
Mood Disorders (Affective disorders) 3Hours
A group of psychiatric disorders in which pathological moods and related
vegetative and psychomotor disturbances dominate the clinical picture.
It refers to sustained emotional states, not merely to the external
(affective) expression of the present emotional state, sustained over a
period of weeks to months, often in periodic or cyclical fashion.
Depressive disorders afflict at least 20 percent of women and 12 percent
of men at some time during their lives. Despite the availability of
effective treatments, many persons with mood disorders are disabled, and
rates of suicide (which occurs in about 15 percent of depressive
disorders) are high in both young and (especially) elderly men. Although
depressive disorders are more common in women, more men than women
die of suicide.
Major Depressive Disorder and Bipolar Disorder:
Major depressive disorder (unipolar depression) is reported to be the
most common mood disorder. It may manifest as a single episode or as
recurrent episodes. The course may be up to 2 years or longer—in those
with the single-episode form. Whereas the prognosis for recovery from an
acute episode is good for most patients with major depressive disorder,
three out of four patients experience recurrences throughout life.
Bipolar disorders (previously called manic-depressive psychosis) consist
of at least one hypomanic, manic, or mixed episode. Mixed episodes
represent a simultaneous mixture of depressive and manic or hypomanic
manifestations. Although a minority of patients experience only manic
episodes, most bipolar disorder patients experience episodes of both
polarity. Manias predominate in men, depression and mixed states in
women.
Recent clinical studies have shown the existence of a spectrum of
ambulatory depressive states that alternate with milder, short-lived
periods of hypomania rather than full-blown mania (bipolar II disorder).
Mood Disorders
Major depressive disorder: characterized by one or more major
depressive episodes (at least 2 weeks of depressed mood or loss of
interest accompanied by at least four additional symptoms of depression,
see later).

Dysthymic disorder: characterized by at least 2 years of depressed
mood for more days than not, accompanied by additional depressive
symptoms that do not meet criteria for major depressive episode.
Bipolar I disorder: characterized by one or more manic or mixed
episodes, usually accompanied by major depressive episodes.
Bipolar II disorder: characterized by one or more major depressive
episodes accompanied by at least one hypomanic episode.
Cyclothymic disorder: characterized by at least 2 years of numerous
periods of hypomanic symptoms that do not meet criteria for a manic
episode, and numerous periods of depressive symptoms that do not meet
criteria for a major depressive episode.
Mood disorder due to general medical condition: characterized by a
prominent and persistent disturbance in mood that is judged to be a direct
physiological consequence of a general medical condition.
Substance-induced mood disorder: characterized by prominent and
persistent disturbance in mood that is judged to be a direct physiological
consequence of a drug of abuse, toxin exposure, or a medication.
MAJOR DEPRESSIVE DISORDERS
- Clinical features vary in nature and severity from patient to patient.
- The following list of features is not necessarily to be present in all
patients.
A. Mood (Affective) Changes:
Feeling low (more severe than ordinary sadness).
Lack of enjoyment and inability to experience pleasure (anhedonia).
Irritability.
Frustration.
Tension.
B. Appearance & Behaviour:
Neglected dress and grooming.
Facial appearance of sadness:
- turning downwards of corners of mouth.
- down cast gaze.
- tearful eyes.
- reduced rate of blinking.
- head is inclined forwards.

Psychomotor retardation (sometimes agitation).
- lack of motivation and irritation.
- slow movements.
- slow interactions.
Social isolation and withdrawal.
Delay of tasks and decisions.
Loss of interest in work and pleasure activities.
C. Biological Features (Neurovegetative Signs):
Change in appetite (usually reduced but in some patients increased).
Change in sleep (usually reduced but in some patients increased).
Early morning (terminal) insomnia; waking 2 - 3 hours before the usual
time, this is usually associated with severe depression.
Change in weight (usually reduce but may be increased).
Fatigability, low energy level, (simple task is an effort)
Low libido and /or impotence.
Change in bowel habit (usually constipation).
Change in menstrual cycle (amenorrhoea).
Diurnal variation of mood (usually worse in the morning).
D. Cognitive Functions & Thinking:
Poor attention and concentration.
Poor memory (subjective).
Pessimistic thoughts; depressive cognitions as suggested by Beck:
- Present: patient sees the unhappy side of every event (discounts any
success in life, no longer feels confident, sees himself as failure).
- Past: unjustifiable guilt feeling and self-blame.
-Future: gloomy preoccupations; hopelessness, helplessness, death wishes
( may progress to suicidal ideation and attempt ).
Psychotic Features Associated with Severe Depression
A. Delusions (mood-congruent)
1. Delusion of guilt (patient believes he deserves severe punishment).
2. Nihilistic delusion (patient believes that some part of his body ceased
to exist or function, e.g. bowel, brain…).
3. Delusion of poverty and impoverishment.
4. Persecutory delusion (patient accepts the supposed persecution as
something he deserves, in contrast to schizophrenic patient).

B. Hallucinations (mood-congruent)
1. Usually second person auditory hallucinations (addressing derogatory
repetitive phrases).
2. Visual hallucinations (scenes of death and destruction) may be
experienced by a few patients.
Epidemiology of Major Depression
It is more prevalent than bipolar mood disorder (more in women).
Lifetime prevalence is in the range of 15 - 25 %.
The mean age of onset is about 40 years (25 - 50 years).
It may occur in childhood or in the elderly.
In adolescents may be precipitated by substance abuse.
More common in those who lack confiding relationship (e.g. divorced,
separated, single…).
No correlation has been found between socio - economic status and
major depressive disorder.
Etiology of Major Depression:
The causative factors are multifactorial (interacting together)
A-GENETIC FACTORS :as supported by family and twin studies.
B-- BIOLOGICAL FACTORS
Reduced levels of:
Noradrenaline
Serotonin
Dopamine
C-PSYCHOLOGICAL FACTORS
Stressful events
Premorbid personality factors
Cognitive faults (distortions)
Differential Diagnosis of Major Depression :
Depression secondary to medical diseases: - Thyroid dysfunction. -
Diabetes mellitus. - Cushing’s disease. - Parkinson’s disease. - Stroke. -
Carcinoma (especially of the pancreas and lung). - Multiple sclerosis.
Depression secondary to medications:
- Antihypertensives (resepine, beta-blockers). - Corticosteroids.
- Antineoplastic drugs.
- Bromocriptine.
- Indomethacin.
- L - dopa.
Psychiatric disorders:
Dysthymic disorder (less severe, and chronic).
Adjustment disorder with depressed mood.
Substance - induced mood disorder.
Schizophrenia, schizoaffective disorder.
Somatization disorder
DSM-V Criteria for Major Depressive Episode
A. Five (or more) of the following symptoms have been present during
the same 2- week period and represent a change from previous
functioning; at least one of the symptoms is either (1) depressed mood or
(2) loss of interest or pleasure.
Note: Do not include symptoms that are clearly attributable to another
medical condition.
1. Depressed mood most of the day, nearly every day, as indicated by
either subjective report (e.g., feels sad, empty, hopeless) or observation
made by others (e.g., appears tearful). (Note: In children and adolescents,
can be irritable mood.)
2. Markedly diminished interest or pleasure in all, or almost all, activities
most of the day, nearly every day (as indicated by either subjective
account or observation).
3. Significant weight loss when not dieting or weight gain (e.g., a change
of more than 5% of body weight in a month), or decrease or increase in
appetite nearly every day. (Note: In children, consider failure to make
expected weight gain.)
4. Insomnia or hypersomnia nearly every day.
5. Psychomotor agitation or retardation nearly every day (observable by
others, not merely subjective feelings of restlessness or being slowed
down).
6. Fatigue or loss of energy nearly every day.
7. Feelings of worthlessness or excessive or inappropriate guilt (which
may be delusional) nearly every day (not merely self-reproach or guilt
about being sick).
8. Diminished ability to think or concentrate, or indecisiveness, nearly
every day (either by subjective account or as observed by others).
9. Recurrent thoughts of death (not just fear of dying), recurrent suicidal
ideation without a specific plan, or a suicide attempt or a specific plan for
committing suicide.
B. The symptoms cause clinically significant distress or impairment in
social, occupational, or other important areas of functioning.
C. The episode is not attributable to the physiological effects of a
substance or to another medical condition.
Note: Criteria A–C represent a major depressive episode.
D. The occurrence of the major depressive episode is not better explained
by schizoaffective disorder, schizophrenia, schizophreniform disorder,
delusional disorder, or other specified and unspecified schizophrenia
spectrum and other psychotic disorders.
E. There has never been a manic episode or a hypomanic episode.
Note: This exclusion does not apply if all of the manic-like or
hypomanic-like episodes are substance-induced or are attributable to the
physiological effects of another medical condition.
PSYCHOMOTOR RETARDATION
(1) Paucity of spontaneous movements
(2) Slumped posture with downcast gaze
(3 )fatigue
(4) Reduced flow and amplitude of speech
(5) Poor concentration and forgetfulness.
(6) Inability to make simple decisions.
Management of Major Depression:
Treatment of Depression
A Strategic map for managing mood disorders,
(1) Symptom remission (acute phase) and restoration of psychosocial
functioning (acute and continuation phases).
(2) Prevention of a relapse (continuation phase).
(3) Prevention of recurrences, or new episodes in patients with recurrent
depressions (maintenance phase).
Hospitalization is indicated for: Suicidal or homicidal patient.
- Patient with severe psychomotor retardation who is not eating or
drinking (for ECT).
- Diagnostic purpose (observation, investigation…).
- Drug resistant cases (possible ECT).
- Severe depression with psychotic features (possible ECT).
Medications have proven to be very useful in the treatment of severe
depression. They shorten the duration in most cases.
-Antidepressants.
-Tricyclics / Tetracyclics .
- Monoamino oxidase inhibitors (MAOI) .
-Selective serotonin reuptake inhibitors (SSRIs) .
-Others (new agents)
- Desirable therapeutic antidepressant effect requires a period of time,
usually 3-6 weeks. (Side effects may appear within the first few days.)
- After a first episode of a unipolar major depression, treatment should be
continued for six months after clinical recovery, to reduce the rate of
relapse.
- If the patient has had two or more episodes, treatment should be
prolonged for at least a year after clinical recovery to reduce the risk of
relapse.
- Lithium Carbonate can be used as prophylaxis.
Electroconvulsive therapy ( ECT ):
Psychosocial:
Treatment of Depression
A- Psychotherapy:
- Supportive therapy.
- Family therapy.
- Cognitive-behavior therapy (for less severe cases or after
improvement with medication).
B- ELECTROCONVULSIVE THERAPY(ECT):
The effect of ECT is best in severe depression especially with marked
biological (neurovegetative) and psychotic features. . It is mainly the
speed of action that distinguishes ECT from antidepressant drug
treatment. Despite many of the largely societal criticisms of the modern
use of ECT, this modality should be given a higher priority when treating
patients with extreme suicidality, associated medical illnesses, difficult
adverse reactions to routine psychopharmacological agents, or other
medical emergency situations (such as catatonia) that demand the most
rapid treatment response available.
ECT is effective, even in patients who have failed to respond to one or
more medications or combined treatment. It is effective in both psychotic
and nonpsychotic forms of depression. Usually, 8 to 12 treatments are
needed.
C- Light therapy has been most clearly evaluated in mood disorder
with seasonal pattern, either as monotherapy or in combination
with medication. Patients who respond do so within 2 to 4 weeks.
D-Antidepressant Medications;
1-Tricyclic anti depressant:
a-Amitriptyline (Tryptizol) 75–250mg/day
side effect: Sedative
,increase appetite ,Drowsiness, Orthostatic hypotension, Cardiac
arrhythmia, weight gain, anticholinergic effect (Dry mouth, blurred
vision, urinary hesitancy, constipation.), Overdose may be fatal.

b- Clomipramine (Anafranil): dose 75–250 mg Drowsiness,
weight
gain.
c- Imipramine (Tofranil) 75–250 mg, Sedative ,increase appetite
Drowsiness, Orthostatic hypotension, Cardiac arrhythmia, weight gain,
anticholinergic effect (Dry mouth, blurred vision, urinary hesitancy,
constipation.), Overdose may be fatal.
2-Tetracyclic anti depressant:
Maprotiline (Ludiomil):75–225mg; Drowsiness, weight gain, lower
than tricyclics anticholinergic effect (Dry mouth, blurred vision, urinary
hesitancy, constipation.), Overdose may be fatal.
3-Mono Amine Oxidize Inhibitor (MAOI):
- Irreversible
Phenelzine ( Nardil )
Tranylcypramine ( Parnate )
Isocarboxazid ( Marplan )
- Reversible
Moclobemide ( Aurorix )
MAOI have serious side effect with High Tyramine Content Diet and
when combined with other anti depressant (Hypertensive crises).
4-SelectivSerotinine Reuptake Inhibitor(SSRI):
a- Fluoxetine (Prozac) 20–80mg
b- Paroxetine (Paxil ,Seroxat) 10–60mg
c- Sertraline (Zoloft) 50–200 mg
d- Fluvoxamine ( Faverin ) 50-300mg
* All SSRIs may cause agitation, sedation, GI distress, sexual
dysfunction
5-
Other antidepressants:
Trazodone ( Trazolan )
Venlafaxine ( Effexor )
Mirtazapine ( Remeron )
Nefazodone ( Serzone )
Prognosis of Unipolar Depressive Disorders
- About 25 % of patients have a recurrence within a year.
- Ten percent will eventually develop a manic episode.
- A group of patients have chronic course with residual symptoms and
significant social handicap.
DSM-V Diagnostic Criteria for Dysthymic Disorder
A. Depressed mood for most of the day, for more days than not, as
indicated by either subjective account or observation by others, for at
least 2 years.
Note: In children and adolescents, mood can be irritable and duration
must be at least 1 year.
B. Presence, while depressed, of two (or more) of the following:
1. Poor appetite or overeating.
2. Insomnia or hypersomnia.
3. Low energy or fatigue.
4. Low self-esteem.
5. Poor concentration or difficulty making decisions.
6. Feelings of hopelessness.
C. During the 2-year period (1 year for children or adolescents) of the
disturbance, the individual has never been without the symptoms in
Criteria A and B for more than 2 months at a time.
D. Criteria for a major depressive disorder may be continuously present
for 2 years.
E. There has never been a manic episode or a hypomanic episode, and
criteria have never been met for cyclothymic disorder.
F. The disturbance is not better explained by a persistent schizoaffective
disorder, schizophrenia, delusional disorder, or other specified or
unspecified schizophrenia spectrum and other psychotic disorder.
G. The symptoms are not attributable to the physiological effects of a
substance (e.g., a drug of abuse, a medication) or another medical
condition (e.g., hypothyroidism).
H. The symptoms cause clinically significant distress or impairment in
social, occupational, or other important areas of functioning.
Note: Because the criteria for a major depressive episode include four
symptoms that are absent from the symptom list for persistent depressive
disorder (dysthymia), a very limited number of individuals will have
depressive symptoms that have persisted longer than 2 years but will not
meet criteria for persistent depressive disorder. If full criteria for a major
depressive episode have been met at some point during the current
episode of illness, they should be given a diagnosis of major depressive
disorder. Otherwise, a diagnosis of other specified depressive disorder or
unspecified depressive disorder is warranted.
DSM-V Criteria for Manic Episode
For a diagnosis of bipolar I disorder, it is necessary to meet the following
criteria for a manic episode. The manic episode may have been preceded
by and may be followed by hypomanic or major depressive episodes.
A. A distinct period of abnormally and persistently elevated, expansive,
or irritable mood and abnormally and persistently increased activity or
energy, lasting at least 1 week and present most of the day, nearly every
day (or any duration if hospitalization is necessary).
B. During the period of mood disturbance and increased energy or
activity, three (or more) of the following symptoms (four if the mood is
only irritable) are present to a significant degree and represent a
noticeable change from usual behavior:
1. Inflated self-esteem or grandiosity.
2. Decreased need for sleep (e.g., feels rested after only 3 hours of sleep).
3. More talkative than usual or pressure to keep talking.
4. Flight of ideas or subjective experience that thoughts are racing.
5. Distractibility (i.e., attention too easily drawn to unimportant or
irrelevant external stimuli), as reported or observed.
6. Increase in goal-directed activity (either socially, at work or school, or
sexually) or psychomotor agitation (i.e., purposeless non-goal-directed
activity).
7. Excessive involvement in activities that have a high potential for
painful consequences (e.g., engaging in unrestrained buying sprees,
sexual indiscretions, or foolish business investments).
C. The mood disturbance is sufficiently severe to cause marked
impairment in social or occupational functioning or to necessitate
hospitalization to prevent harm to self or others, or there are psychotic
features.
D. The episode is not attributable to the physiological effects of a
substance (e.g., a drug of abuse, a medication, other treatment) or to
another medical condition.
Note: A full manic episode that emerges during antidepressant treatment
(e.g., medication, electroconvulsive therapy) but persists at a fully
syndromal level beyond the physiological effect of that treatment is
sufficient evidence for a manic episode and, therefore, a bipolar I
diagnosis.
Note: Criteria A–D constitutes a manic episode. At least one lifetime
manic episode is required for the diagnosis of bipolar I disorder.
Hypomanic Episode
The criteria for hypomanic episode describe a mild form of mania that
may be seen either in the course of bipolar I disorder or as a regular part
of bipolar II disorder.
Diagnostic Criteria for Hypomanic Episode
A. A distinct period of abnormally and persistently elevated, expansive,
or irritable mood and abnormally and persistently increased activity or
energy, lasting at least 4 consecutive days and present most of the day,
nearly every day.
B. During the period of mood disturbance and increased energy and
activity, three (or more) of the following symptoms (four if the mood is
only irritable) have persisted, represent a noticeable change from usual
behavior, and have been present to a significant degree:
1. Inflated self-esteem or grandiosity.
2. Decreased need for sleep (e.g., feels rested after only 3 hours of sleep).
3. More talkative than usual or pressure to keep talking.
4. Flight of ideas or subjective experience that thoughts are racing.
5. Distractibility (i.e., attention too easily drawn to unimportant or
irrelevant external stimuli), as reported or observed.
6. Increase in goal-directed activity (either socially, at work or school, or
sexually) or psychomotor agitation.
7. Excessive involvement in activities that have a high potential for
painful consequences (e.g., engaging in unrestrained buying sprees,
sexual indiscretions, or foolish business investments).
C. The episode is associated with an unequivocal change in functioning
that is uncharacteristic of the individual when not symptomatic.
D. The disturbance in mood and the change in functioning are observable
by others.
E. The episode is not severe enough to cause marked impairment in social
or occupational functioning or to necessitate hospitalization. If there are
psychotic features, the episode is, by definition, manic.
F. The episode is not attributable to the physiological effects of a
substance (e.g., a drug of abuse, a medication, other treatment).
Note: A full hypomanic episode that emerges during antidepressant
treatment (e.g., medication, electroconvulsive therapy) but persists at a
fully syndromal level beyond the physiological effect of that treatment is
sufficient evidence for a hypomanic episode diagnosis. However, caution
is indicated so that one or two symptoms (particularly increased
irritability, edginess, or agitation following antidepressant use) are
not taken as sufficient for diagnosis of a hypomanic episode, nor
necessarily indicative of a bipolar diathesis.
Note: Criteria A–F constitute a hypomanic episode. Hypomanic episodes
are common in bipolar I disorder but are not required for the diagnosis of
bipolar I disorder.
DSM-V Diagnostic Criteria for Cyclothymic Disorder
A. For at least 2 years (at least 1 year in children and adolescents) there
have been numerous periods with hypomanic symptoms that do not meet
criteria for a hypomanic episode and numerous periods with depressive
symptoms that do not meet criteria for a major depressive episode.
B. During the above 2-year period (1 year in children and adolescents),
the hypomanic and depressive periods have been present for at least half
the time and the individual has not been without the symptoms for more
than 2 months at a time.
C. Criteria for a major depressive, manic, or hypomanic episode have
never been met.
D. The symptoms in Criterion A are not better explained by
schizoaffective disorder, schizophrenia, schizophreniform disorder,
delusional disorder, or other specified or unspecified schizophrenia
spectrum and other psychotic disorder.
E. The symptoms are not attributable to the physiological effects of a
substance (e.g., a drug of abuse, a medication) or another medical
condition (e.g., hyperthyroidism).
F. The symptoms cause clinically significant distress or impairment in
social, occupational, or other important areas of functioning.
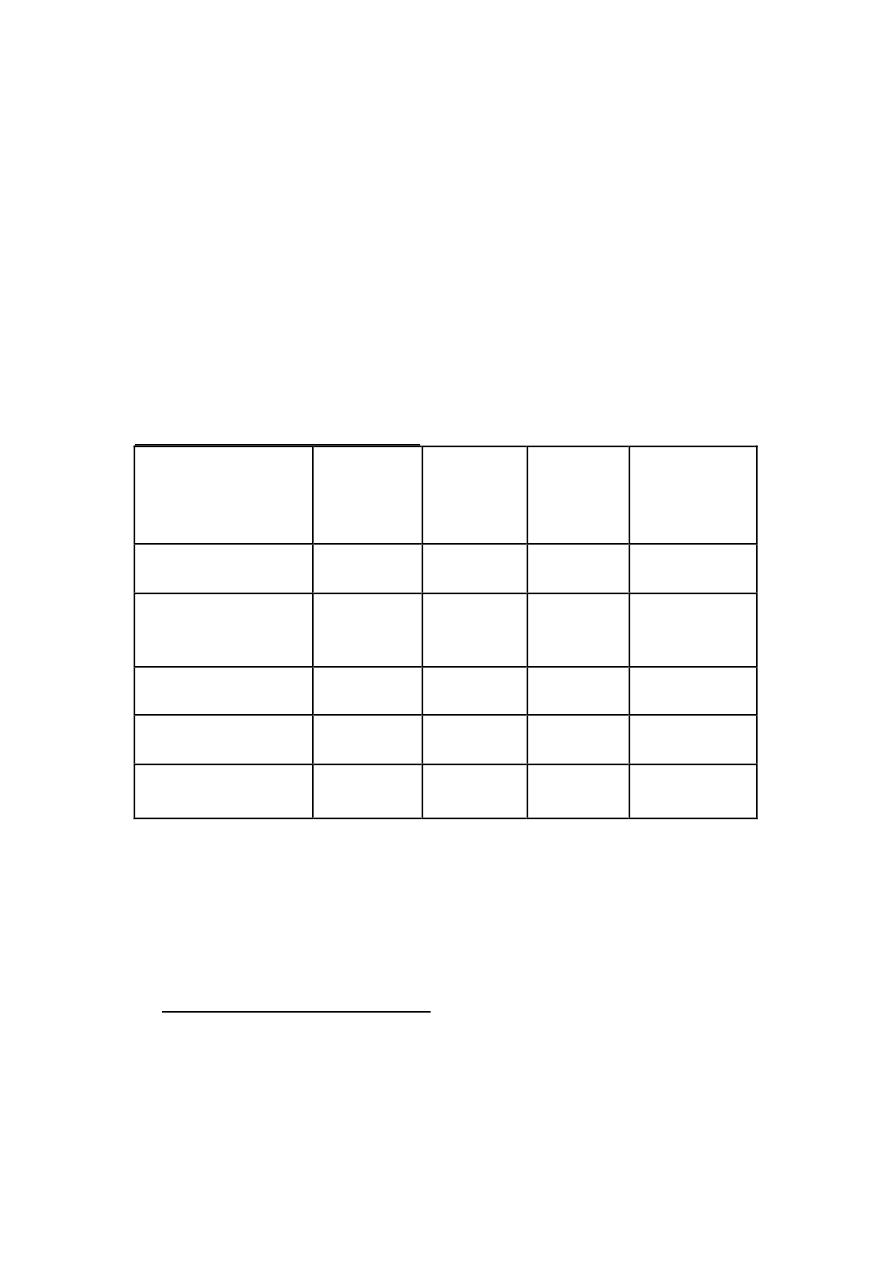
Differentiation of Mood disorders
Diagnoses
MDE
Milder
depression
Manic or
Mixed
episode
Hypomania
MDE
+
+
--
--
--
Dysthymic
disorder
--?
+
--
--
Bipolar I disorder
+
--
+
--
+
+
--
Bipolar II disorder +
--
+
--
--
+
Cyclothymia
--
+
--?
+
n
+most be present to make the diagnoses
n
--most be absent to make the diagnoses
n
? most not occur during the first 2 years of the illness
Treatment of Bipolar disorders
Hospitalization is often indicated for the acutely suicidal or dangerous
patient on self or on the others; or patient how show gross disorganized
behavior and may also be considered for the patient with associated
medical problems.

Treatment of mania (Mood stabilizers):
Lithium
Lithium has been the main line of treatment for acute and prophylactic
treatment of mania. In comparative studies with antipsychotic agents, it
yields better overall improvement in most aspects of manic
symptomatology, including psychomotor activity, grandiosity, manic
thought disorder, insomnia, and irritability. However, the onset of
antimanic action with lithium can be rather slow (2week), even with
aggressive dosing. Until recently, this was traditionally accomplished
with the typical neuroleptic drugs, including the phenothiazines, or
butyrophenones such as haloperidol (Haldol).
Lithium doses; should be administered to achieve concentrations in
serum between 0.6 and 1.2 mEq per liter.
High serum level (1.5 mEq per liter) can lead to toxicity: seizures,
confusion, coma and cardiac dysrhythmia. In sever overdose dialyses is
effective.
In bipolar disorders the high likelihood of relapse (50 percent in the
first 5 months following lithium discontinuation and 80 to 90 percent
within the first year and a half), and this should be explained to the
patient.
Valproic Acid:
200-3000 mg/day
As effective as lithium in treating bipolar illness, may be more
effective in treating mixed episode while lithium is more effective in
treating traditional mania.
It is also used as prophylactic agent especially in rapid cycling cases.
Carbamazepine:
200-1800 mg/day
effective in acute mania , bipolar depression and as prophylactic
agent.
Because of the rapidly growing evidence for the parallel acute
antimanic efficacy of the mood-stabilizing anticonvulsants
carbamazepine and valproic acid, it is suggested that these alternative
agents be used as initial treatment.
ECT: may be used to treat booth phase of bipolar disorder.

Treatment of Dysthymia and Cyclothymia:
1- Dysthymia:
Traditionally treated with psychotherapy (cognitive and behavioral
therapy). SSRI and MAOI are more effective than the tricyclic
antidepressant.
2- Cyclothymia:
Treated with mood stabilizers and supportive psychotherapy.