1
Bones of upper limb
1
st
stage
Dr.Kalid Ali Zayer
Scapula
Contents
1. Costal Surface.
2. Lateral Surface.
3. Posterior Surface.
4. Articulations.
The scapula also known as the shoulder blade. It articulates with the humerus at the
glenohumeral joint, and with the clavicle at the acromioclavicular joint. In doing so, the
scapula connects the upper limb to the trunk.
It is a triangular, flat bone, which serves as a site for attachment for many (17!) muscles.
1.
Costal Surface
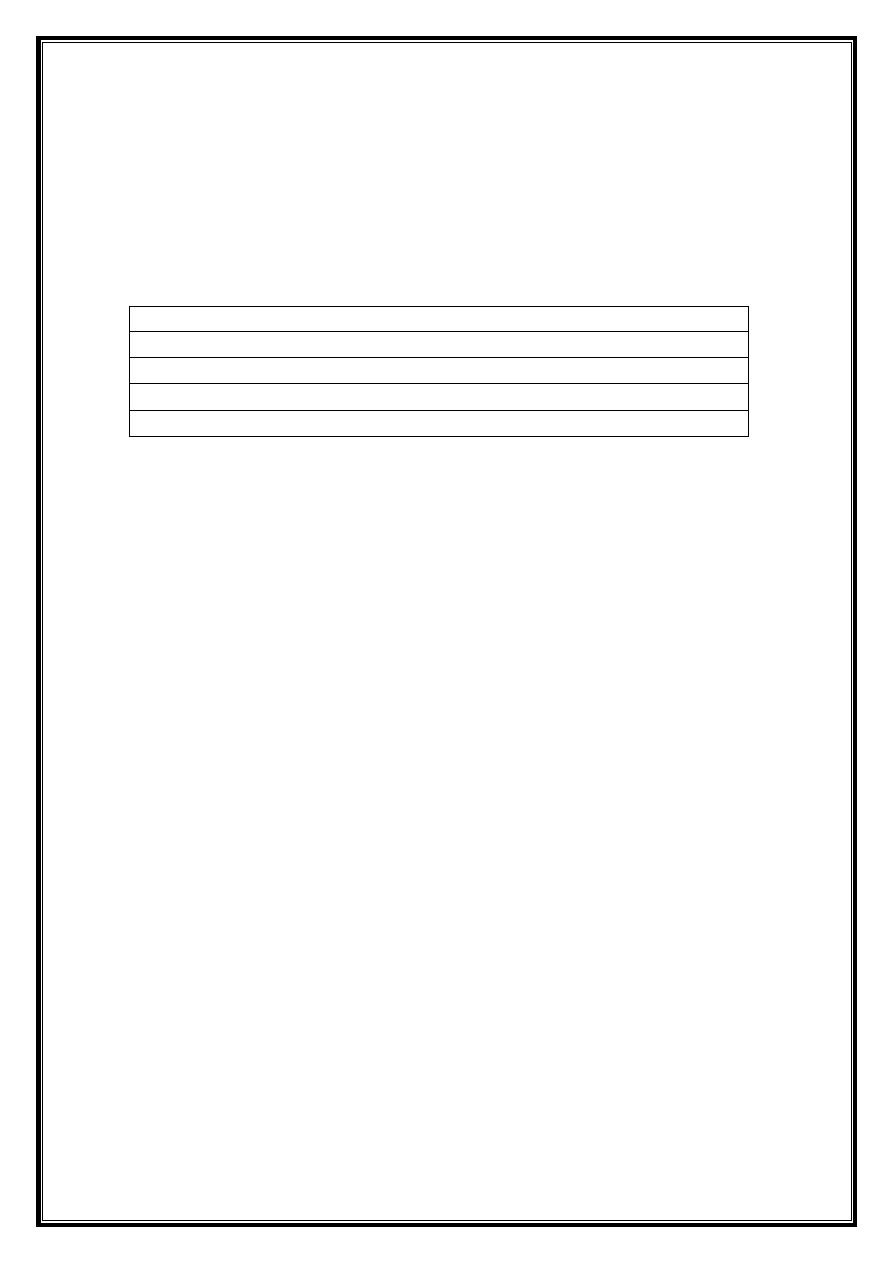
The costal (anterior) surface of the scapula faces the ribcage.
It contains a large concave depression over most of its surface, known as the
subscapular fossa.
The subscapularis (rotator cuff muscle) originates from this fossa.
Originating from the superolateral surface of the costal scapula is the coracoid
process. It is a hook-like projection, which lies just underneath the clavicle. The
pectoralis minor attaches here, while the coracobrachialis and biceps brachii (short
head) muscles originates from this projection.
2
Fig 1 – The costal surface of the scapula.
2.
Lateral Surface
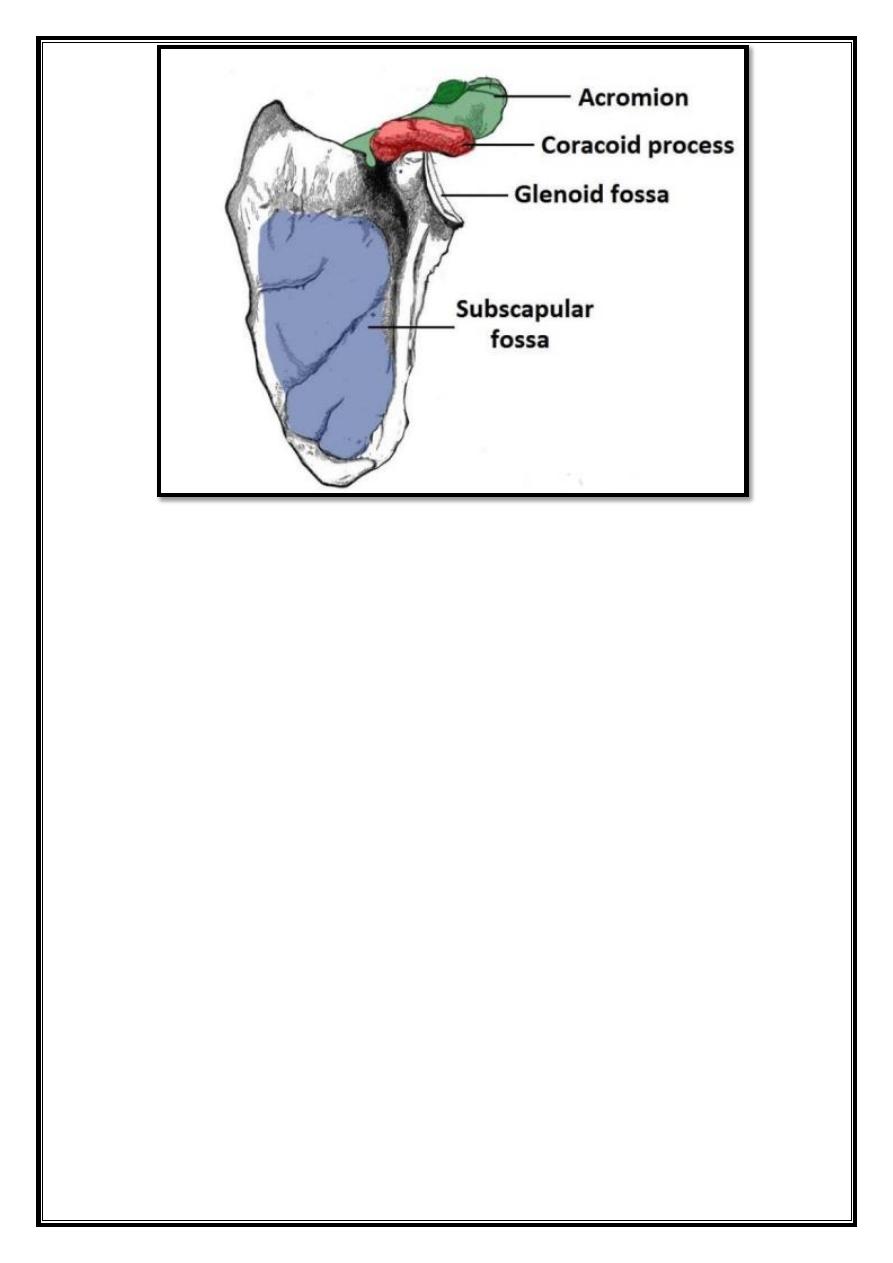
The lateral surface of the scapula faces the humerus. It is the site of the glenohumeral
joint, and of various muscle attachments. Its important bony landmarks include:
Glenoid fossa – a shallow cavity, located superiorly on the lateral border. It
articulates with the head of the humerus to form the glenohumeral (shoulder) joint.
Supraglenoid tubercle – a roughening immediately superior to the glenoid fossa.
The place of attachment of the long head of the biceps brachii.
Infraglenoid tubercle – a roughening immediately inferior to the glenoid fossa.
The place of attachment of the long head of the triceps brachii.
3
Fig 2 – Lateral view of the scapula.
3.
Posterior Surface
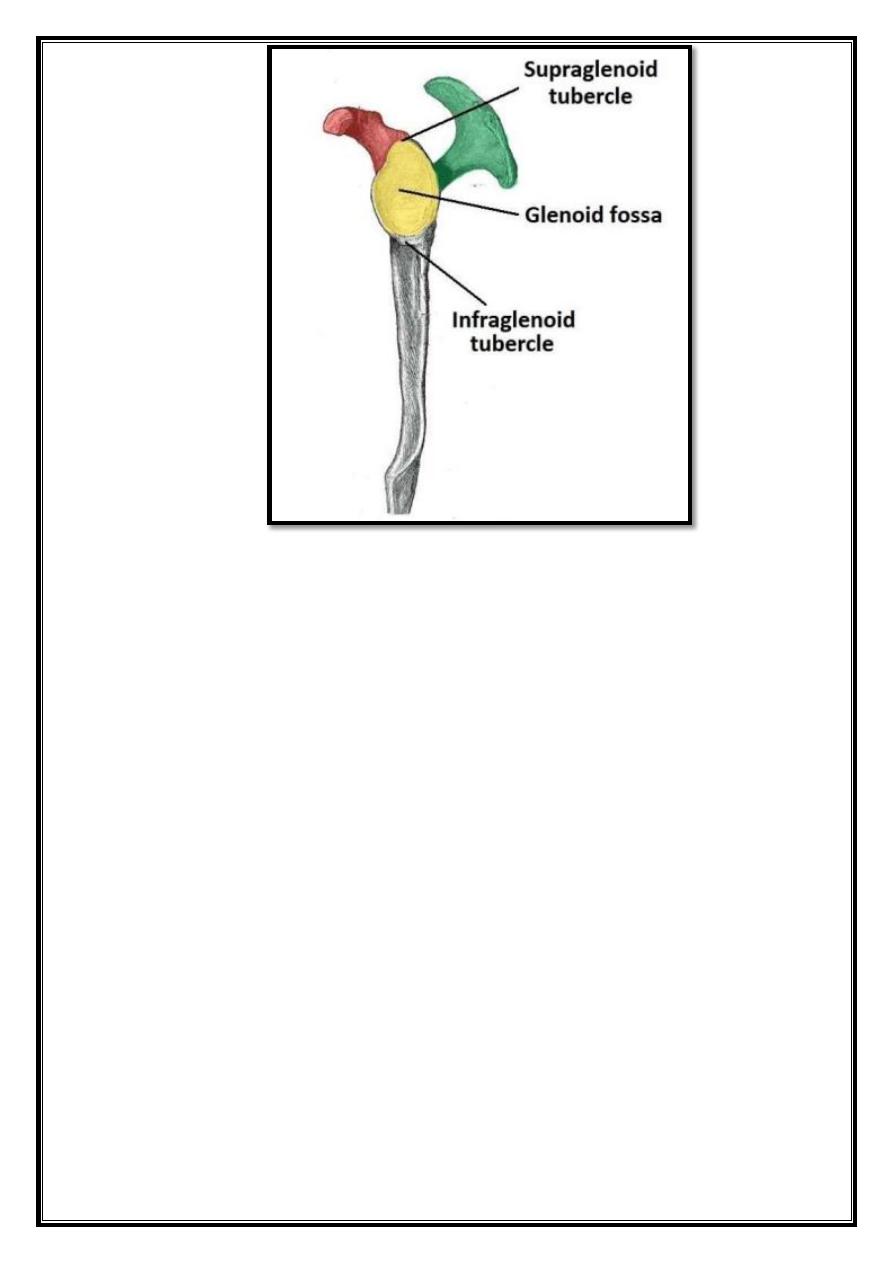
The posterior surface of the scapula faces outwards. It is a site of attachment for the
majority of the rotator cuff muscles of the shoulder. It is marked by:
Spine – the most prominent feature of the posterior scapula. It runs
transversely across the scapula, dividing the surface into two.
Acromion – projection of the spine that arches over the glenohumeral joint and
articulates with the clavicle at the acromioclavicular joint.
Infraspinous fossa – the area below the spine of the scapula, it displays a
convex shape.
o
The infraspinatus muscle originates from this area.
Supraspinous fossa – the area above the spine of the scapula, it is much
smaller than the infraspinous fossa, and is more convex in shape.
o
The supraspinatus muscle originates from this area.
4
Fig 3 – The posterior surface of the scapula.
4.
Articulations
The scapula has two main articulations:
Glenohumeral joint – between the glenoid fossa of the scapula and the head of the
humerus.
Acromioclavicular joint – between the acromion of the scapula and the clavicle.
Clavicle
Contents
1 Bony Landmarks and Articulations
o
1.1 Sternal (medial) End
o
1.2 Shaft
o
1.3 Acromial (lateral) End
The clavicle (collarbone) extends between the manubrium of the sternum and the acromion
of the scapula.
5
Fig 4 – The anatomical position of the clavicle
It classed as a long bone, and palpated along its length. In thin individuals, it is visible
under the skin. The clavicle has three main functions:
1. Attaches the upper limb to the trunk as part of the ‘shoulder girdle’.
2. Protects the underlying neurovascular structures supplying the upper limb.
3. Transmits force from the upper limb to the axial skeleton.
1.
Bony Landmarks and Articulations
The clavicle is a slender bone with an ‘S’ shape. Facing forward, the medial aspect is
convex, and the lateral aspect concave. It divided into a sternal end, a shaft and an
acromial end.
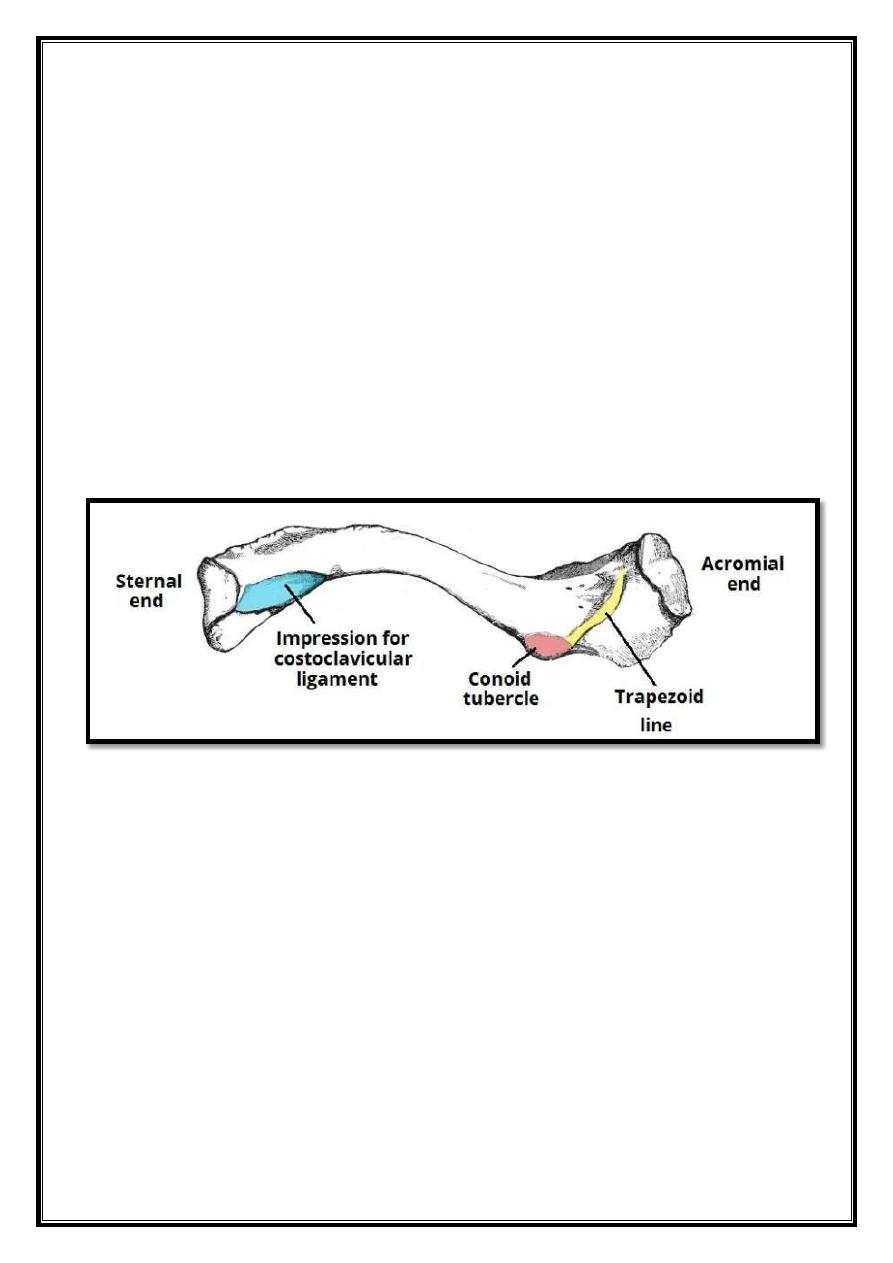
1.1. Sternal (medial) End
The sternal end contains a large facet – for articulation with the manubrium of the
sternum at the sternoclavicular joint.
The inferior surface of the sternal end marked by a rough oval depression for the
costoclavicular ligament (a ligament of the SC joint).
6
1.2.Shaft
The shaft of the clavicle acts a point of origin and attachment for several muscles –
deltoid,trapezius, subclavius, pectoralis major, sternocleidomastoid and Sternohyoid.
1.3.Acromial (lateral) End
The acromial end houses a small facet for articulation with the acromion of the scapula at
the acromioclavicular joint. It also serves as an attachment point for two ligaments:
Conoid tubercle – attachment point of the conoid ligament, the medial part of the
coracoclavicular ligament.
Trapezoid line – attachment point of the trapezoid ligament, the lateral part of the
coracoclavicular ligament.
The coracoclavicular ligament is a very strong structure, effectively suspending the
weight of the upper limb from the clavicle.
Fig 5 – Bony landmarks of the inferior surface of the clavicle.
7
Humerus
Contents
1 Proximal Landmarks
o
1.1 Clinical Relevance: Surgical Neck Fracture
2 Shaft
o
2.1 Clinical Relevance: Mid-Shaft Fracture
3 Distal Region
4 Articulations
The humerus is a long bone of the upper limb, which extends from the shoulder to the
elbow.
The proximal region of the humerus articulates with the glenoid fossa of the scapula, forming
the glenohumeral joint. Distally, at the elbow joint, the humerus articulates with the head of
the radius and trochlear notch of the ulna.
Fig 6 – The anatomical position of the humerus
8
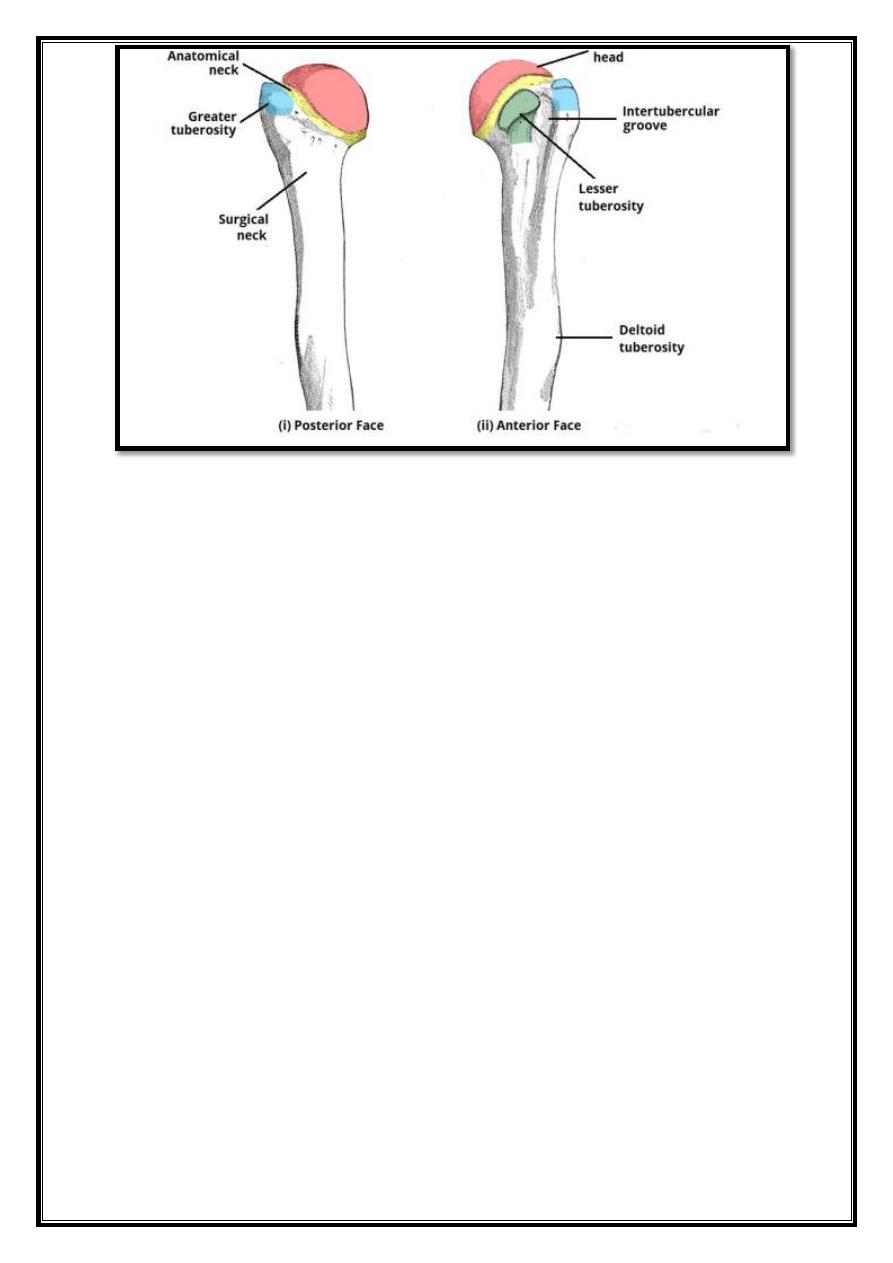
1.
Proximal Landmarks
The proximal humerus is marked by a head, anatomical neck, surgical neck, greater and
lesser tubercles and intertubercular sulcus (a tubercle is a round nodule, and signifies the
attachment site of a muscle or ligament).
The upper end of the humerus consists of the head. This faces medially, upwards and
backwards and separated from the greater and lesser tubercle by the anatomical neck.
The greater tubercle is located laterally on the humerus. It has an anterior and posterior face.
The greater tubercle serves as attachment site for three of the rotator cuff muscles –
supraspinatus, infraspinatus and teres minor – they attach to superior, middle and inferior
facets respectively.
The lesser tubercle is much smaller, and more medially located on the bone. It only has an
anterior face. It provides attachment for the last rotator cuff muscle; subscapularis.
Separating the two tubercles is a deep depression, called the intertubercular sulcus, or
groove.
The tendon of the long head of biceps brachii emerges from the shoulder joint and runs
through this groove.
The edges of the intertubercular sulcus known as lips. Pectoralis major, teres major
and latissimus dorsi insert on the lips of the intertubercular sulcus. This can be remembered
with the mnemonic “a lady between two majors”, with latissimus dorsi attaching between
teres major on the medial lip and pectoralis major laterally.
The surgical neck runs from just distal to the tubercles to the shaft of the humerus. The
axillary nerve and circumflex humeral vessels lie against here.
9
Fig 7 – The proximal aspect of the humerus. Note the greater and lesser tuberosities as a
site of attachment for muscles.
2. Shaft
The shaft of the humerus is the site of attachment for various muscles. Cross section views
reveal it to be circular proximally and flattened distally.
On the lateral side of the humeral shaft is a roughened surface where the deltoid
muscle attaches. This known as the deltoid tuberosity.
The radial (or spiral) groove is a shallow depression that runs diagonally down the
posterior surface of the humerus, parallel to the deltoid tuberosity. The radial nerve and
profunda brachii artery lie in this groove. The following muscles attach to the humerus along
its shaft:
Anteriorly – coracobrachialis, deltoid, brachialis, brachioradialis.
Posteriorly – medial and lateral heads of the triceps (the spiral groove demarcates their
respective origins).
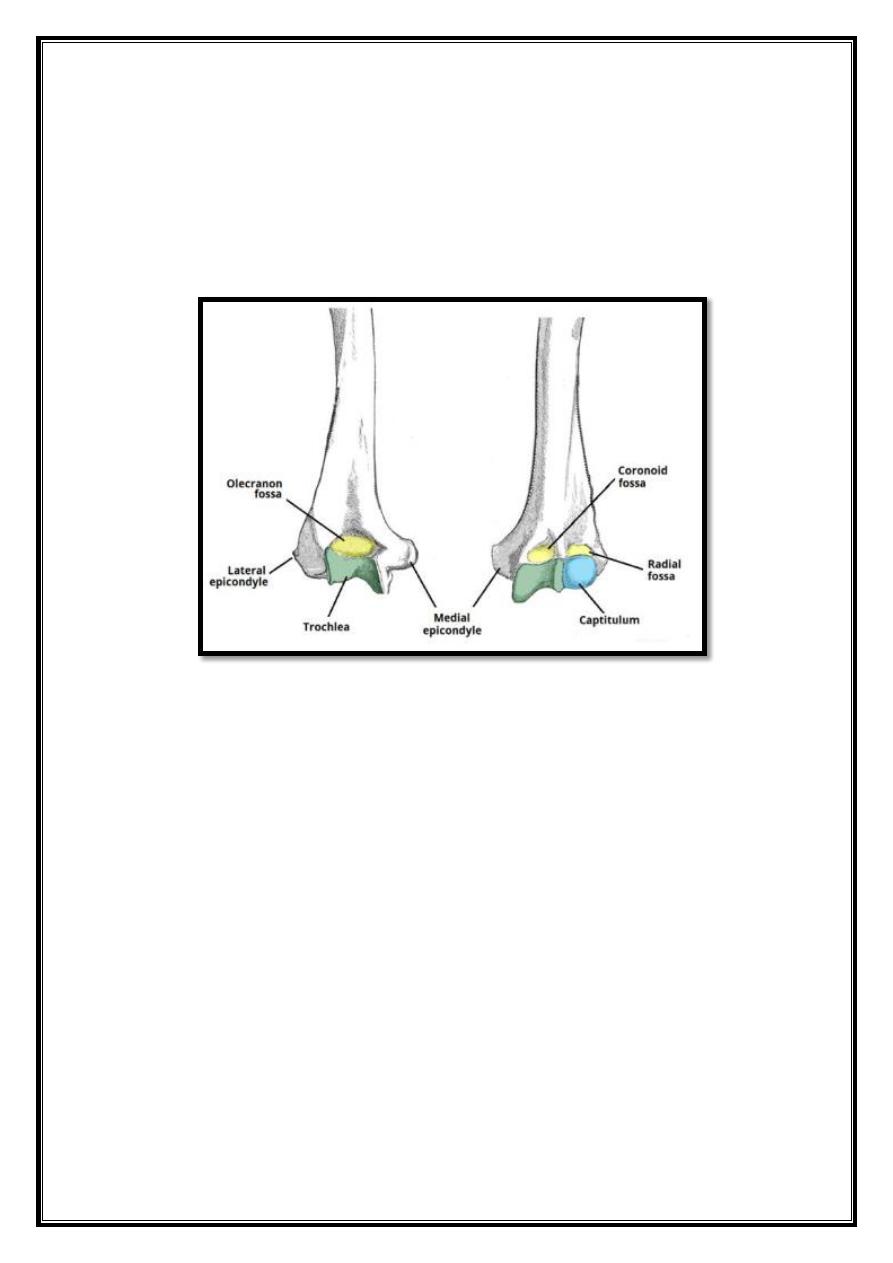
Distal Region
The lateral and medial borders of the distal humerus form medial and lateral
supraepicondylar ridges. The lateral supraepicondylar ridge is more roughened, providing
the site of common origin of the forearm extensor muscles.
Immediately distal to the supraepicondylar ridges are extracapsular projections of bone,
the lateral and medial epicondyles. Both can be palpated at the elbow. The medial is the
larger of the two and extends more distally.
10
The ulnar nerve passes in a groove on the posterior aspect of the medial epicondyle where it
is palpable.
Distally, the trochlea is located medially, and extends onto the posterior aspect of the bone.
Lateral to the trochlea is the capitulum, which articulates with the radius.
Also located on the distal portion of the humerus are three depressions, known as
the coronoid, radial and olecranon fossae. They accommodate the forearm bones during
movement at the elbow.
Fig 8 – Bony landmarks of the distal humerus. It articulates with the radius and ulna to
form the elbow joint.
3.
Articulations
The proximal region of the humerus articulates with the glenoid fossa of the scapula to
form the glenohumeral joint (shoulder joint).
Distally, at the elbow joint, the capitulum of the humerus articulates with the head of the
radius and the trochlea of the humerus articulates with the trochlear notch of the ulna.