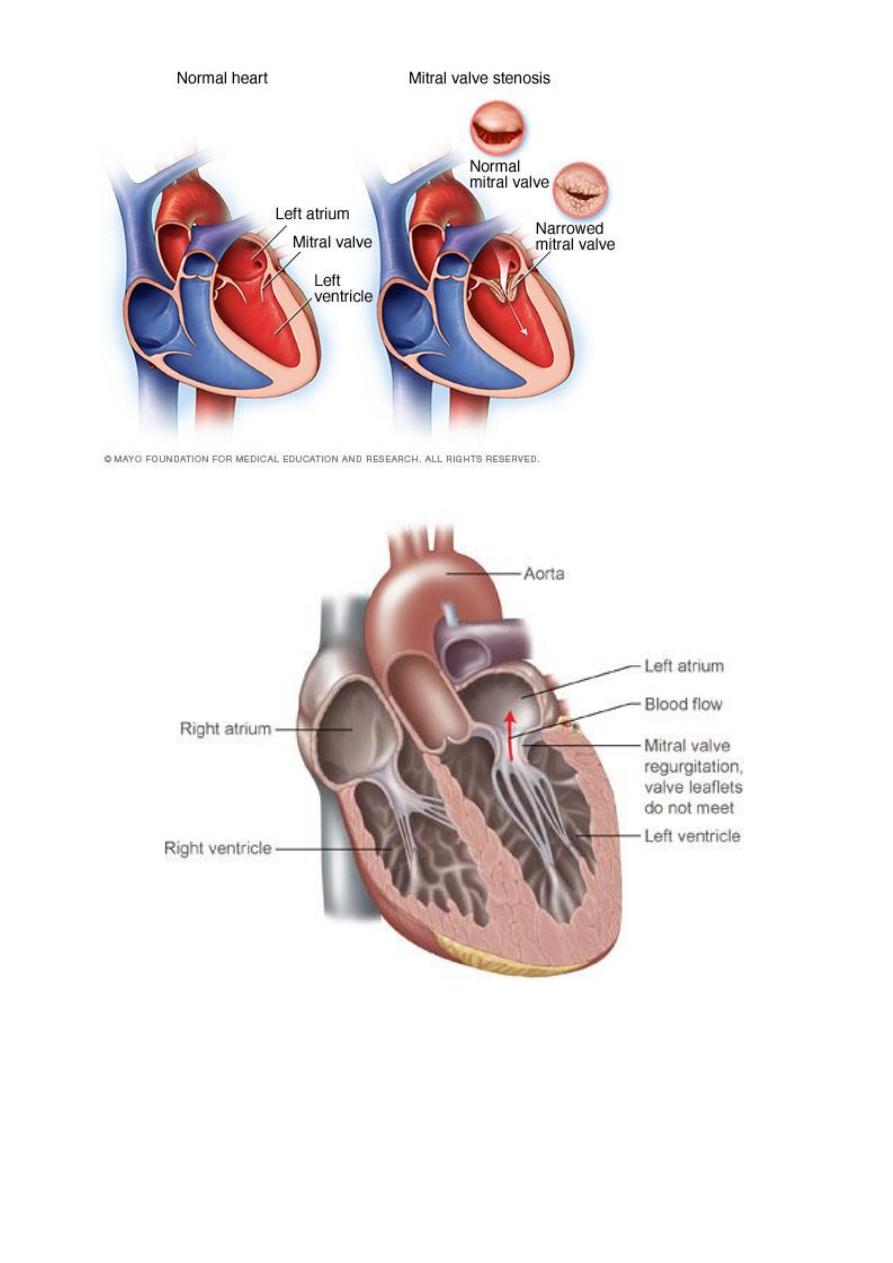
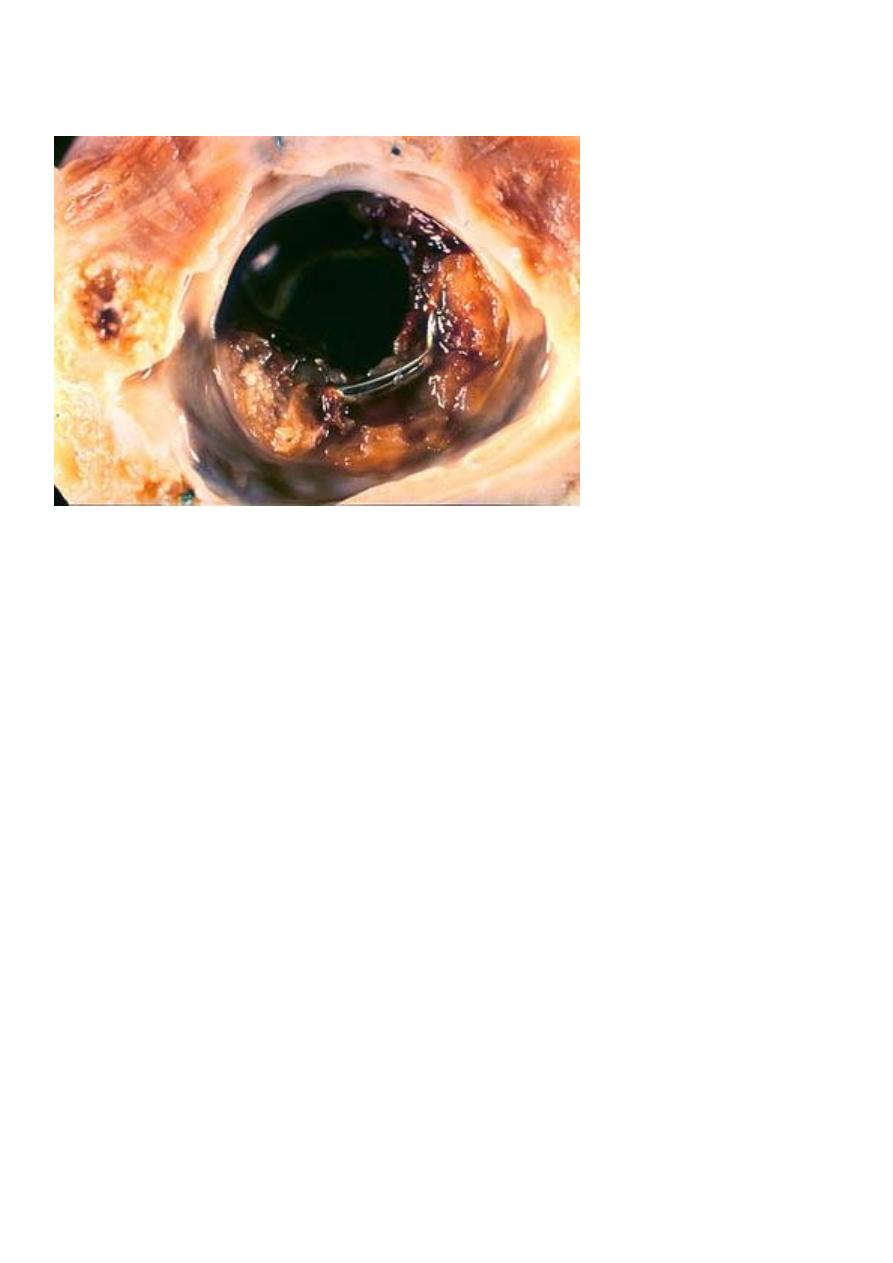
Chronic rheumatic mitral valvulitis:-
Stenosis is more than regurgitation and is most common cause of mitral
stenosis, the valve leaflets and chordae tendineae are thick, rigid and
interadherent and orifice narrowed to a slit-like channel, have a" fish-mouth
deformity", the left atrium is dilated and hypertrophied, mural thrombi may
be present which's source of systemic emboli.
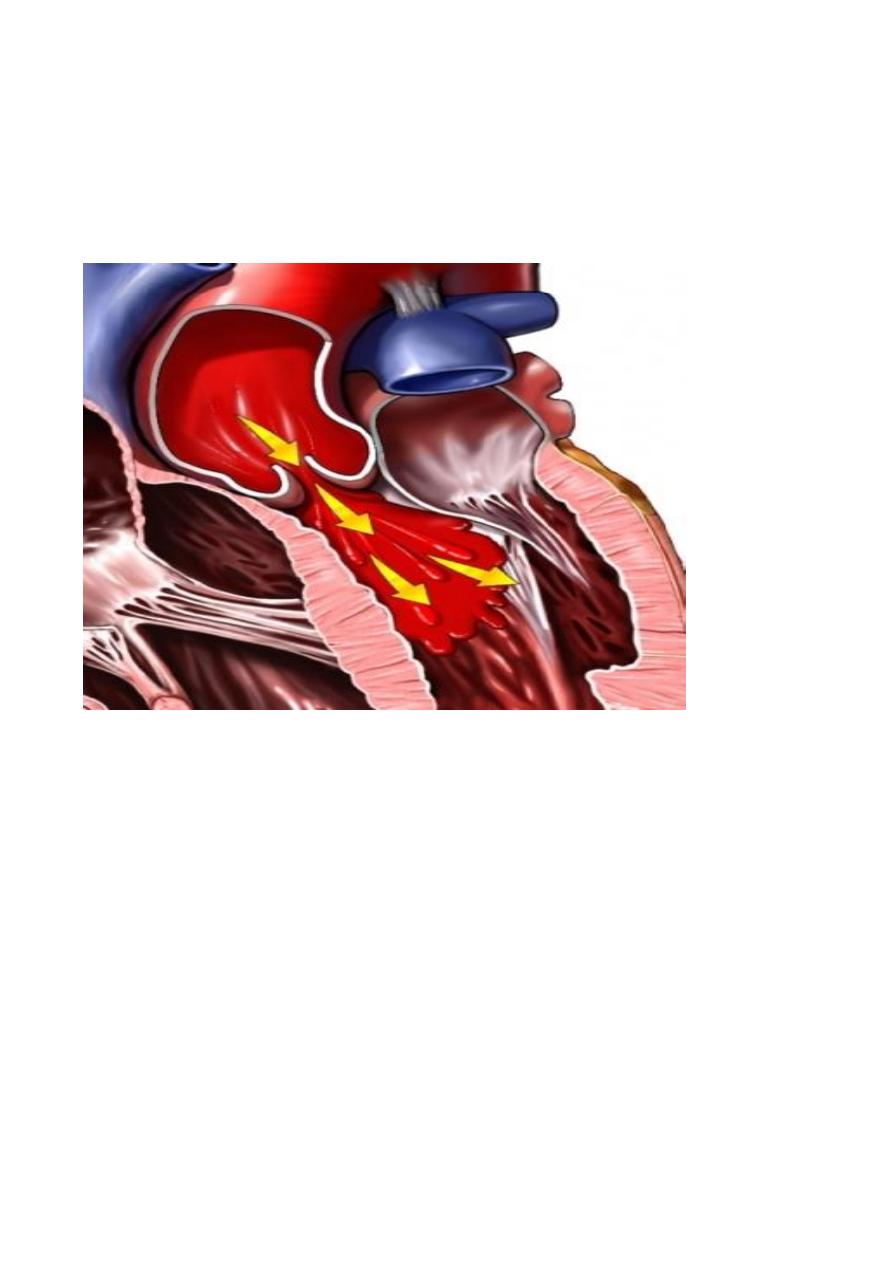
In mitral regurgitation, the deformed mitral leaflets are retracted and the
added volume load on the left ventricle causes left ventricular dilation and
hypertrophy.
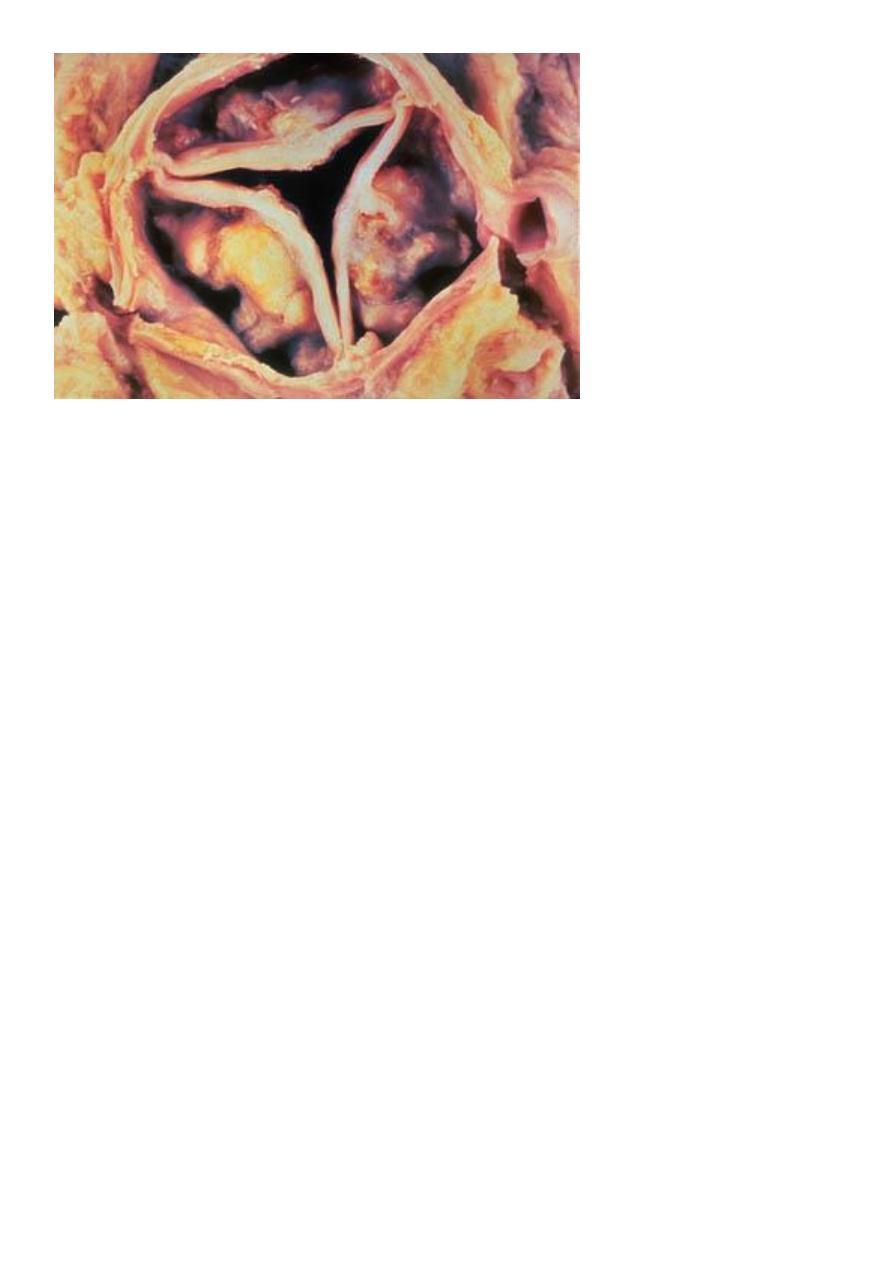
Chronic aortic valvulitis:-
The valve cusps are thickened, firm and adherent to each other, the orifice
reduced to a rigid, triangular channel.
Aortic stenosis places a pressure load on the left ventricle, so undergoes
concentric hypertrophy, fibrosis of the valve leaflets may also cause them to
retract toward the aortic wall result in aortic regurgitation.
Calcific aortic stenosis:-
This occur due to aging process by degenerative changes with fibrosis of
valve leaflets and calcification, so it's called degenerative calcific aortic
stenosis
(DCAS).
Infective endocarditis:-
It's infection of the cardiac valves or mural surface of the endocardium
resulting in the formation of an adherent mass of thrombotic debris and
organism (vegetation).
Infective endocarditis divided into:-
1- Acute endocarditis:-
associated with infection of the valves by high virulent
microorganism as staphylococcus aureus on normal valve and cause rapidly
progressive infection with few local host reaction.
2- Subacute endocarditis:-
associated with infection of previously abnormal
valves by low virulent organisms, such as ά-hemolytic streptococci, the
infection tend to progress slowely and accompanied by the development of a
local inflammatory reaction and granulation tissue in the affected valve.
Pathogenesis:-
Infection occur from any microorganism as bacteria, fungi and parasite but
bacteria is the most causative agents, this bacteria found in blood (bacteremia)
then implanted on the endocardial surface, the source of bacteremia usually by
intravenous drug abusers, previous dental, surgical or other procedure.
The most common abnormalities of valve predispose to infective endocarditis
are prosthetic valve, chronic rheumatic heart disease, DACS and mitral valve
prolapse.
Infective endocarditis is a particularly difficult infection to eradicate because
of the avascular nature of the heart valves, the inflammatory response to the
infection is relatively scant, so that even a virulent organism can proliferate in
uncontrolled fashion.
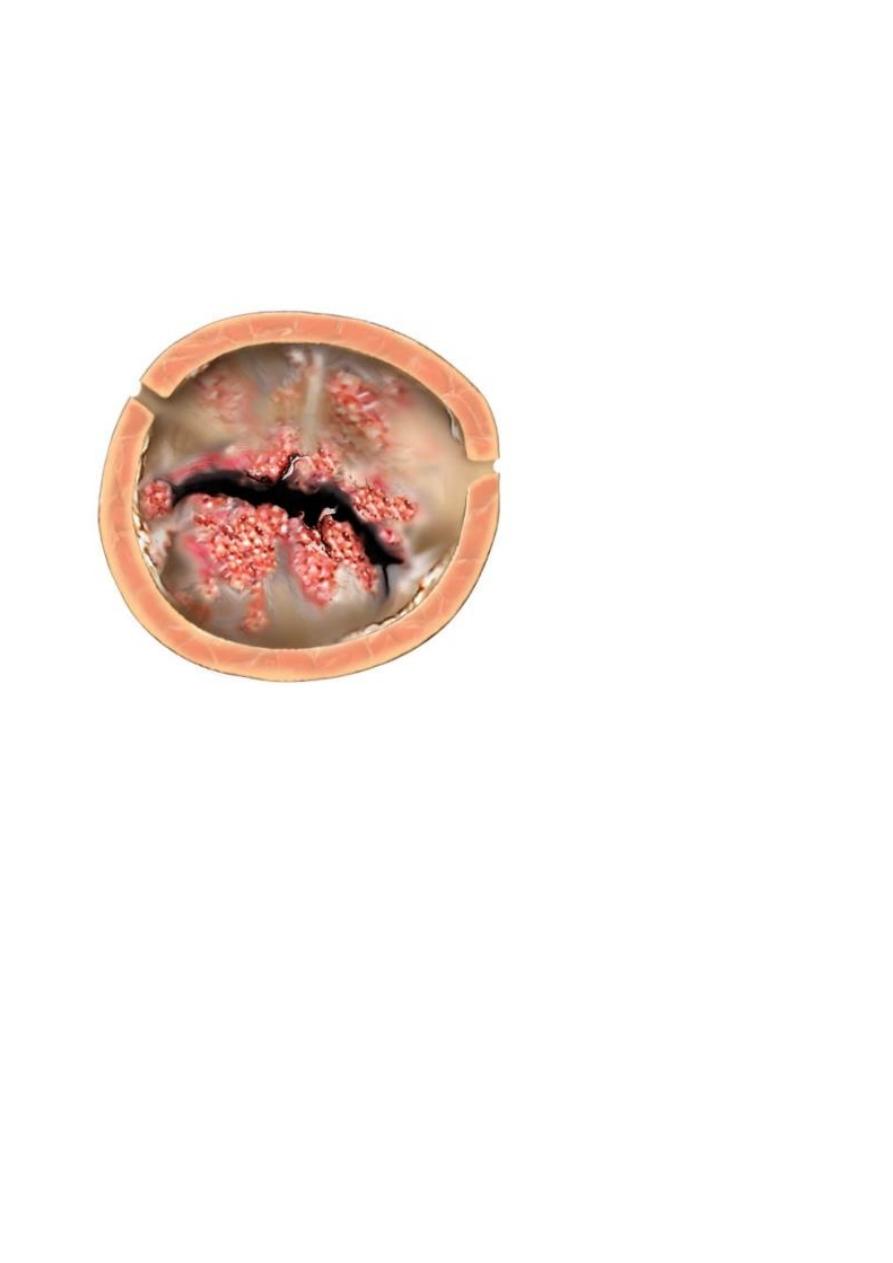
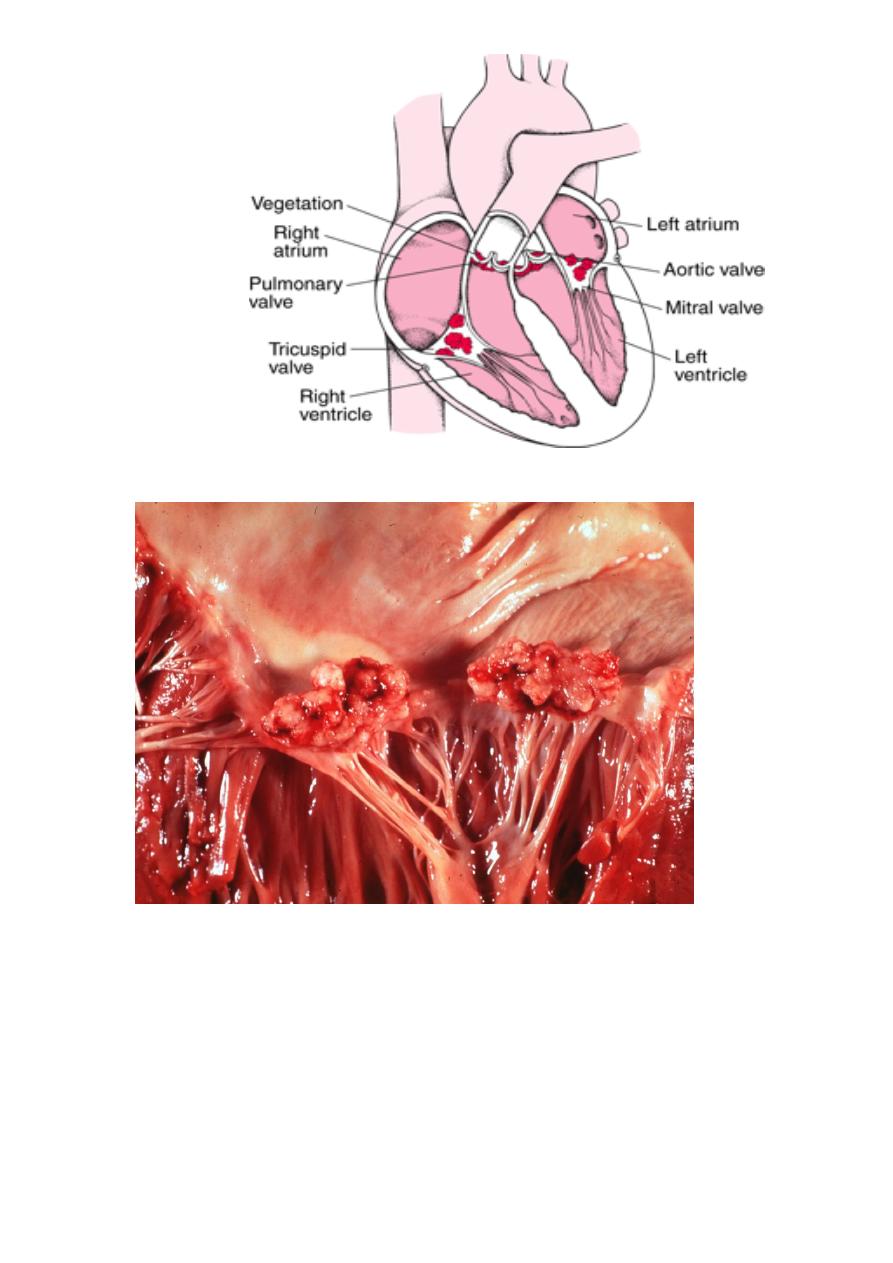
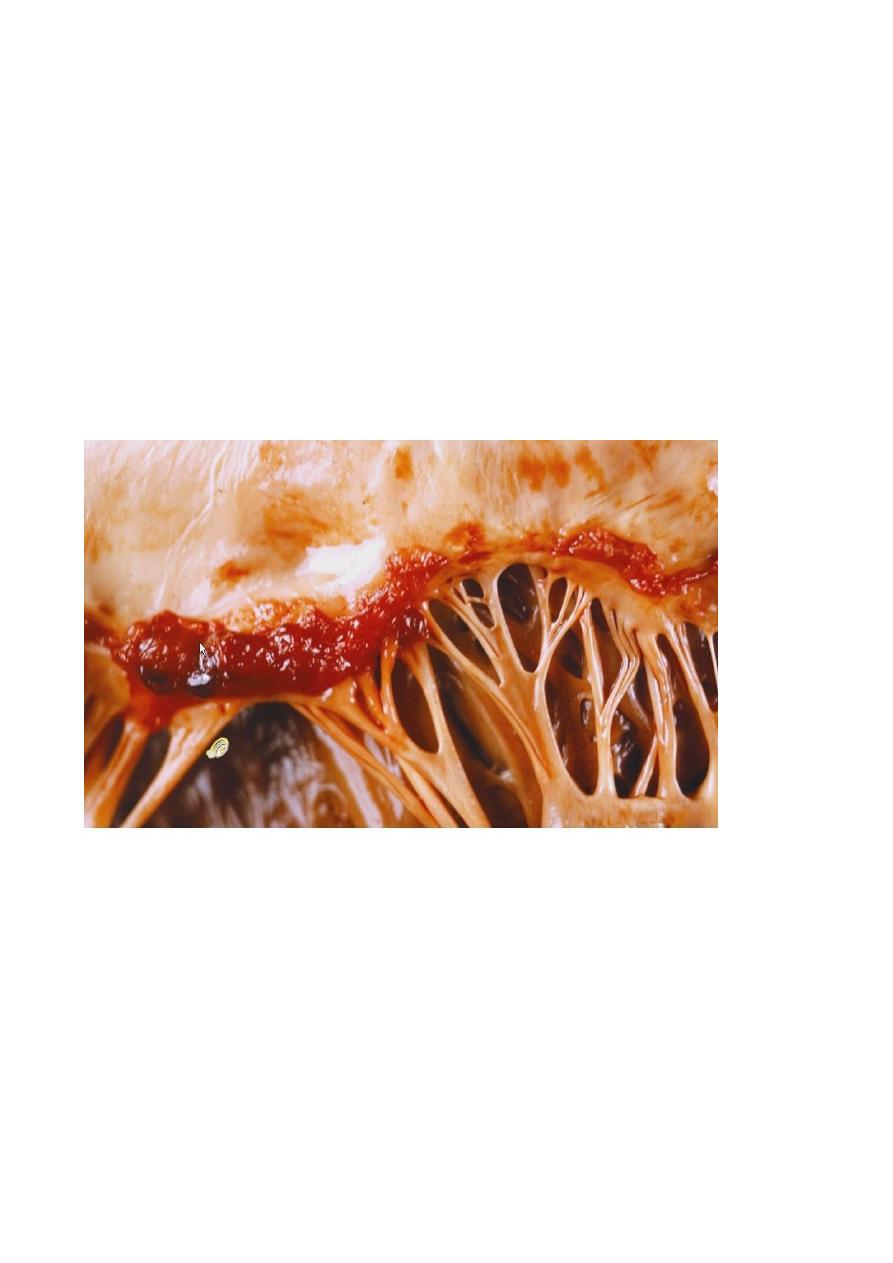
Morphology:-
The hall mark of infective endocarditis is the presence of valvular vegetation
containing bacteria or other organisms, the aortic and mitral valves are the
most common sites of infection, the vegetation may be single or multiple and
may be involve more than one valve, seen grossly as small excrescence and
vegetation enlarge to form bulky, friable lesion obstruct valve orifice
Microscopically
: show large numbers of organisms admixed with fibrin and
blood cells.
Systemic emboli may occur due to friable nature of the vegetation sites, and
abscesses usually develop at the sites of such infarcts because of embolic
fragments contain large number of virulent organism.
Non bacterial thrombotic endocarditis:
Is characterized by deposition of small masses of fibrin, platelets and other
blood components, on the leaflets of cardiac valves, these valvular lesions are
sterile and do not contain microorganism.
Pathogenesis:-
Endothelial abnormalities and hyper-coagulable states predispose to its
development, this hypercoagulability occur in deep venous thrombosis,
malignancies and even occur in healthy individuals.
Morphology:-
It's appear as group of small nodules on the lined of valve closure and may
become large and friable.