Gastric Polyps and Tumors
Polyps, nodules or masses that project above the level of the surrounding mucosa.Polyps may develop as a result of epithelial or stromal cell hyperplasia, inflammation, or neoplasia.
1-INFLAMMATORY AND HYPERPLASTIC POLYPS
Approximately 75% of all gastric polyps are inflammatory or hyperplastic polyps. They are most common in individuals between 50 and 60 years of age. These polyps usually develop in association with chronic gastritis,Among individuals with H. pylori gastritis, polyps may regress after bacterial eradication.
Because the risk of dysplasia correlates with size, polyps larger than 1.5 cm should be resected and examined histologically.
Morphology.
The majority of inflammatory or hyperplastic polyps are smaller than 1 cm in diameter and are frequently multiple, particularly in individuals with atrophic gastritis.Microscopically, polyps have irregular, cystically dilated, and elongated foveolar glands .
Gastric hyperplastic polyp. Low-power microscopic view of the polyp showing hyperplastic foveolar epithelium and inflammation.
2-GASTRIC ADENOMA
10% of all gastric polypsPatients are usually between 50 and 60 years of age, and males are affected three times more often than females.
adenomas almost always occur on a background of chronic gastritis with atrophy and intestinal metaplasia.
The risk of adenocarcinoma in gastric adenomas is related to the size of the lesion and is particularly elevated in lesions greater than 2 cm in diameter.
Morphology.
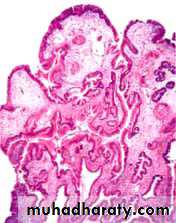
Gastric adenomas are usually solitary lesions less than 2 cm in diameter, most commonly located in the antrum.
By definition, all GI adenomas have epithelial dysplasia that can be classified as low or high grade.
Gastric adenoma. Gross photograph showing a large polyp in the stomach.

Gastric carcinoma
Adenocarcioma is the most common.Carcinoma 90-95%
Lymphoma 4%
Carcinoid 3%
Mesenchymal spindle cell tumor 2%
Epidemiology and classification
High incidence in Japans, Colombia, Costa Rica.Mass endoscopic screening programs can be successful in regions where the incidence is high, such as Japan, where 35% of newly detected cases are early gastric cancer, tumors limited to the mucosa and submucosa.
There are two morphological types:
Intestinal variant
Diffuse variant
Intestinal type
Predisposed by chronic gastritis.Most common type in high risk population.
Arise from gastric mucous cells that have undergone intestinal metaplasia.
Better differentiated than diffuse type.
Diffuse type
Arise denovo from native mucous cells.Not associated with chronic gastritis.
Poorly differentiated.
Risk factors
Intestinal-Type Adenocarcinoma◘Diet
Nitrites derived from nitrate.
Smoked foods and pickled vegetables
Excessive salt intake
Decreased intake of fresh vegetables and fruits: antioxidants present in these foods may be protective
◘Chronic gastritis with intestinal metaplasia
Infection with Helicobacter pyloriPernicious anemia
◘Altered anatomy
After subtotal distal gasrectomy
2- Diffuse carcinoma
Risk factors undefined
morphology
Most gastric adenocarcinomas involve the gastric antrum;the lesser curvature is involved more often than the greater curvature.
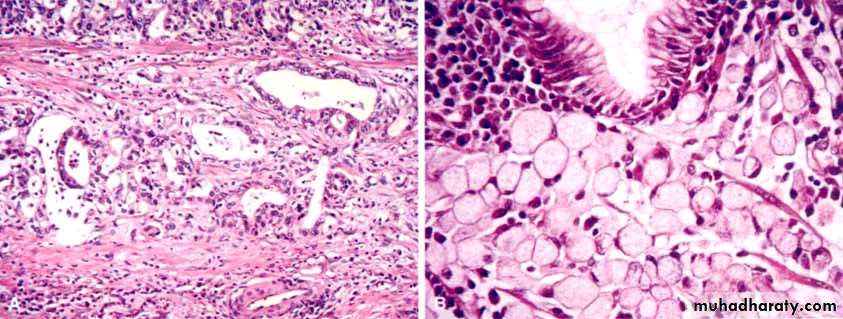
Gastric tumors with an intestinal morphology tend to form bulky tumors composed of glandular structures,
while cancers with a diffuse infiltrative growth pattern are more often composed of signet-ring cells .
intestinal-type adenocarcinomas typically grow to form either an exophytic mass or an ulcerated tumor. The neoplastic cells often contain apical mucin vacuoles, and abundant mucin may be present in gland lumens
diffuse gastric cancer is generally composed of discohesive cells that do not form glands but instead have large mucin vacuoles that expand the cytoplasm and push the nucleus to the periphery, creating a signet-ring cell morphology. These cells permeate the mucosa and stomach wall individually or in small clusters
A mass may be difficult to appreciate in diffuse gastric cancer,
but these infiltrative tumors often evoke a desmoplastic reaction that stiffens the gastric wall and may provide a valuable diagnostic clue.When there are large areas of infitration, diffuse rugal flattening and a rigid, thickened wall may impart a leather bottle appearance termed linitis plastica
all gastric carcinomas eventually penetrate the wall to involve the serosa, spread to regional and more distant lymph nodes, and metastasize widely.
For obscure reasons, the earliest lymph node metastasis may sometimes involve a supraclavicular lymph node (Virchow’s node).
Another somewhat unusual mode of intraperitoneal spread in females is to both the ovaries, giving rise to the so-called Krukenberg tumor.
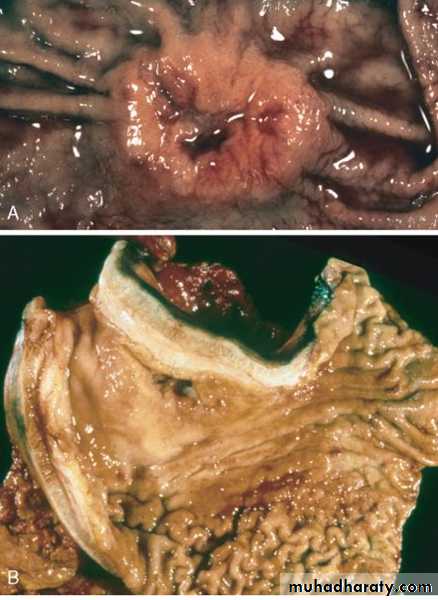
Gastric adenocarcinoma. A, Intestinal-type adenocarcinoma consisting of an elevated mass with heaped-up borders and central ulceration. B,Linitis plastica. The gastric wall is markedly thickened, and rugal folds are partially lost.

Gastric carcinoma. A, Intestinal type demonstrating gland formation by malignant cells, which are invading the muscular wall of the stomach. B, Diffuse type demonstrating signet-ring carcinoma cells.