
1
The Blood Flukes or Schistosomes
Adult male and Female of Schistosoma Anterior portion of Male
Morphology, Biology and Life Cycle.
The adult males measure 12 to 20 mm in length by about 0.5 mm in greatest
breadth. Females are much more delicate, with a length of about 15 to 30 mm and
a breadth of 0.1 to 0.3 mm. Eggs discharged in the stool are usually rotund,
measure 70 to 100 microns by 50 to 65 microns, and each contains a ciliated
miracidium.
The earliest habitat of the young adult S. japonicum is the tributaries of the
superior mesenteric vein adjacent to the small intestine. Later, some worms
migrate into the inferior mesenteric vein, or even into the caval system. In these
locations, female continue to lay eggs daily over a period of years.
2
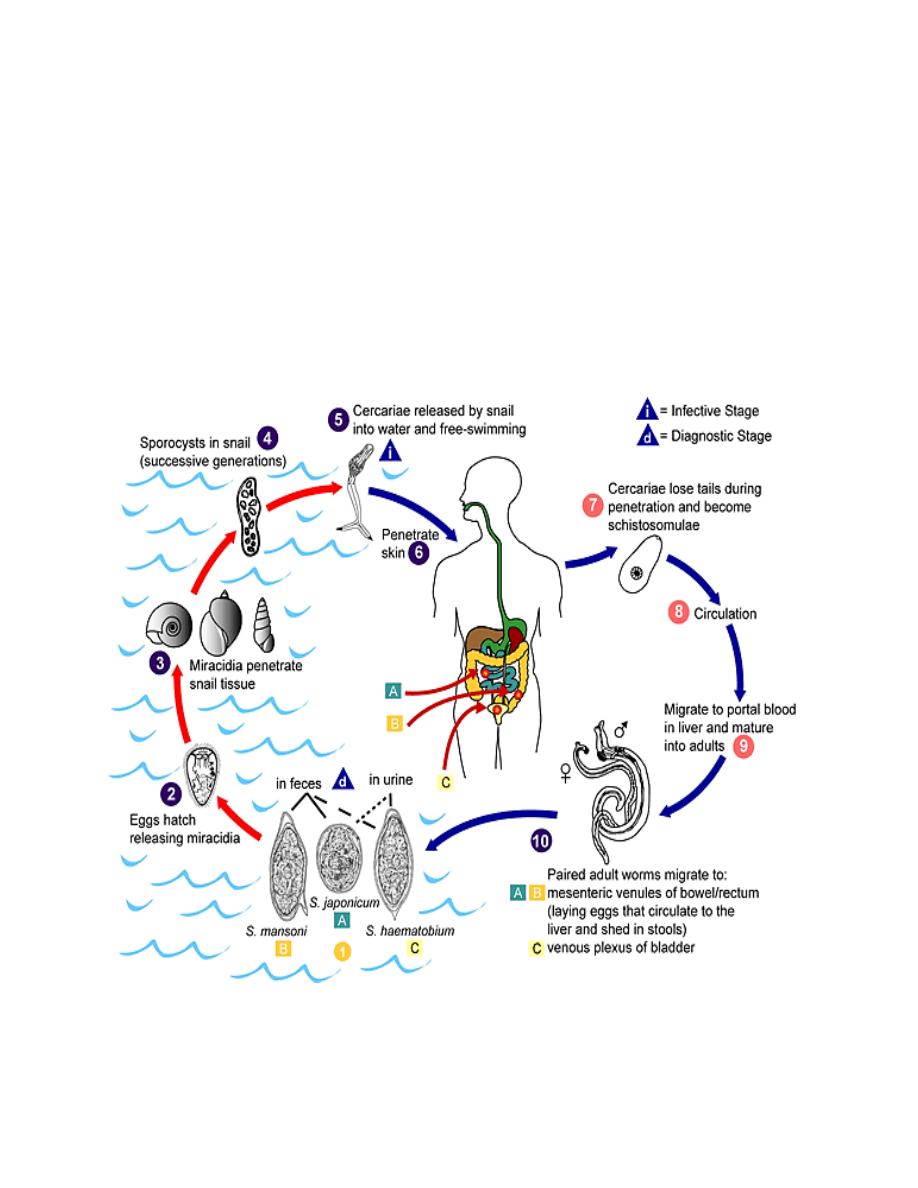
Fully embryonated viable eggs of S. japonicum soon hatch in fresh water and the
miracidia attack and enter tissues of species of small operculate snails, genus
Oncomelania (Schistosoma japonicum) genus Biomphalaria (S. mansoni), and
genus Bulinus (S. haematobium). After approximately 4 weeks of development in
an appropriate snail, the intra-mollouskan phase is completed and cercariae begin
to emerge into the water; during dry weather they remain within the snail. On
contrast, the cercariae become attached to the skin of man, penetrate into cutaneous
capillaries and begin their blood migration. Approximately 4 to 5 week later they
have matured in the smaller branches of the superior mesenteric vein and egg-lying
begins.

3
Pathogenesis and Symptomatology.
Schistosoma haematobium
The prepatent incubation period in schistosomiasis haematobia parallels that of the
two intestinal types of the disease, but there is usually less evidence of acute
hepatitis and systemic intoxication.
Egg deposition and extrusion cause local traumatic damage and hemorrhage, either
in the wall of the rectum or the urinary bladder.
Vesical lesions include hyperplasia of the wall, then gritty phosphatic deposits on
the structure and dense fibrosis of the muscular and submucous coats, through
which it is increasingly difficult for eggs to filter. Meanwhile the urethral lumen
becomes greatly constricted, at times completely closed, similarily the ureters and
pelves of the kidneys, the penis or scrotum may develop obstruction. In women the
vulvae are frequently hyperplastic and indurated. Advanced cases of vesical
schistosomiasis often have septic involvement.
During the biologic incubation period, the patient may be essentially symptomless
or he may have an increasing malaise with late afternoon fever, moderate hepatic
pain or epigasrtic distress, and an elevated eosinophil count. If worms matrure in
the rectal veins there may be severe tenesmus with dysentry. More often the first
evidence of the infection is the painless passage of blood at the end of the period of
micturition, but more and more there is also discharge of pus cells and necrotic
tissue debris, decrease in the interval between periods of urination and eventual
incontinence, or anuria due to urethral stricture. Bladder colic is a
fundamental
symptom.

4
Diagnosis
Schistosoma japonicum
During the biologic incubation period, specific diagnosis
is not possible. With development of the acute stage eggs
can usually be recovered in bloody mucus in the stool,
although sedimentation or acid-ether concentration
technics may be required to discover the eggs. In chronic
cases rectal biopsy will often supply demonstration of
eggs when they are not found in the stools.
Schistosoma mansoni
This is usually made on demonstration of characteristic
eggs of S.mansoni, with their distinct lateral spine,
evacuated in the stool. Likewise, rectal biopsy is a
particularly fruitful procedure. Intradermal and
complement-fixation
reactions
with
schistosome
antigen are at times more valuable.
Schistosoma haematobium
This is accomplished by recovery of characteristic eggs
in the sediment which settles out of the urine in a
sedimentation
flask
or
similar
container.
Immunological tests may be valuable, especially in
epidemiological surveys. Bladder biopsy may be useful
in demonstrating the eggs.

5
Treatment
The drug of choice for treating all species of schistosomes is praziquantel. Cure
rates of 65-90% have been described after a single treatment with praziquantel. In
individuals not cured, the drug causes egg excretion to be reduced by 90%.
Epidemiology
Man is the only important definitive host of S. haematobium. The eggs of this
worm are commonly extruded from the wall of the urinary bladder and excreted in
the urine. Promiscuous urination into bodies of fresh water including ponds and
irrigation canals, primitive latrines situated over small rivers or small village
streams all provide infection for the snail hosts, Bulinus truncates and related
species.