CHEMICAL AND INFECTIOUS ESOPHAGITIS
The stratified squamous mucosa of the esophagus may be damaged by a variety of irritants including alcohol, corrosive acids or alkalis, excessively hot fluids, and heavy smoking. The esophageal mucosa may also be injured when medicinal pills lodge and dissolve in the esophagus rather than passing into the stomach intact, a condition termed pill-induced esophagitis.
Esophagitis due to chemical injury generally only causes:
self-limited pain, particularly dysphagia (pain with swallowing).Hemorrhage,
stricture,
or perforation may occur in severe cases.
Infectious esophagitis
Infections may occur in otherwise healthy individuals but are most frequent in those who are deblitated or immunosuppressed as a result of disease or therapy.Reflux esophagitis
GE reflux disease affects about 0.5% of the US adult population.Dominant symptom recurrent heartburn.
Etiology:
Decrease efficacy of esophageal antireflux mechanisms.
Inadequate or slowed esophageal clearance of refluxed material.
Sliding hiatal hernia.
Increased gastric volume.
Impaired reparative capacity of the esophagus mucosa by prolonged exposure to gastric juices.
Morphology
Gross: depend on:Causative agent
Duration
Severity
Mild only hyperemia
Severe epithelial erosions, or total ulceration Microscopically:
eosinophils, with or without neutrophils, in the epithelial layer.

COMPLICATIONS
BLEEDINGSTRICTURE
BARRETT ESOPHAGUS
PREDISPOSITION TO MALIGNANCY
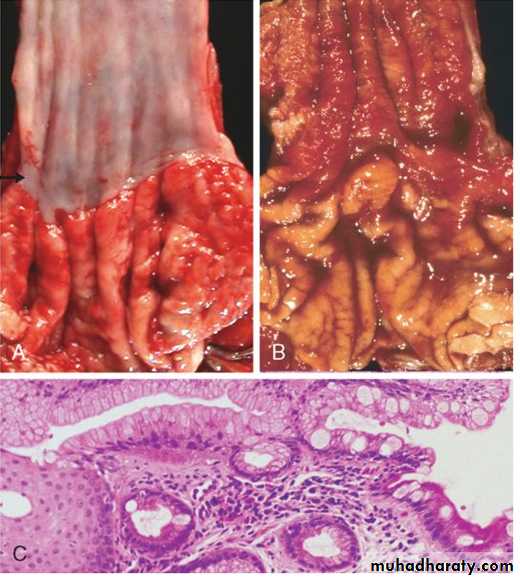
Barrett esophagus
It is a complication of long-standing gastroesophageal reflux, occurring in up to 10% of patients with persistent symptomatic reflux disease, as well as in some patients with asymptomatic reflux.Barrret esophagus is defined as the replacement of the normal distal stratified squamous mucosa by metaplastic columnar epithelium containing goblet cells.
pathogenesis
Prolonged and recurrent gastroesophageal reflux is thought to produce inflammationand eventually ulceration of the squamous epithelial lining of lower esophagus.
Healing occurs by re-epithelialization. to the columnar epithehum.
Metaplastic columnar epithelium is thought to be more resistant to injury from refluxing gastric contents.
males more often than females (ratio of 4:1)
much more common in whites than in other races.Genetic factors are suggested by clustering in families.
Complications
Ulcer and stricture
adenocarcinoma. Patients with Barrett esophagus have a 30 to 40 fold greater risk of developing esophageal adenocarcinoma compared with normal populations.
MORPHOLOGY
salmon-pink, velvety mucosa between the smooth, pale pink esophageal squamous mucosa and the more light brown gastric mucosa.Microscopically, the esophageal squamous epithelium is replaced by metaplastic columnar epithelium.with goblet cells.
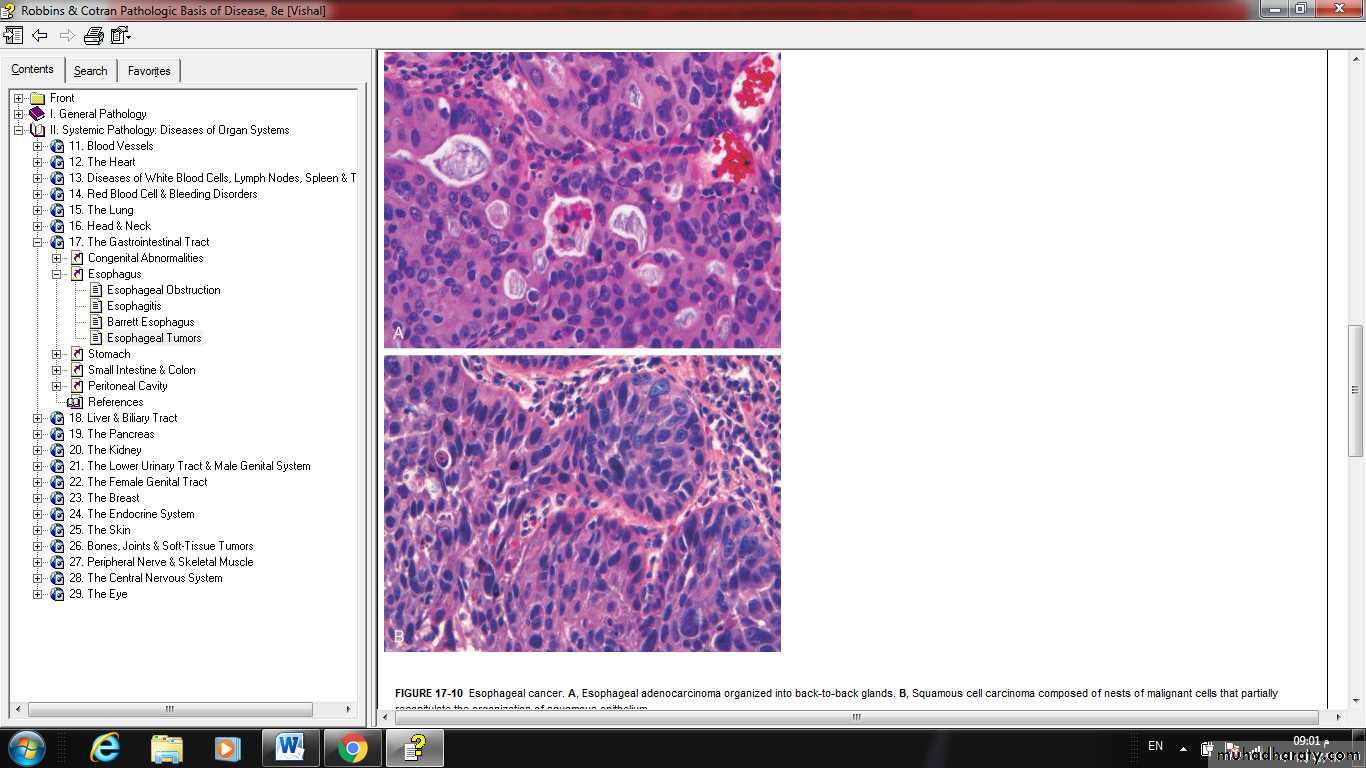
Esophageal carcinoma
• Squamous cell carcinomaoccurs in adults over age 45
affects males four times more frequently than females.
It is nearly sixfold more common in African-Americans than Caucasians, a striking risk disparity that reflects differences in rates of alcohol and tobacco use as well as other poorly understood factors.
•
Etiology and pathogenesis of SCC
• Esophageal disorders:• ◙ long standing esophagitis.
• ◙ Achalasia
• ◙ Plumer-Vinson $.
• esophageal web
• microcytic hypochromic anemia
• atrophic glossitis
• 2- Life style:
• alcoholic consumption• tobacco abuse
• 3- Dietry
• deficiency of vitamins.
• deficiency of metals
• fungal contamination of food stuffs
• high contents of nitrites/ nitrosamines
• 4- Genetic predisposition:
• Tylosis which is hyperkeratosis of palms and soles.• There is a link between mentioned risk factors and molecular changes;
• * mutation of tumor suppressor gene P53
• * mutation of k- RAS gene.
morphology
Gross:Three patterns;
Polypoid,
necrotizing cancerous ulceration,
or diffuse infiltrative neoplasm leading to thickening and rigidity of the wall, and narrowing of the lumen.
50% middle third
Microscopically:
adenocarcinoma
Male:female 3:1.More common in whites.
Associated with Barrett esophagus.
Arise in the distal third of esophagus.
Gross:
Either flat, raised plaque like, large nodular masses, deeply ulcerative, or diffusely infiltrative features.
Microscopically:
Mucin- producing glandular tumors (intestinal type features).Clinical presentation and treatment of carcinoma:
Insidious onset, dysphagia, obstruction, weight loss, anorexia, weakness, and fatigue.
** surgical excision is rarely curative.???