
1
GASTROINTESTINAL TRACT
PROF.DR. MAHA SHAKIR HASAN
Lec.1
Esophagus
Lesions of the esophagus run the gamut from bland esophagitis
to highly lethal cancers, yet they evoke a similar and remarkably
limited range of symptoms. All produce dysphagia, Heartburn
(retrosternal burning pain). Hematemesis (vomiting of blood)
and melena (blood in the stools) are evidence of severe
inflammation, ulceration, or laceration of the esophageal
mucosa.
ANATOMIC AND MOTOR DISORDERS
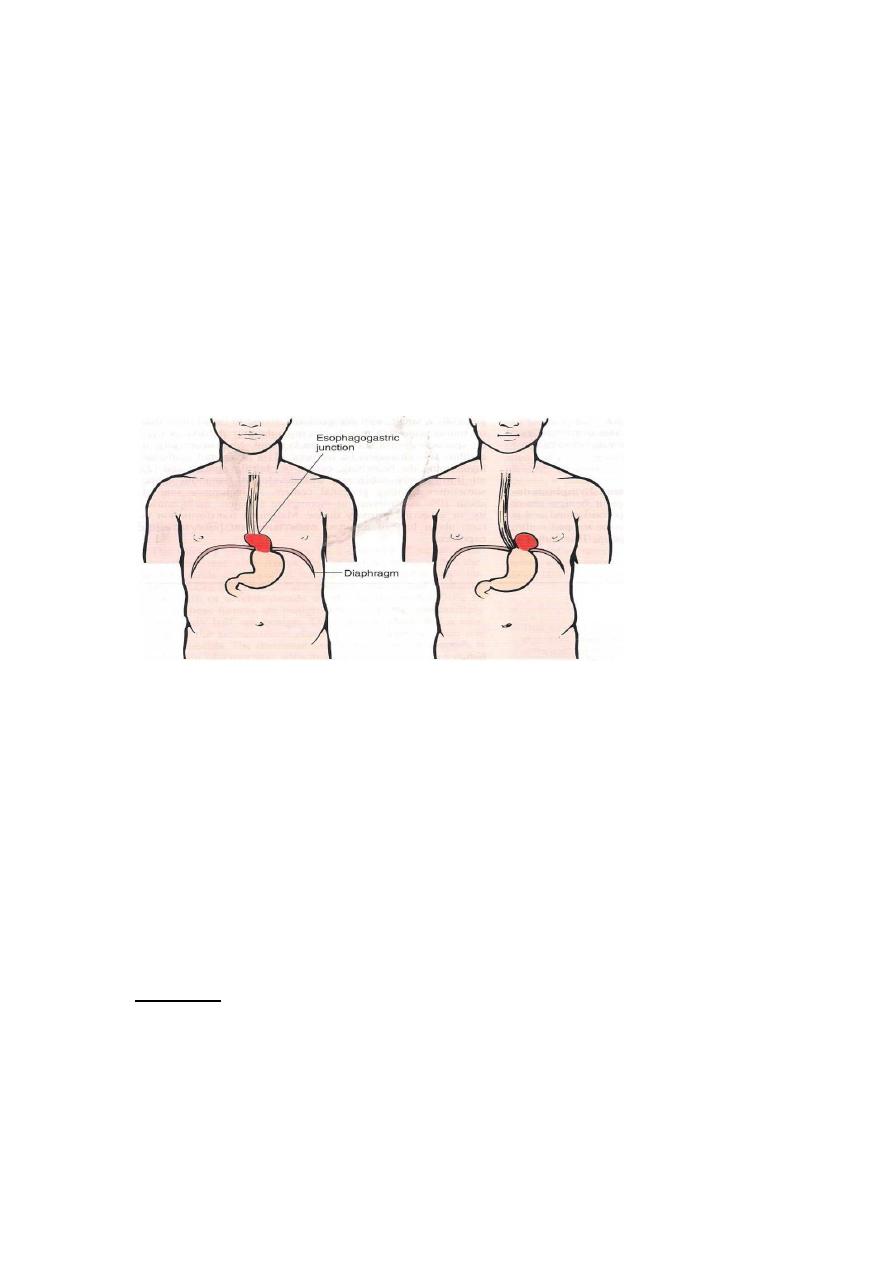
Hiatal hernia
In hiatal hernia, separation of the diaphragmatic crura and
widening of the space between the muscular crura and the
esophageal wall permits a dilated segment of the stomach to
protrude above the diaphragm. Two anatomic patterns are
recognized :
1- the axial, or sliding, hernia 2- the nonaxial, or
paraesophageal, hernia.
The sliding hernia constitutes 95% of cases; protrusion of the
stomach above the diaphragm creates a bell-shaped dilation,
bounded below by the diaphragmatic narrowing.
In paraesophageal hernias, a separate portion of the stomach,
usually along the greater curvature, enters the thorax through the
widened foramen.
2
The cause of this deranged anatomy is obscure. On the basis of
radiographic studies, hiatal hernias are reported in 1% to 20% of
adult subjects, increasing in incidence with age.
Clinical Presentation
Adult with progressive dysphagia to solids and eventually to all
foods; heartburn or regurgitation of gastric juices into the
mouth. These symptoms result from incompetence of the lower
esophageal sphincter.
Achalasia
The term achalasia means “failure to relax” and in the present context
denotes incomplete relaxation of the lower esophageal sphincter in
response to swallowing. This produces functional obstruction of the
esophagus, with consequent dilation of the more proximal esophagus.
Manometric studies show three major abnormalities in achalasia: (1)
aperistalsis, (2) partial or incomplete relaxation of the lower esophageal
sphincter with swallowing, and (3) increased resting tone of the lower
esophageal sphincter. It is now generally accepted that in primary
achalasia there is loss of intrinsic inhibitory innervation of the lower
esophageal sphincter and smooth muscle segment of the esophageal body.
Etiology
• Secondary achalasia may arise from pathologic processes that
impair esophageal function. The classic example is Chagas disease,
caused by Trypanosoma cruzi, which causes destruction of the
myenteric plexus of the esophagus, duodenum, colon, and ureter.

3
• primary disorder of uncertain etiology. Autoimmunity and
previous viral infection have been hypothesized but remain
unproven.
Morphology:
-In primary achalasia there is progressive dilation of esophagus above
the level of the lower esophageal sphincter.
-The wall of the esophagus may be of normal thickness thicker than
normal because of hypertrophy of the muscularis, or markedly thinned by
dilation.
-The myenteric ganglia are usually absent from the body of the
esophagus, Inflammation in the location of the esophageal myenteric
plexus is pathognomonic of the disease.
C/P :progressive dysphagia and inability to completely convey food to
the stomach. Nocturnal regurgitation and aspiration of undigested food
may occur. It usually becomes manifest in young adulthood, but it may
appear in infancy or childhood.
Complication:
is the hazard of developing esophageal squamous cell
carcinoma, reported to occur in about 5% of patients and typically at an
earlier age than in those without achalasia.
Lacerations (Mallory-Weiss Syndrome)
Definition: Longitudinal tears in the esophagus at the esophagogastric
junction.
Etiology: They are encountered in chronic alcoholics after a bout of
severe retching or vomiting, but they may also occur during acute
illnesses with severe vomiting.
pathogenesis :may be due to inadequate relaxation of the musculature of
the lower esophageal sphincter during vomiting, with stretching and
tearing of the esophagogastric junction at the moment of propulsive
expulsion of gastric contents.
Morphology: Tears may involve only the mucosa or may penetrate the
wall. Infection of the defect may lead to an inflammatory ulcer or to

4
mediastinitis.
Most often bleeding is not profuse and ceases without surgical
intervention, but life-threatening hematemesis may occur. Even with
severe blood loss, supportive therapy with vasoconstrictive medications,
transfusions, and sometimes balloon tamponade, is usually all that is
required. Healing is usually prompt, with minimal to no residua.
Varices
One of the few potential sites for communication between the intra-
abdominal splanchnic circulation and the systemic venous circulation is
through the esophagus. When portal Venous blood flow into the liver is
impeded by cirrhosis or other causes, the resultant portal hypertension
induces the formation of collateral bypass channels wherever the portal
and systemic systems communicate. The increased pressure in the
esophageal plexus produces dilated tortuous vessels called varices. They
are most often associated with alcoholic cirrhosis.
MORPHOLOGY
Varices appear primarily as tortuous dilated veins lying primarily within
the submucosa of the distal esophagus and proximal stomach.
-Varices produce no symptoms until they rupture.
Complications:
Rupture of varices.The factors leading to initial rupture
of a varix are unclear: silent erosion of overlying thinned mucosa,
increased tension in progressively dilated veins, and vomiting with
increased intra-abdominal pressure are likely to be involved.

5
Fig1:Esophageal varices: a view of the everted esophagus and gastroesophageal
junction, showing dilated submucosal veins (varices).
Esophagitis
• CHEMICAL AND INFECTIOUS ESOPHAGITIS
The stratified squamous mucosa of the esophagus may be damaged by a
variety of irritants including alcohol, corrosive acids or alkalis,
excessively hot fluids, and heavy smoking,
C/P:
Esophagitis due to chemical injury generally only dysphagia.
Hemorrhage, stricture, or perforation may occur in severe cases.
Infectious esophagitis may occur in otherwise healthy individuals but are
most frequent in those who are debilitated or immunosuppressed as a
result of disease or therapy.
• REFLUX ESOPHAGITIS
GE reflux disease affects about 0.5% is of the US adult population.
Dominant symptom recurrent heartburn.
Etiology:
• Decrease efficacy of esophageal antireflux mechanisms.
• Inadequate or slowed esophageal clearance of refluxed material.
• Sliding hiatal hernia.
• Increased gastric volume.
• Impaired reparative capacity of the esophagus mucosa by
prolonged exposure to gastric juices.
MORPHOLOGY
The anatomic Changes depend on the causative agent and on the
duration and severity of the exposure. Mild esophagitis may appear
macroscopically as simple hyperemia, with virtually no histologic
abnormality. In Contrast the mucosa in severe esophagitis exhibits
confluent epithelial erosions or total ulceration into the submucosa.
The histologic feature are characteristic of uncomplicated reflux
esophagitis is:
eosinophils, with or without neutrophils, in the epithelial layer.
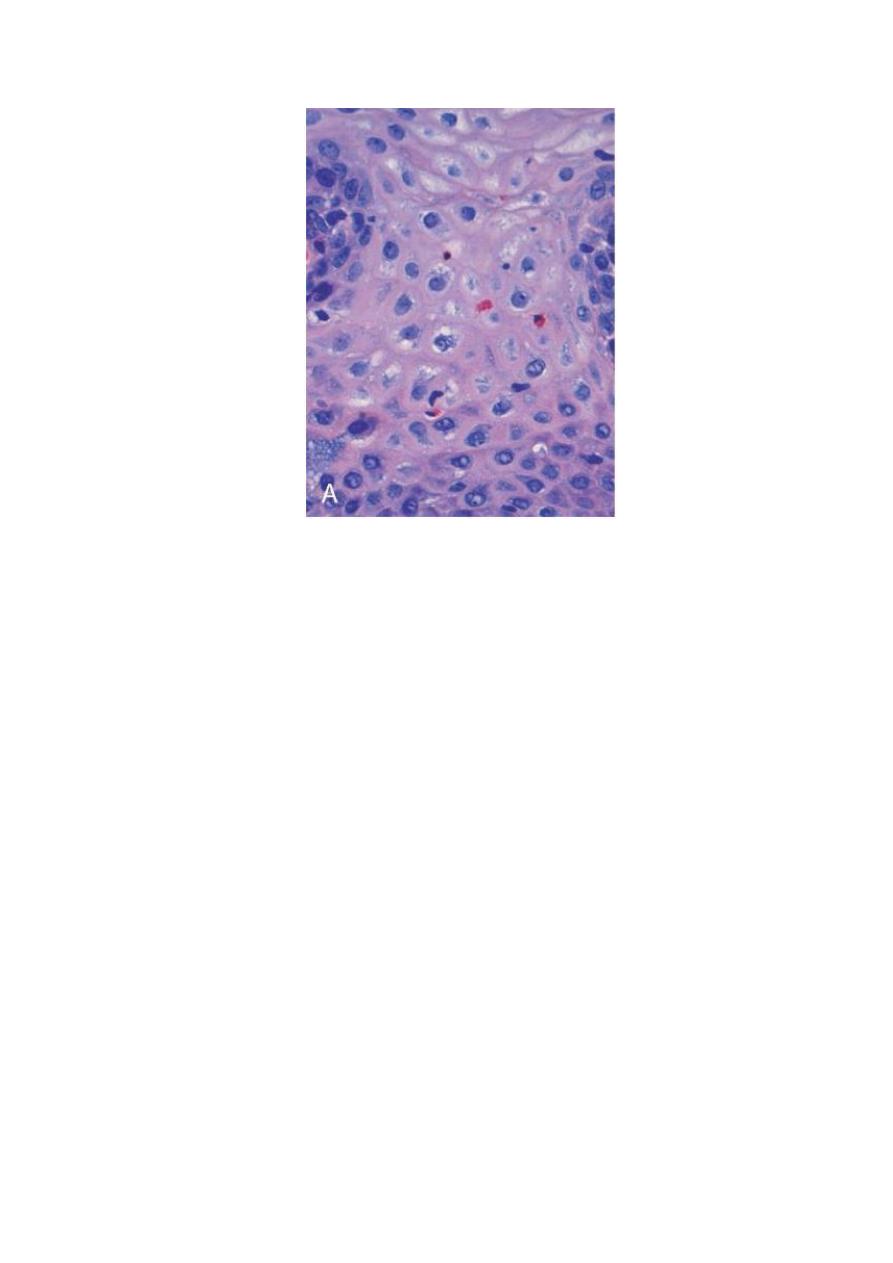
6
FIGURE Esophagitis. A, Reflux esophagitis with scattered intraepithelial eosinophils . squamous
cell maturation is relatively normal.
COMPLICATIONS
• BLEEDING
• STRICTURE
• BARRETT ESOPHAGUS
• PREDISPOSITION TO MALIGNANCY
,,
.
BARRETT ESOPHAGUS
Barrett esophagus is a complication of long-standing gastroesophageal
reflux, occurring in up to 10% of patients with persistent symptomatic
reflux disease, as well as in some patients with asymptomatic reflux.
Barrret esophagus is defined as the replacement of the normal distal
stratified squamous mucosa by metaplastic columnar epithelium
containing goblet cells.
Prolonged and recurrent gastroesophageal reflux is thought to produce
inflammation and eventually ulceration of the squamous epithelial lining
of lower esophags.
7
Healing occurs by in growth of stem cells and re-epithelialization. In the
microenvironment of an abnormally low pH in the distal esophagus
caused by acid reflux, the cells differentiate into columnar epithehum.
Metaplastic columnar epithelium is thought to be more resistant to injury
from refluxing gastric contents.
Barrett esophagus affects males more often than females (ratio of 4:1)
and is much more common in whites than in other races. Genetic factors
are suggested by clustering in families.
Ulcer and stricture may develop as a complication of Barrett esophagus.
However, the chief clinical significance of Barrett esophagus relates
to the development of adenocarcinoma. Patients with Barrett esophagus
have a 30 to 40 fold greater risk of developing esophageal
adenocarcinoma compared with normal populations.
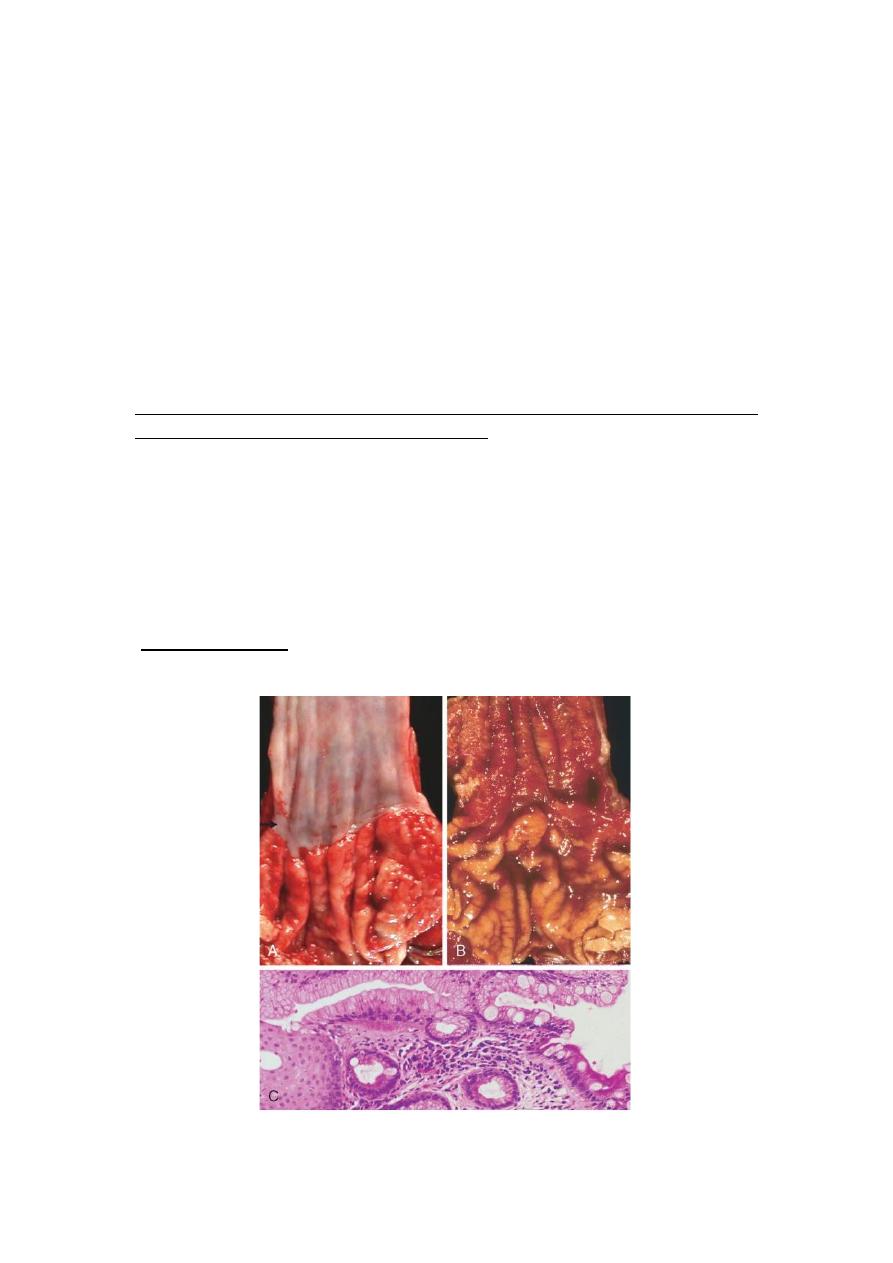
MORPHOLOGY
Barrett esophagus is apparent as a salmon-pink, velvety mucosa between
the smooth, pale pink esophageal squamous mucosa and the more light
brown gastric mucosa.
Microscopically, the esophageal squamous epithelium is replaced by
metaplastic columnar epithelium.

8
FIGURE
Barrett esophagus. A, Normal gastroesophageal junction. B, Barrett esophagus. Note the small
islands of paler squamous mucosa within the Barrett mucosa. C, Histologic appearance of the
gastroesophageal junction in Barrett esophagus. Note the transition between esophageal squamous
mucosa (left) and Barrett metaplasia, with abundant metaplastic goblet cells (right).
ESOPHAGEAL CARCINOMA
There are two types: squamous cell carcinomas and adenocarinomas.
Worldwide, squamous cell carcinomas constitute 90% of esophageal
cancers.
Adenocarcinoma arising in Barrett esophagus is more common in whites
than in blacks. By contrast, squamous cell carcinomas are more common
in blacks worldwide.
SQUAMOUS CELL CARCINOMA
Occurs in adults over age 45 and affects males four times more frequently
than females. It is nearly six fold more common in African-Americans
than Caucasians, a striking risk disparity that reflects differences in rates
of alcohol and tobacco use as well as other poorly understood factors.
Risk factors for SCC of the esophagus
1- Esophageal Disorders
a- Long-standing esophagitis
b- Achalasia
c- Plummer-Vinson syndrome (esophageal webs, microcytic
hypochromic anemia, atrophic glossitis)
2- Life Style
Alcohol consumption
Tobacco abuse
3- Dietary

9
Deficiency of vitamins (A, C, riboflavin, thiamine,
pyridoxine)
Deficiency of trace metals (zinc, molybdenum)
Fungal contamination of foodstuffs
High content of nitrites/nitrosamines
4- Genetic Pedisposition Tylosis
5-
Previous radiation therapy to the mediastinum also
predisposes individuals to esophageal carcinoma, typically
10 or more years after exposure.
There is a link between mentioned risk factors and
molecular changes;
* mutation of tumor suppressor gene P53
* mutation of k- RAS gene.
MORPHOLOGY
Squamous cell carcinomas are usually preceded by a long prodrome of
mucosal epithelial dysplasia followed by carcinoma in situ and,
ultimately, by the emergence of invasive cancer,
tumor masses may be
• polypoid or exophytic and protrude into and obstruct the lumen.
• Other tumors are either ulcerated or diffusely infiltrative lesions
that spread within the esophageal wall and cause thickening,
rigidity, and luminal narrowing.
These may invade surrounding structures including the respiratory
tree, causing pneumonia; the aorta, causing catastrophic
exsanguination; or the mediastinum and pericardium.
Half of squamous cell carcinomas occur in the middle third of the
esophagus
,
Symptomatic tumors are generally very large at
diagnosis and have already invaded the esophageal wall. The rich

10
submucosal lymphatic network promotes circumferential and
longitudinal spread.
Clinical Features.
dysphagia, odynophagia (pain on swallowing), and obstruction.
Patients subconsciously adjust to the progressively increasing
obstruction by altering their diet from solid to liquid foods.
Extreme weight loss and debilitation result from both impaired
nutrition and effects of the tumor itself. Hemorrhage and sepsis
may accompany tumor ulceration.
Adenocarcinomas
appear to arise from dysplastic mucosa in the setting of Barrett
esophagus. Unlike squamous cell carcinomas, they are usually in the
distal one third of the esophagus and may invade the subjacent gastric
cardia.
Microscopically, most tumors are mucin-producing glandular tumors
exhibiting intestinal-type features, in keeping with the morphology of the
preexisting metaplastic
mucosa.
Diagnosis
is usually made by imaging techniques and endoscopic biopsy.
Because these cancers extensively invade the rich esophageal lymphatic
network and adjacent structures, surgical excision rarely is curative.
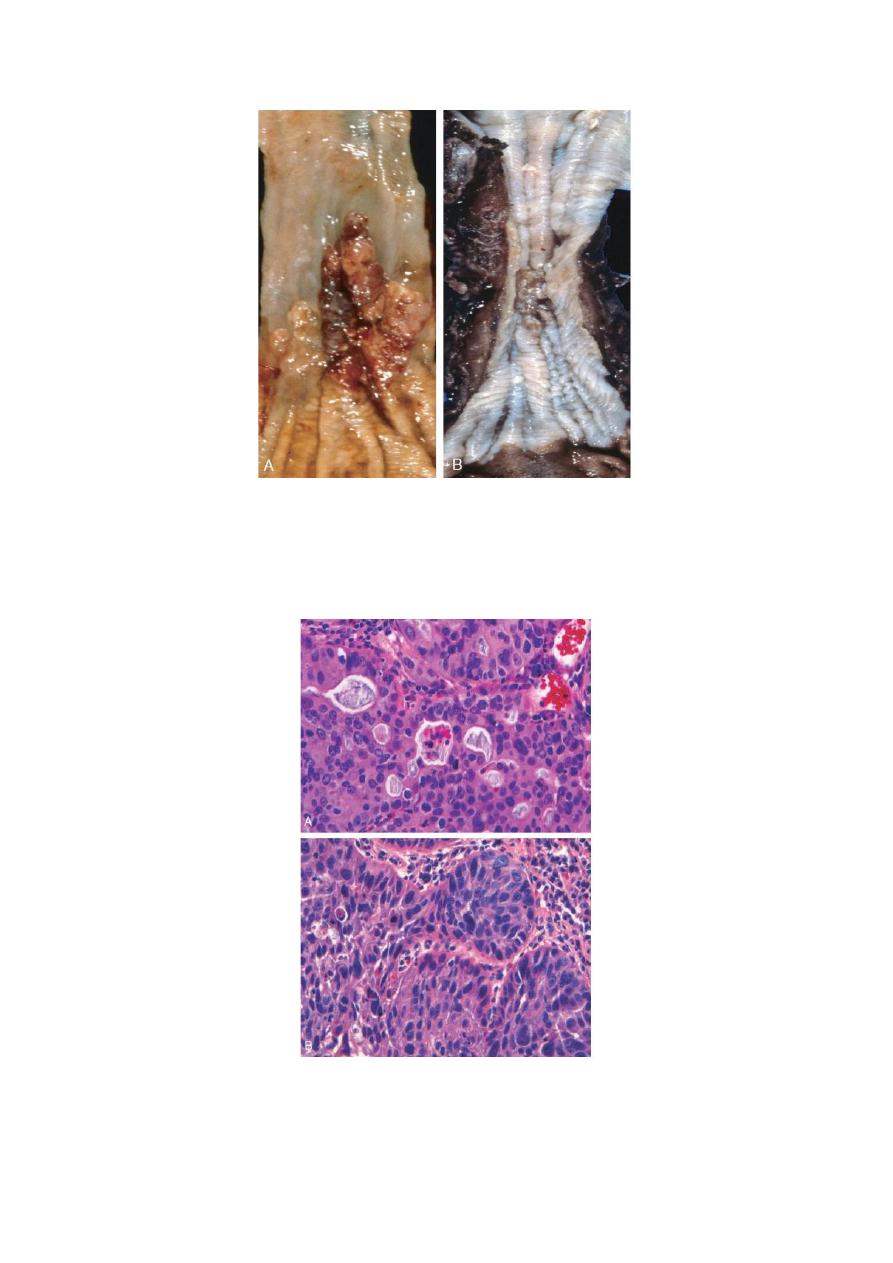
11
FIGURE Esophageal cancer. A, Adenocarcinoma usually occurs distally and, as in this case, often
involves the gastric cardia. B, Squamous cell carcinoma is most frequently found in the mid-esophagus,
where it commonly causes strictures.
FIGURE Esophageal cancer. A, Esophageal adenocarcinoma organized into back-to-back glands. B,
Squamous cell carcinoma composed of nests of malignant cells that partially recapitulate the
organization of squamous epithelium.