1
Joints of upper limb
1
st
stage
Dr.Kalid Ali Zayer
Elbow joint
Contents
1 Structures of the Elbow Joint
o
1.1 Articulating Surfaces
o
1.2 Joint Capsule and Bursae
o
1.3 Ligaments
2 Neurovasculature
3 Movements of the Joint
The elbow is the joint connecting the upper arm to the forearm. It classed as a
hingetype synovial joint.
Structures of the Elbow Joint
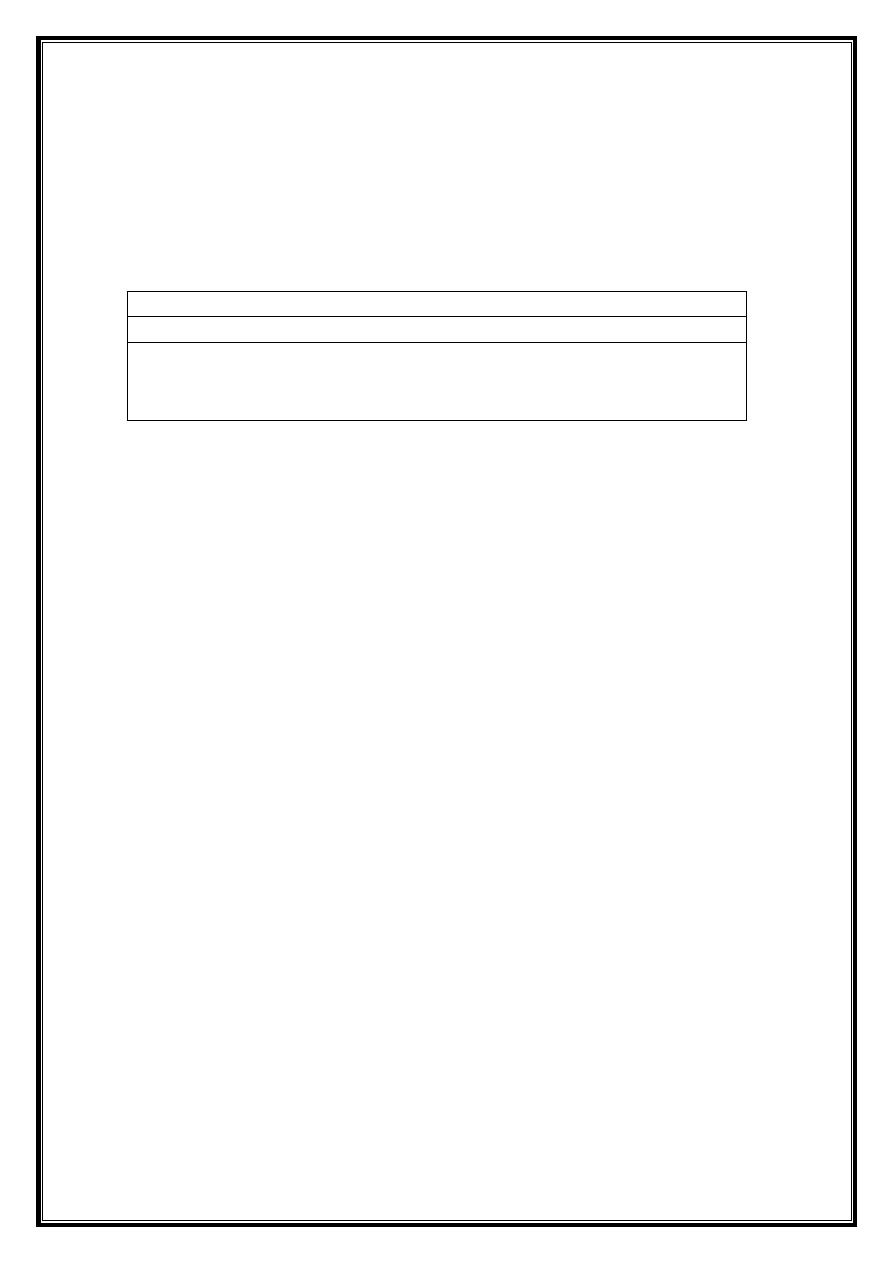
Articulating Surfaces
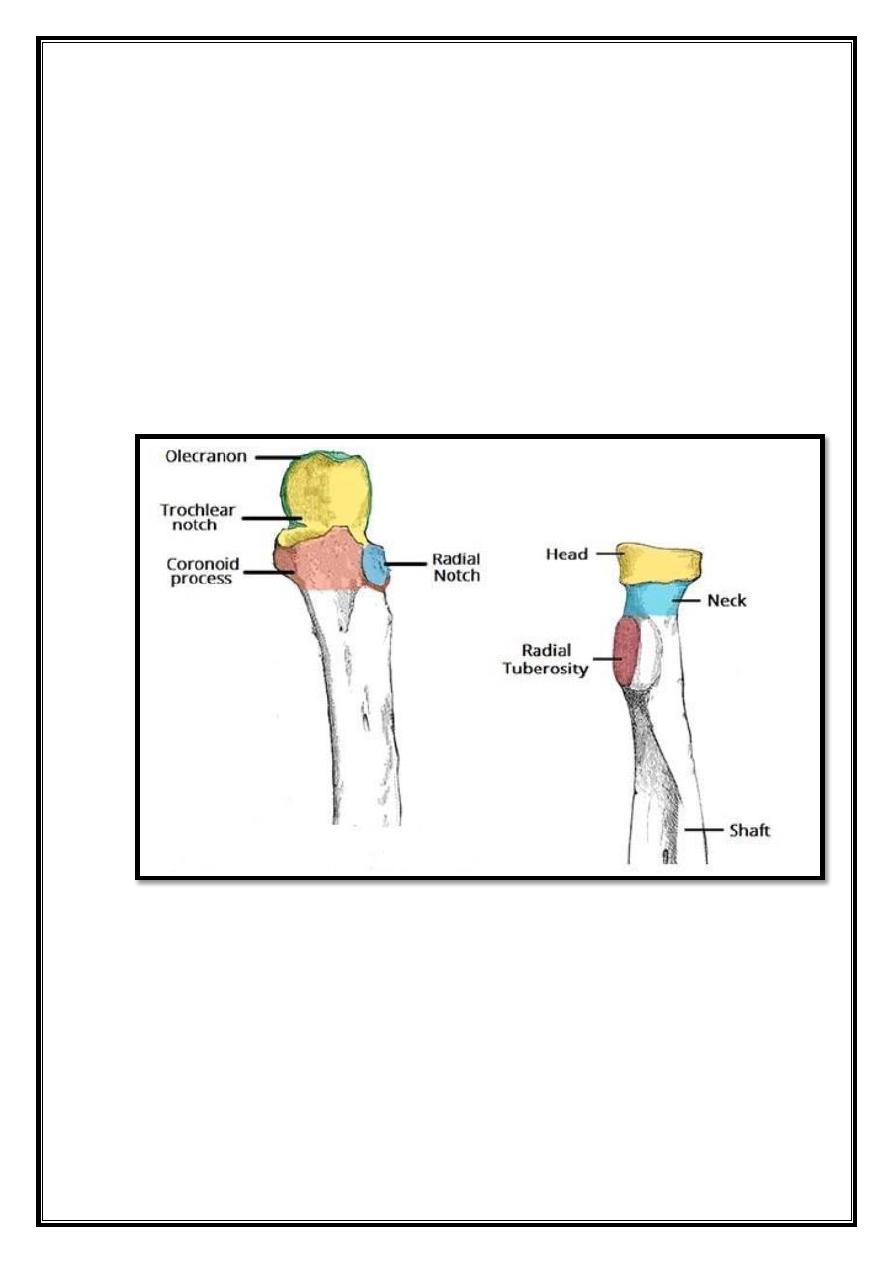
It consists of two separate articulations:
Trochlear notch of the ulna and the trochlea of the humerus
Head of the radius and the capitulum of the humerus
Note: The proximal radioulnar joint found within same joint capsule of the
elbow, but most resources consider it as a separate articulation.
2
Fig 9 – Anterior and posterior views of the articulations of the elbow
joint
Joint Capsule and Bursae
Like all synovial joints, the elbow joint has a capsule enclosing the joint. This in
itself is strong and fibrous, strengthening the joint. The joint capsule thickened
medially and laterally to form collateral ligaments, which stabilize the flexing and
extending motion of the arm.
A bursa is a membranous sac filled with synovial fluid. It acts as a cushion to
reduce friction between the moving parts of a joint, limiting degenerative damage.
There are many bursae in the elbow, but only a few have clinical importance:
Intratendinous
– located within the tendon of the triceps brachii.
Subtendinous
– between the olecranon and the tendon of the triceps brachii,
reducing friction between the two structures during extension and flexion of the
arm.
3
Subcutaneous (olecranon) bursa
– between the olecranon and the overlying
connective tissue (implicated in olecranon bursitis).
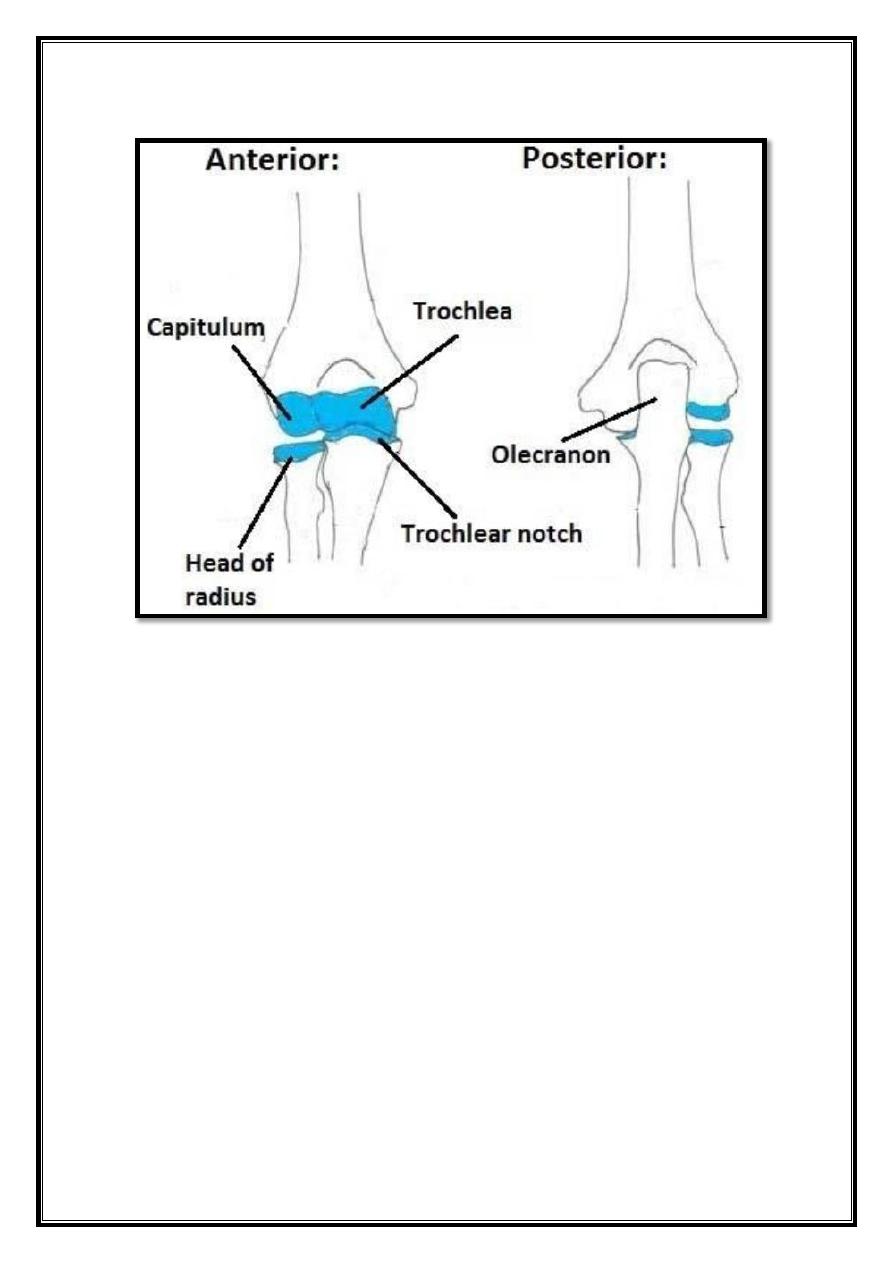
Ligaments
- Ligaments strengthen the joint capsule of the elbow
medially and laterally.
The radial collateral ligament found on the lateral side of the joint,
extending from the lateral epicondyle, and blending with the annular
ligament of the radius (a ligament from the proximal radioulnar joint).
The ulnar collateral ligament originates from the medial epicondyle,
and attaches to the coronoid process and olecranon of the ulna.
Fig 10 – Ligaments of the elbow joint.
Neurovasculature
The arterial supply to the elbow joint is from the cubital anastomosis, which
includes recurrent and collateral branches from the brachial and deep brachial
arteries.
Its nerve supply is provided by the median, musculocutaneous and radial nerves
anteriorly, and the ulnar nerve posteriorly.
4
Movements of the Joint
The orientation of the bones forming the elbow joint produces a hinge type
synovial joint, which allows for extension and flexion of the forearm:
Extension: Triceps brachii and anconeus
Flexion: Brachialis, biceps brachii, brachioradialis
Note – pronation and supination do not occur at the elbow – they are produced at
the nearby radioulnar joints.
Radioulnar joints
Contents
1 Proximal Radioulnar Joint
2 Distal Radioulnar Joint
3 Interosseous Membrane
The radioulnar joints are two locations in which the radius and ulna
articulate in the forearm:
Proximal radioulnar joint: This is located near the elbow, and
is an articulation between the head of the radius, and the radial
notch of the ulna.
Distal radioulnar joint: This is located near the wrist, and is an
articulation between the ulnar notch of the radius, and the ulnar
head.
Both of these joints classified as pivot joints, responsible for pronation
and supination of the forearm.
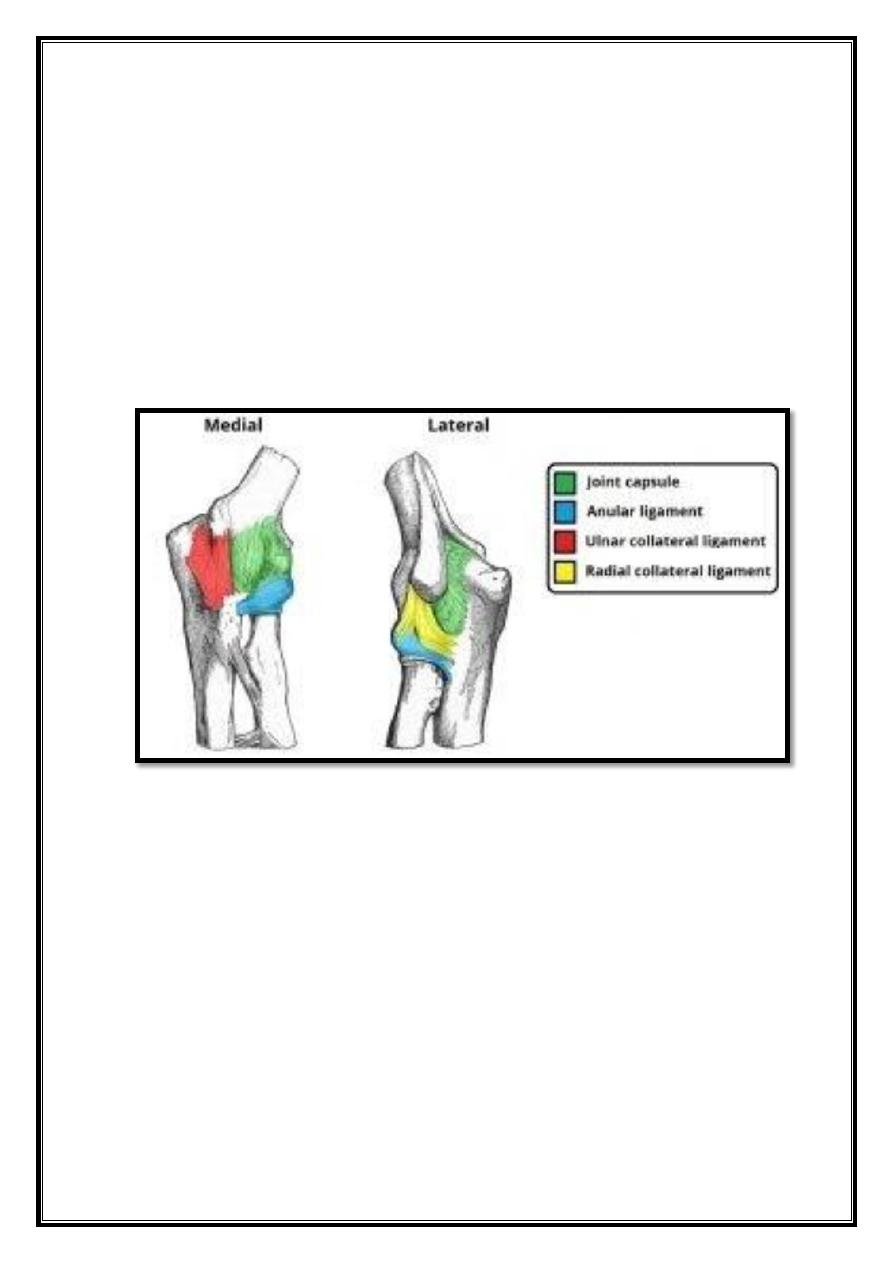
Fig 11 – The proximal radioulnar joint, with the annular ligament.
5
Proximal Radioulnar Joint
The proximal radioulnar joint is located immediately distal to the elbow joint,
and enclosed within the same articular capsule. It formed by an articulation
between the head of the radius and the radial notch of the ulna.
The radial head held in place by the annular radial ligament, which forms a
‘collar’ around the joint. The annular radial ligament lined with a synovial
membrane, reducing friction during movement.
The head of the radius rotating within the annular ligament produce movement.
There are two movements possible at this joint; pronation and supination.
Pronation: Produced by the pronator quadratus and pronator teres.
Supination: Produced by the supinator and biceps brachii.
Fig 12 – Articulating surfaces of the proximal radioulnar joint.
6
Distal Radioulnar Joint
This distal radioulnar joint is located just proximally to the wrist joint. It is an
articulation between the ulnar notch of the radius, and the ulnar head.
In addition to anterior and posterior ligaments strengthening the joint, there is
also a fibrocartilaginous ligament present, called the articular disk. It serves two
functions:
Binds the radius and ulna together, and holds them together during movement
at the joint.
Separates the distal radioulnar joint from the wrist joint.
Like the proximal radioulnar joint, this is a pivot joint, allowing for pronation
and supination.
The ulnar notch of the radius slides anteriorly over the head of the ulnar during
such movements.
Pronation: Produced by the pronator quadratus and pronator teres
Supination: Produced by the supinator and biceps brachii
Fig 13 – Articular surfaces of the distal radioulnar and wrist joints.
7
Interosseous Membrane
The interosseous membrane is a sheet of connective tissue that joins the radius
and ulna together between the radioulnar joints.
It spans the distance between the medial radial border, and the lateral ulnar
border. There are small holes in the sheet, as a conduit for the forearm
vasculature. This connective tissue sheet has three major functions:
Holds the radius and ulna together during pronation and supination of the
forearm, providing addition stability.
Acts as a site of attachment for muscles in the anterior and posterior
compartments of the forearm.
Transfers forces from the radius to the ulna.
Wrist joint
Contents
1 Structures of the Wrist Joint
o
1.1 Articulating Surfaces
o
1.2 Joint Capsule
o
1.3 Ligaments
o
1.4 Neurovascular Supply
2 Movements of the Wrist Joint
The wrist joint (also known as the radiocarpal joint) is a synovial joint in the
upper limb, marking the area of transition between the forearm and the hand.
Structures of the Wrist Joint
Articulating Surfaces
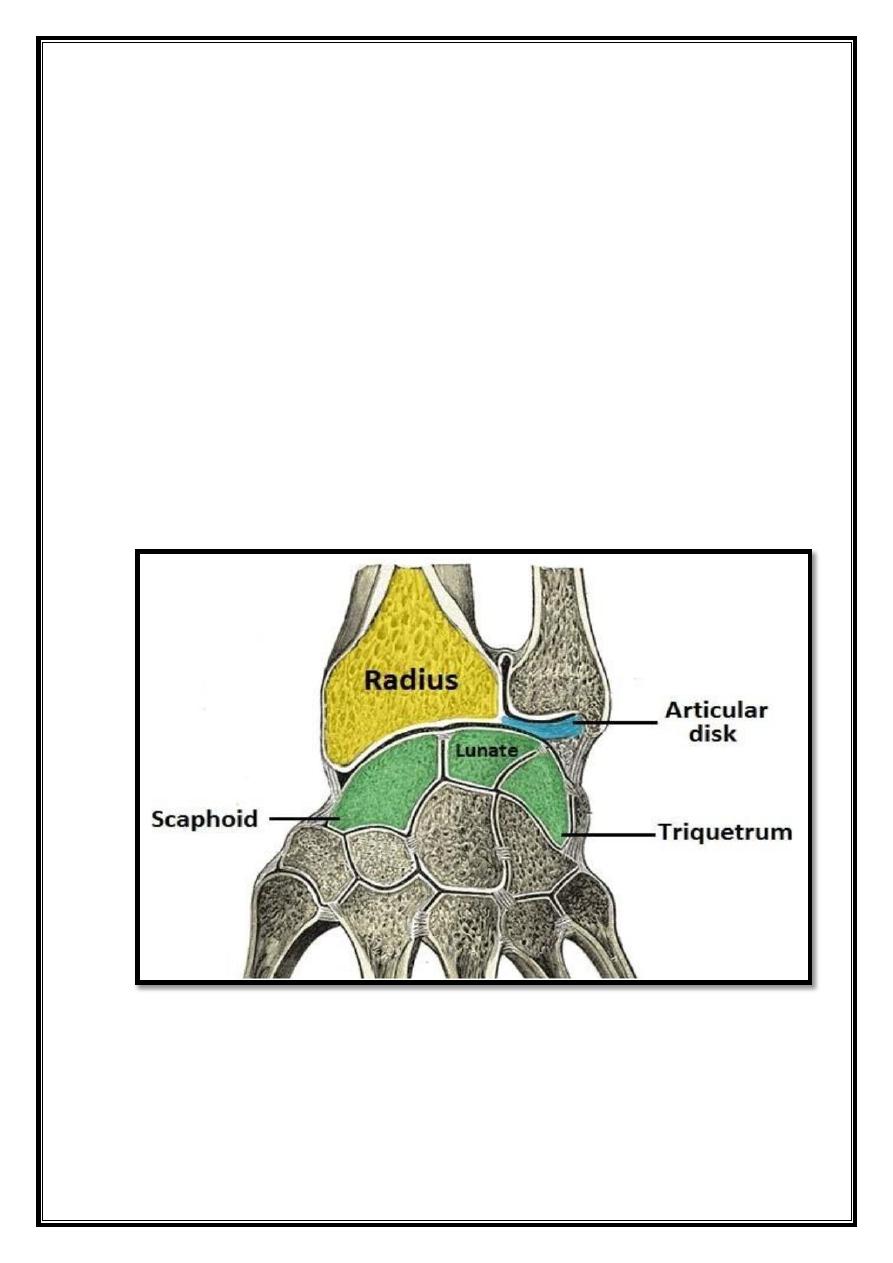
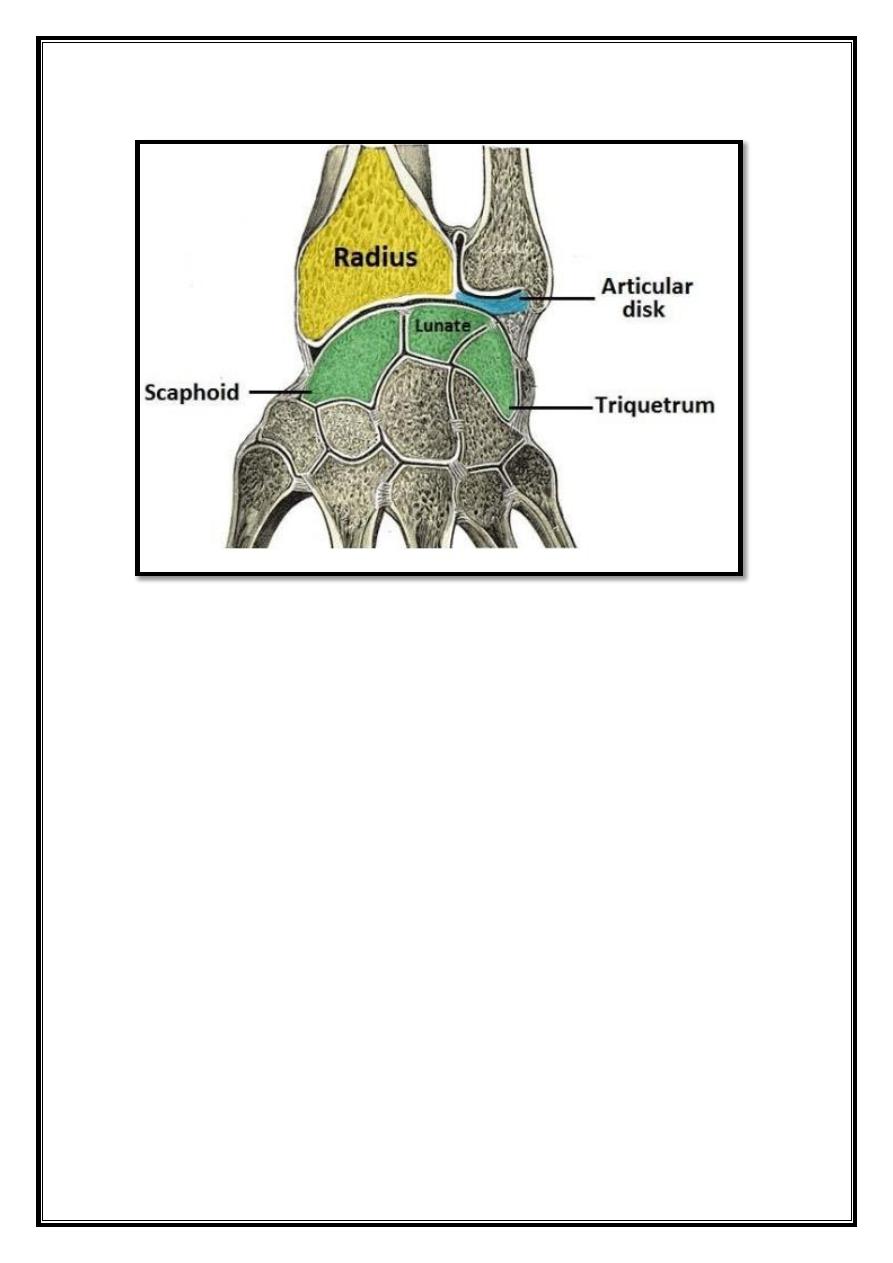
The wrist joint formed by:
Distally – The proximal row of the carpal bones (except the pisiform).
Proximally – The distal end of the radius, and the articular disk (see below).
The ulna is not part of the wrist joint – it articulates with the radius, just
proximal to the wrist joint, at the distal radioulnar joint. It prevented from
articulating with the carpal bones by a fibrocartilaginous ligament, called the
articular disk, which lies over the superior surface of the ulna. Together, the
carpal bones form a convex surface, which articulates with the concave surface
of the radius and articular disk.
8
Fig 14 – Articular surfaces of the wrist joint.
Joint Capsule
Like any synovial joint, the capsule is dual layered. The fibrous outer layer
attaches to the radius, ulna and the proximal row of the carpal bones. The internal
layer is comprised of a synovial membrane, secreting synovial fluid, which
lubricates the joint.
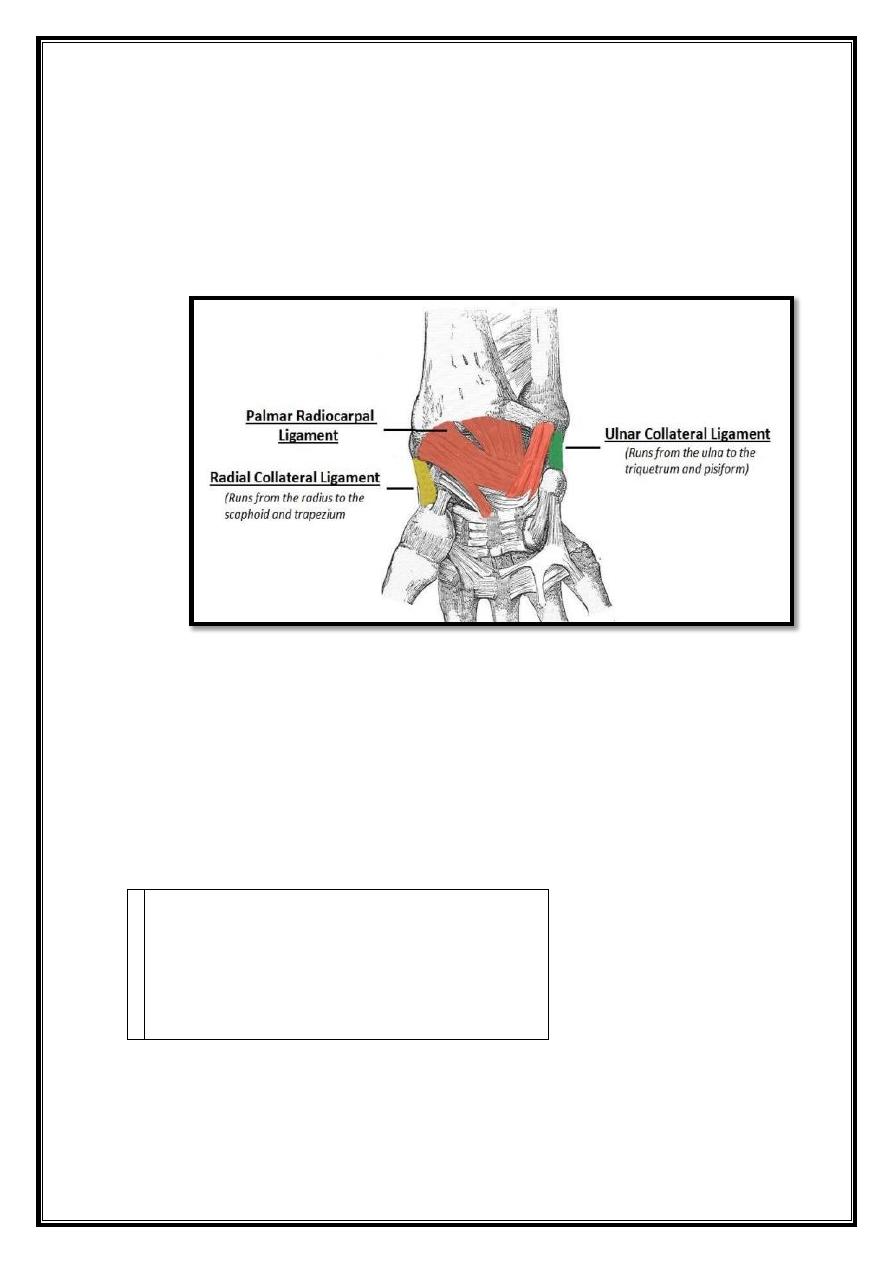
Ligaments
There are four ligaments of note in the wrist joint, one for each side of the joint
Palmar radiocarpal – It found on the palmar (anterior) side of the hand. It
passes from the radius to both rows of carpal bones. Its function, apart from
increasing stability, is to ensure that the hand follows the forearm during
supination.
Dorsal radiocarpal – It found on the dorsum (posterior) side of the hand. It
passes from the radius to both rows of carpal bones. It contributes to the stability
of the wrist, but also ensures that the hand follows the forearm during pronation.
9
Ulnar collateral – Runs from the ulnar styloid process to the triquetrum and
pisiform. Works in union with the other collateral ligament to prevent excessive
lateral joint displacement.
Radial collateral – Runs from the radial styloid process to the scaphoid and
trapezium. Works in union with the other collateral ligament to prevent excessive
lateral joint displacement.
Fig 15 – Palmar view of the ligaments of the wrist joint.
Neurovascular Supply
The wrist joint receives blood from branches of the dorsal and palmar carpal
arches, which are
derived from the ulnar and radial arteries (for more information, see Blood
Supply to the
Upper Limb). Branches of three nerves deliver innervation to the wrist:
Median nerve – Anterior interosseous
branch.
Radial nerve – Posterior interosseous
branch.
Ulnar nerve – deep and dorsal branches.
Movements of the Wrist Joint
The wrist is an ellipsoidal (condyloid) type synovial joint, allowing for movement
along two axes. This means that flexion, extension, adduction and abduction can
all occur at the wrist joint. The muscles of the forearm perform all the movements
of the wrist.
10
Flexion – Produced mainly by the flexor carpi ulnaris, flexor carpi radialis, with
assistance from the flexor digitorum superficialis.
Extension – Produced mainly by the extensor carpi radialis longus and brevis, and
extensor carpi ulnaris, with assistance from the extensor digitorum.
Adduction – Produced by the extensor carpi ulnaris and flexor carpi ulnaris
Abduction – Produced by the abductor pollicis longus, flexor carpi radialis,
extensor carpi radialis longus and brevis.
Hand
Contents
1 Joints in the Hand
2 Movements of the Hand
3 Fascia
The hand contains a complex range of structures, which permit a wide variety of
movements,
many of which are essential for day-to-day tasks.
Joints in the Hand
Metacarpophalangeal Joint (MCPJ)
– More commonly known as the
knuckles, these are the condyloid joints comprised of the articulation between
metacarpal and proximal phalanx in each of the five digits.
Interphalangeal Joints
– These are the hinge joints between the phalanges and
there are two in each digit. The thumb is an exception, and has only one
interphalangeal joint. The two joints are the:
o
Proximal Interphalangeal Joints (PIPJ)
– The articulation between the
proximal phalanx and intermediate phalanx in each of the 2nd to 5th digits.
o Distal Interphalangeal Joints (DIPJ)
– The articulation between the
intermediate phalanx and distal phalanx in each of the 2nd to 5th digits.
Movements of the Hand
The hand is able to perform a vast range of movements, which highlighted below:
Flexion of digits – can performed at each MCPJ, PIPJ and DIPJ and brings the
Hand into a fist.
Extension of digits – can performed at each MCPJ, PIPJ and DIPJ and stretches the
hand out straight.
Abduction of digits – moving the digits away from the midline (middle of 3rd
digit).
Adduction of digits – moving the digits back toward the midline (middle of
3rd digit).
11
Opposition of thumb and little finger – bringing the thumb and little finger
together.
Reposition of thumb and little finger – moving the thumb and little finger away
from each other.
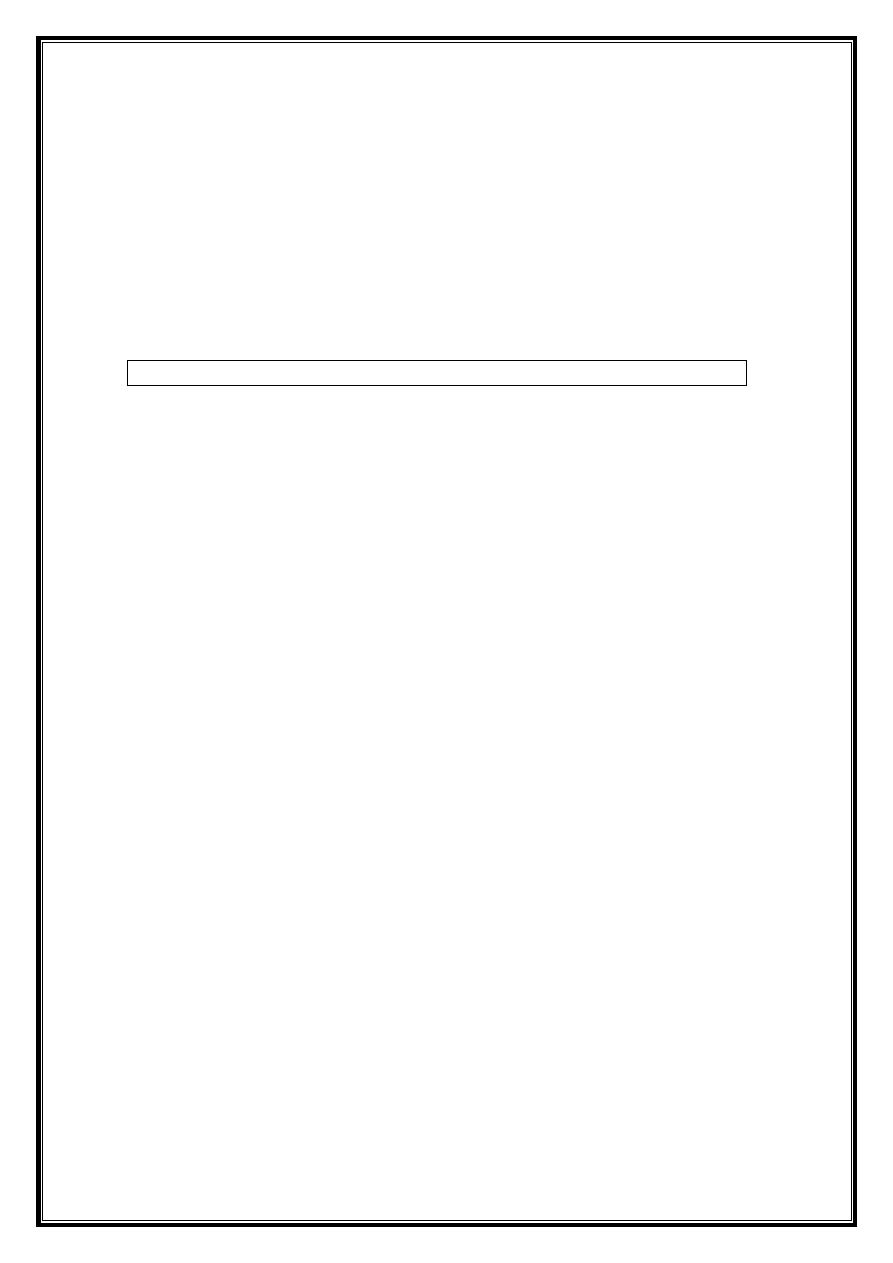
Fig 16 Palmar aponeurosis of the hand
Fascia
The palmar fascia consists of fibrous connective tissue, which thickens, in the
center of the hand forming the palmar aponeurosis, which is continuous with the
palmaris longus tendon and flexor retinaculum. The palmar aponeurosis protects
the underlying muscle compartments and fans out distally into four digital rays,
which then become the fibrous digital sheaths.
The fibrous digital sheaths cover the synovial sheaths (which contain the flexor
tendons) in the digits and keep them in place preventing bowstringing. By
maintaining the tension in the tendons, movements performed as efficiently and
accurately as possible.
Ligaments
Number of ligaments within the hand maintain stability of the structures within it:
Flexor Retinaculum – This thick strip of connective tissue forms
the roof of the carpal tunnel, protecting the structures within it. It
attaches medially to the pisiform and hook of hamate, and laterally
to the trapezium and scaphoid.
Extensor Retinaculum – This thickening of the fascia on the
dorsum of the hand keeps the extensor tendons in position,
preventing bowstringing.
12
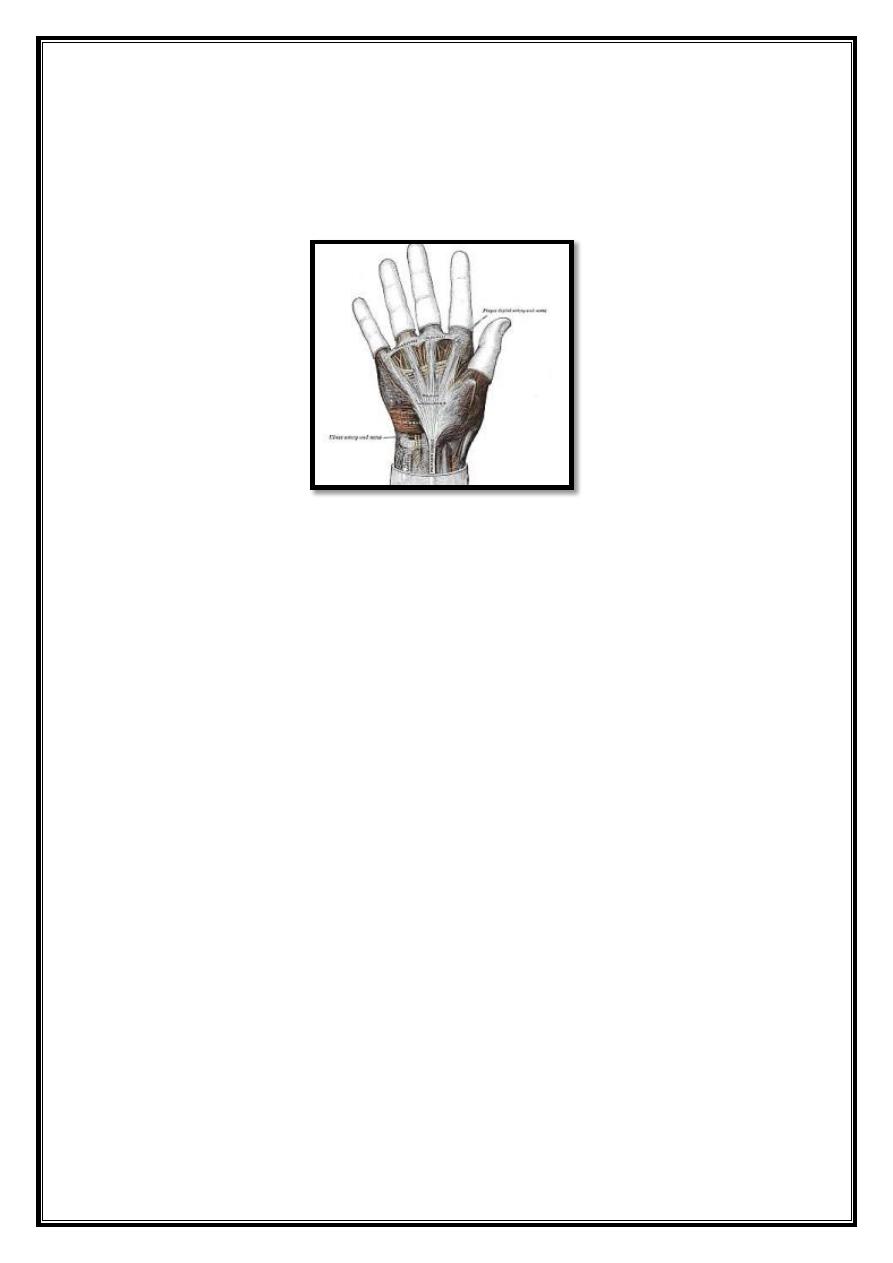
Palmar (Volar) Plates – These are structures present on the
palmar side of each MCP and interphalangeal joint, which limit
hyperextension of the digit, and therefore enhance its stability
Collateral Ligaments – are present on both the medial and lateral sides
of each MCP and interphalangeal joint. They are taut when the fingers are
flexed, thus limiting abduction when they are clenched in a fist. However,
they are lax when the fingers are extended, allowing abduction when the
fingers are in this position.
Fig 17. Volar (Palmar) Plates and Collateral Ligaments
13
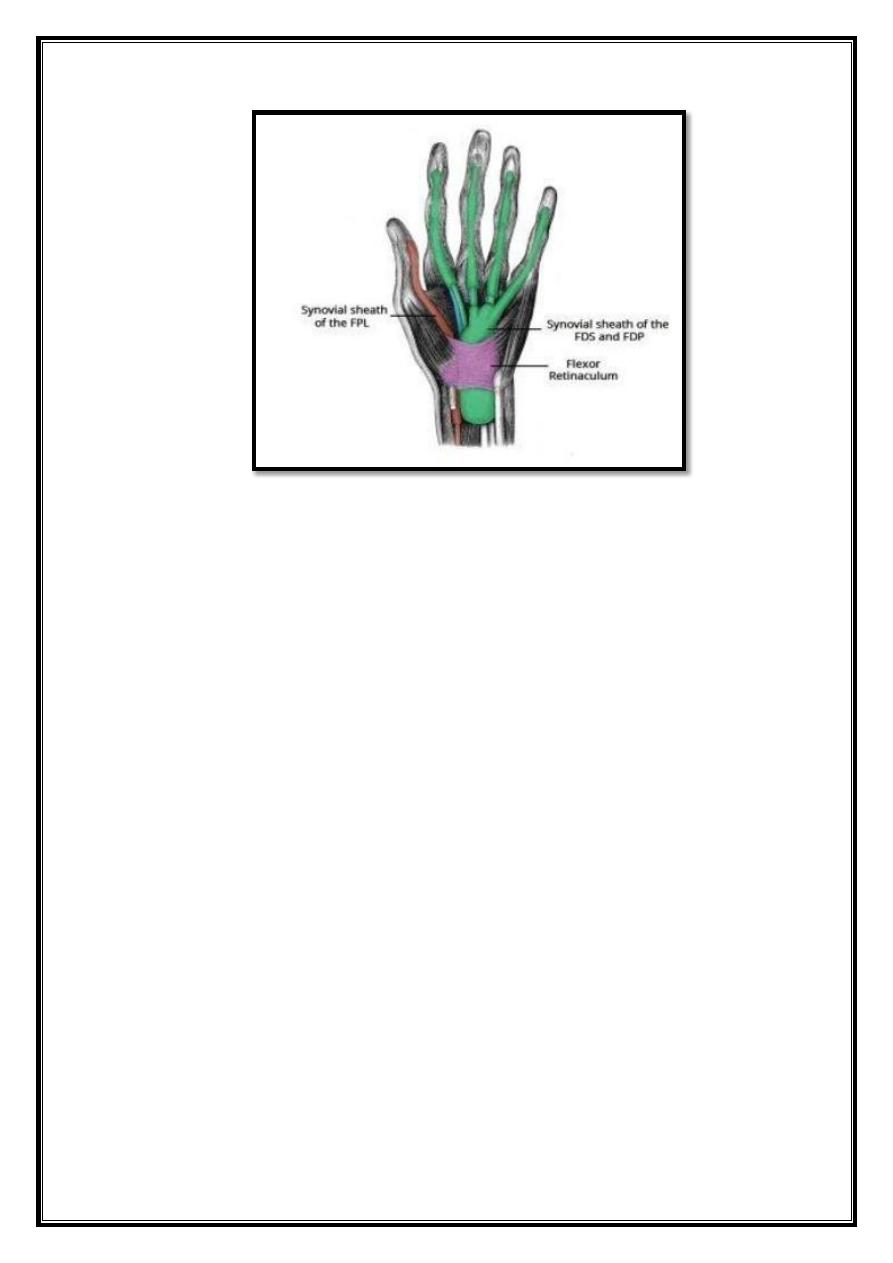
Fig 18. Synovial sheaths of the flexor tendons
Tendons
A number of muscles in the forearm whose tendons attach to the fingers to cause
an action:
Flexor Tendons in the Fingers – The flexor tendons of flexor digitorum
profundus (FDP) and flexor digitorum superficialis (FDS) allow flexion of the
fingers. They pass through the carpal tunnel and then enter into the hand where
they protected by the common flexor sheath.
This then fans out into the digital synovial sheaths in each finger, which permit
the free movement of the tendons over each other during flexion. In each finger,
the FDS tendon splits near the base of the proximal phalanx then inserts into the
intermediate phalanx. This allows the FDP tendon to pass through and insert onto
the distal phalanx.
Extensor Tendons in the Fingers – The tendons of the extensor digitorum
flatten as they reach the metacarpals and become extensor expansions (or hoods)
which fan out and wrap around the metacarpal and proximal phalanx joining onto
the palmar plate. This extensor expansion spreads out further distally into a
median band which attaches to the middle phalanx and two lateral bands which
attach to the distal phalanx. Contraction of the extensor digitorum muscle
tightens this tendon, which acts on these attachments and extends the fingers.
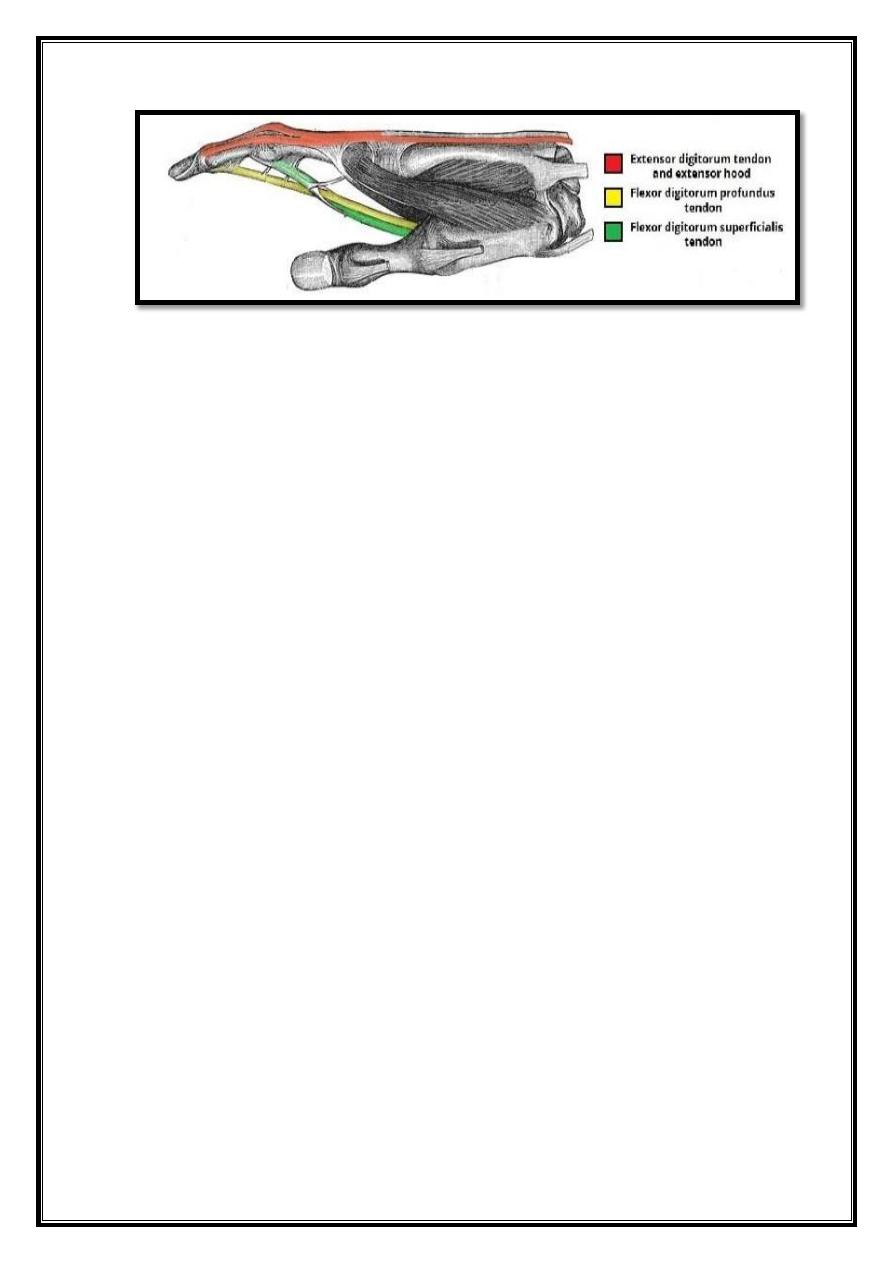
14
Fig 19. Tendons of FDS, FDP and extensor digitorum