
1
The Pituitary Gland
The Pituitary Gland
It is the master endocrine gland , consists of 3 lobes ( anterior,
intermediate and posterior) which are more or less separated endocrine
glands.
The intermediate lobe is rudimentary in humans.
The anterior and posterior lobes are entirely distinct physiologically.
The Anterior pituitary
( Adenohypophysis)
Classification:
anterior pituitary gland secretes three hormone groups:
1- Protein hormone group:
a. Growth hormone.
b. Prolactin.
c. Placental lactogen(chorionic somatomammotropin).
2- Glycoprotein hormone group:
a. TSH.
b. LH.
c. FSH.
d. Chorionic gonadotropin.
3- Pro-opio-melano-cortin(POMC) peptide group:
a. ACTH.
b. Melanocyte stimulating hormone (MSH).
c. β-lipotropin.
d. Endorphins.
e. Enkephalin.

2
Growth hormone “ GH”
GH secretion is controlled by 2 hypothalamic hormones:
1. GHRH (growth hormone releasing hormone)
2.GHRIH
(
growth
hormone
release
inhibitory
hormone
,”Somatostatin” ).
GH is a single poly peptide synthesized by the somatotropes ( anterior
pituitary acidophilic cells).
Secretion of GHRH, and therefore of GH is
pulsatile occurring about seven or eight times a day usually associated
with the following:
a) exercise,
b) onset of deep sleep,
c) in response to the falling plasma glucose concentration an hour
after meals.
Effects of GH
1. Protein metabolism:-
GH is protein anabolic H. It increases the transport of amino acids
into muscle cells.
2. Carbohydrate metabolism :-
GH antagonizes the effects of insulin, it decreases the peripheral
glucose utilization, and increases hepatic glucose production via
gluconeogenesis. GH also increases liver glycogen.
3. Lipid metabolism :-
GH promotes the release of fatty acids and glycerol from adipose
tissues and increases circulating fatty acids. It also increases fatty
acid oxidation in the liver.
4. Mineral metabolism :-
It promotes positive Ca, Mg, and P balance, and causes retention of
Na, K and Cl. It promotes the growth of long bones at the
epiphyseal plate in growing in children and acral growth in adults.
It also enhances cartilage formation in children.
5. PRL – like effects:-
It bind to lactogenic receptors, and has many of PRL effects such
as stimulation of mammary gland and lactogenesis
.
3
Pathophysiology:
GH deficiency
1. GH deficiency in childhood result in short stature, a condition called
Dwarfism
2. GH deficiency in adulthood result in lethargy, muscle weakness and
increased fat mass
.
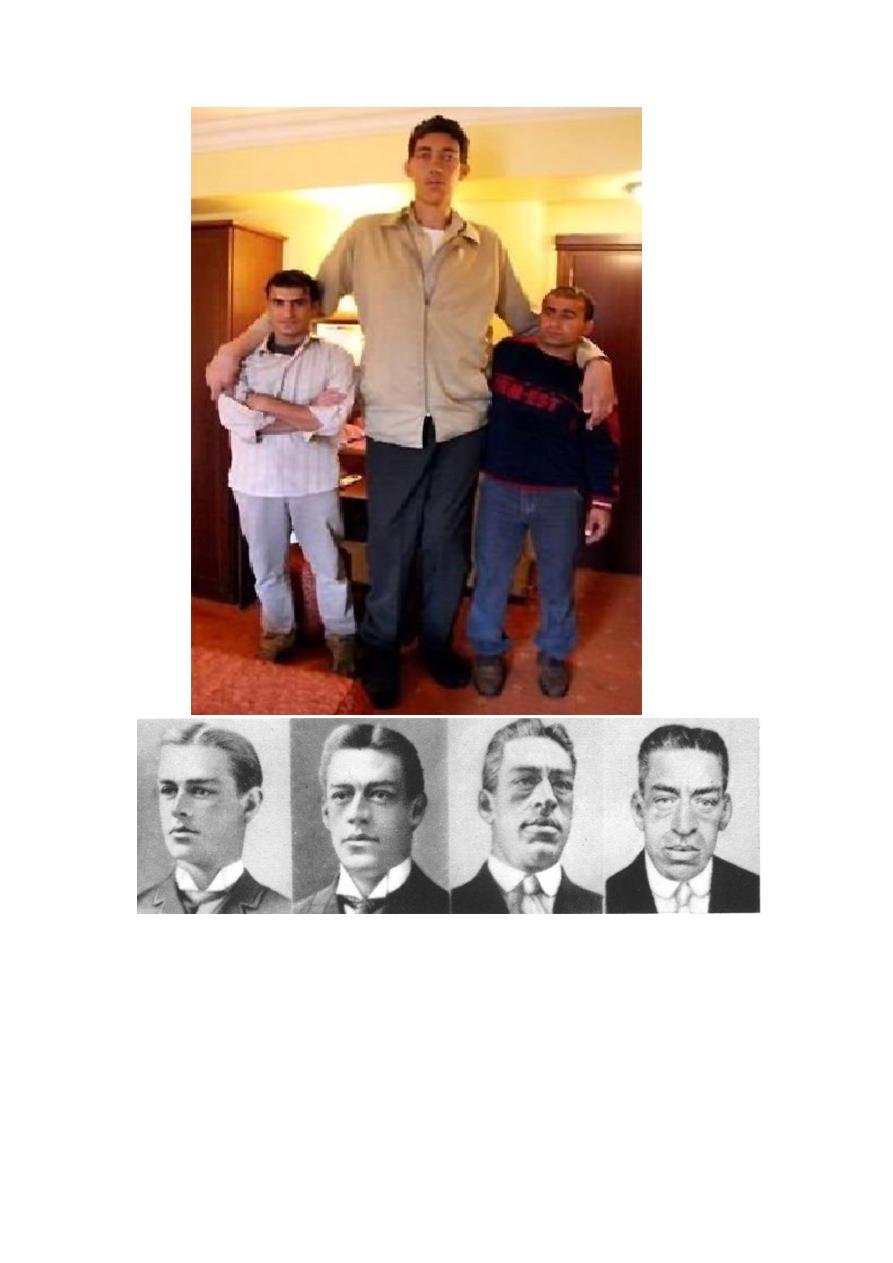
GH excess
1. If occurs before the closure of epiphyseal plate leads to an increase
in the growth of long bones, a condition called Gigantism.
2. If it occurs after epiphyseal plate closure, then it results in
Acromegaly in which
3. An increase in bulk of bone and soft tissues causing the
characteristic appearance (protruding jaw, enlarged nose, and also
enlargement of hands, feet and skull).
Excessive hair growth and sebaceous gland secretion.
Menstrual disturbances.
Impaired glucose tolerance.
4

5
Prolactin “ PRL”
Is a protein hormone secreted by the lactotropes ( Pituitary acidophilic
cells).
PRL secretion is under predominantly inhibitory control by Dopamine
which is secreted by hypothalamus. However, TRH (Thyrotropin
releasing hormone), secreted by hypothalamus may , in some instances,
stimulate PRL secretion.
It is important during pregnancy& post partum period. Prolactin
secretion increases progressively after the eight week of pregnancy
probably because of the high estrogen concentration. At term, it may be
10 to 20 times that of non pregnant woman.
Effects
Women:- Initiation and maintenance of lactation .
Men:- not clearly known yet.
Pathophysiology
Women:-
Excessive RRL ( hyperprolactinaemia) causes amenorrhoea and
galactorrhoea.
Pathological causes of hyperprolactinaemia:-
1- A prolactin secreting micro adenoma of the pituitary gland.
2- Failure of hypothalamic inhibitory factors to reach the anterior
pituitary gland.
3- Other pituitary tumors.
4- Drugs such as: - estrogen. dopaminergic agonist (phenothiazin,
mitoclopramide).
5- Chronic renal failure.
6- Severe primary hypothyroidism.
Men:-
Excessive PRL results in erectile dysfunction, impotence and
gynaecomastia. Also, it may result in oligospermia.

6
Thyroid – Stimulating hormone “ TSH”
Is a glycoprotein hormone. It’s secretion is controlled by the
hypothalamic TRH. It is synthesized by the thyrotropes (basophilic
pituitary cells).
Effects:-
Stimulate the growth of thyroid gland, and the synthesis and release of
thyroid hormones ( T
4
& T
3
).
The secretion of TSH from the anterior pituitary gland is controlled by:-
Circulating concentration of thyroid hormone.
thyrotrophin releasing hormone (TRH) which produced In the
hypothalamus and stimulate TSH secretion.
Follicle – Stimulating hormone “FSH”
and
Luteinizing hormone “LH”
Interestingly, although there is only one releasing H. for both FSH and
LH called LH and FSH releasing H “ GnRH” ( LHRH, FSHRH) secreted
by the hypothalamus, however, LH and FSH can be secreted
independently.
FSH and LH are glycoproteins secreted by the gonadotropes (basophilic
pituitary cells).
Effects of LH
Women:
Induces ovulation stimulate progesterone production by the
corpus luteum , and also, is required for the early maintenance of corpus
luteum.
Men:
Stimulate testosterone production by the Leydig cells of the testis.
Effects of FSH
Women:-
Stimulate the maturation of ovarian follicle causing an increase
in estradiol production by the granulosa cells of the follicle.
Men:-
FSH is essential for maintenance of spermatogenesis. FSH bind to
sertoli cells of Testis, promotes synthesis of ABP “ androgen binding
protein” which bind to testosterone and transport it to the lumen of
seminiferous tubules ( the site of spermatogenesis ).

7
Adrenocorticotropic hormone “ACTH”
Is a single poly peptide secreted by the cortictrops basophilic pituitary
cells under the control of the hypothalamic CRH ( corticotrophin-
releasing H.)
Effects:-
It regulate the growth and function of adrenal cortex, and enhances the
production of adrenal steroids ( glucocorticoids, mineralocorticoids &
dehydroepiandrosterone ). ACTH also has considerable MSH activity.
β - Lipotropin “β–LPH”
It is found only in the pituitary since it is rapidly converted to γ- LPH and
β - endorphin in other tissues.
Effects:-
causes lipolysis and fatty acids mobilization, but it physiological
role is minimal. It probably serves only as the precursor of β–Endorphin
which in turn behave as the precursor of α-endorphin and γ-endorphin.
Endorphins :
acts inside the CNS as neurotansmitters and are involved in
endogenous pain perception.
γ–Melanocyte – Stimulating hormone “γ-MSH”
They increases pigmentation of the skin and mucous membrane by
stimulating melanin synthesis in the melanocytes, and also, causes
dispersion of the intracellular melanin granules resulting in skin
darkening.
The pituitary in mammals contain 3 MSHs:-
1. α –MSH
2. β -MSH
3. γ -MSH
γ-MSH is present in high concentration in the intermediate lobe, but is
also present in the anterior pituitary. In adults , it appear that neither α -
MSH nor β -MSH are secreted.
8
Hypopituitarism:-
The anterior pituitary gland has considerable functional reserve.
Clinical features of deficiency are usually absent until about 70% of the
gland has been destroyed.
Causes of hypopituitarism:-
1. Destruction of, or damage to, the anterior pituitary gland or the
hypothalamus by a primary or secondary tumor.
2. Infarction most commonly postpartum (Sheehan ̓s syndrome).
3. Pituitary surgery or irradiation.
4. Less common causes include:- a-head injury .
b-Infection or granulomas.
The Posterior Pituitary
( Neurohypophysis )
It secretes 2 Hs which are synthesized by the hypothalamus and are
transported into the nerve endings in the posterior pituitary, where upon
appropriate stimulation, these Hs are released into the circulation:-
1. Oxytocin
2. Antidiuretic H. (ADH), “ Vasopressin ”
Each of them is a peptide of 9 amino acids.
Oxytocin
It's secretion is stimulated by neural impulses resulting from nipple
stimulation, vaginal and uterine distension. And by oestrogen.
While progesterone inhibit oxytocin production.
Effects of
Oxytocin
Women : - Causes contraction of uterine smooth muscle. Thus ,it is used
therapeutically for the induction of labour also it stimulate the contraction
of myoepithelial cells surrounding the mammary alveoli promoting milk
ejection from the breast.
Men:- not clearly known yet

9
HOWEVER, Current evidence suggests that oxytocin is involved in
facilitating sperm transport within the male reproductive system and
perhaps also in the female, due to its presence in seminal fluid. It may
also have effects on some aspects of male sexual behavior.
Antidiuretic H. (ADH), “ Vasopressin ”
ADH secretion is stimulated by :-
1. Increased plasma osmolality
2. Physical stress
3. Emotional stress
4. Pharmacological agents:-
-Acetylcholine,- Nicotine, - Morphine.
Effects:
Acts on the distal convoluted tubules and collecting ducts of the kidneys
causing water reabsorption by the renal tubules , permitting osmotic
equilibrium of the cells of interstitium.
Pathophysiology
Diabetes Insipidus:
Deficiency of ADH or its action leads to Diabetes
lnsipidus (DI) which is characterized by excretion of large quantities of
extremely diluted urine ( of very low specific gravity).
DI could be:-
1. Cranial ( primary) DI:- due to insufficient ADH secretion.
2. Nephrogenic ( Secondary) DI:- ADH is normally secreted but,
either there is inherited defect or acquired damage in ADH
receptors.